Patient and tumor characteristics
We reviewed 32 cases with 41 non-central lesions of pelvic recurrent cervical cancer after external beam radiotherapy in which brachytherapy was performed at our institution between June 2015 and April 2022. The confirmation of recurrence was mostly based on imaging examination(CT、MRI、PETCT) and examination of tumor markers or biopsy.The patient and tumor characteristics are summarized in Table 1.Patients treated with standard chemoradiotherapy were treated with previous treatments, and patients treated with concurrent chemoradiotherapy were given doses of 45(40 to 50)Gy. Unresectable lymph nodes can be treated with a simultaneous dose or a delayed dose of 10 to 15 Gy by highly conformal radiotherapy. 192 Ir as part of initial treatment, A point A or high risk CTV(HR-CTV)is prescribed at a dose of (5 to 7)Gy(4 to 6) times for a total of 20 to 35 Gy. Only 2 of the 32 patients did not receive chemotherapy after brachytherapy because of abnormal liver and kidney function.Based on the protocol followed at our hospital, the indications for 125I seed brachytherapy were as follows: (1) non-central pelvic recurrent cervical cancer after external beam radiotherapy, (2) the presence of metastatic lesions that are determined to be inoperable or unresectable by an experienced gynecologist; (3) blood routine results showing a white blood cell count of ≥ 3 × 109/L, a neutrophil absolute value of > 1.5 × 109, a platelet count of ≥ 75 × 1012/L, a hemoglobin concentration of ≥ 90 g/L, and normal coagulation function; (4) a Karnofsky performance score (KPS) of 70 or higher; (5) expected survival of ≥ 3 months and (6) no major organ dysfunction. The exclusion criteria were (1) major organ dysfunction, such as severe heart, lung, liver, and kidney dysfunction; (2) severe coagulation disorder; (3) poor general condition or bad fluid quality with acute or chronic infections; and (4) less than 3 months since the end of the last external radiotherapy. All the included patients provided their written informed consent, and this study received the approval of the Institutional Review Board. Our multidisciplinary team discussed the decision to administer brachytherapy.
Table 1 Patient and tumor characteristicsPreoperative planning
One week before implantation, the patients were immobilized with a vacuum cushion in the treatment position. A position line was drawn along the CT positioning laser line on the surface of the patient’s skin around the tumor location, and three to four markers were pasted on the horizontal line. Then, enhanced CT scanning was performed with a slice thickness of 5 mm. Next, the Prowess treatment planning system (TPS) (Panther Brachy version 5.0 TPS; Prowess Inc., Concord, CA, USA) was used to create a Brachy Stereo–Seed preplan. During the pre-planning with the TPS, the gross target volume (GTV) is the location and extent of tumor confirmed by imaging examination (CT, MRI, PET-CT, etc.)and the organ at risk (OAR) were delineated, but the clinical target volume (CTV) was obtained by expanding the GTV by 5 mm in all directions. The organs at risk (OAR)are mainly intestine, bladder, ureter, etc., and the dose is converted into particle dose by BED and EQD2, referring to the dose of external radiotherapy.The delineations were carefully done following the CT images, and the volume of the CTV influenced the choice of seed activity (0.3–0.7 mCi). The needles were implanted, and the seeds were loaded according to a pre-plan for a patient. The median prescription dose was 100 Gy (range, 80–120 Gy), which was determined by the conversion of BED and EQD2 according to the specific organ at risk, the dose of radiotherapy and the time between radiotherapy. Finally, a dose–volume histogram was generated. A 3D template was printed with a sla600 type 3D printer (Unicorn 3DSL450M; Beijing Unicorn Science and Technology Ltd., Beijing, China) according to the biological surface characteristics of the seed implantation area, the X-axis and Y-axis laser lines, a registration mark, and information about the simulated needle path.
Brachytherapy protocol
The patients were fixed in the same position as the preplanning stage with a vacuum cushion. Surgery was carried out with the patients under anesthesia induced by local infiltration or nerve block, and the CT positioning scan was used to select the puncture points and determine the angle and depth of the puncture path. Single-use needles were inserted into the target lesion under CT guidance by using a freehand implantation technique or a 3D-printed template, with a distance of 0.5–1.0 cm between seeds and a distance of 1 cm between needles. A CT scan was obtained to confirm that the template location was correct, and then a Mick applicator was used to implant seeds according to the preoperative plan.After seed implantation, CT was performed again to view the actual distribution of the 125I seeds in the target areas, and additional seeds were implanted if the 125I seeds were not adequately distributed within the target volume.Finally, the images were transferred into the TPS to verify the dose distribution.
End-points and follow-up
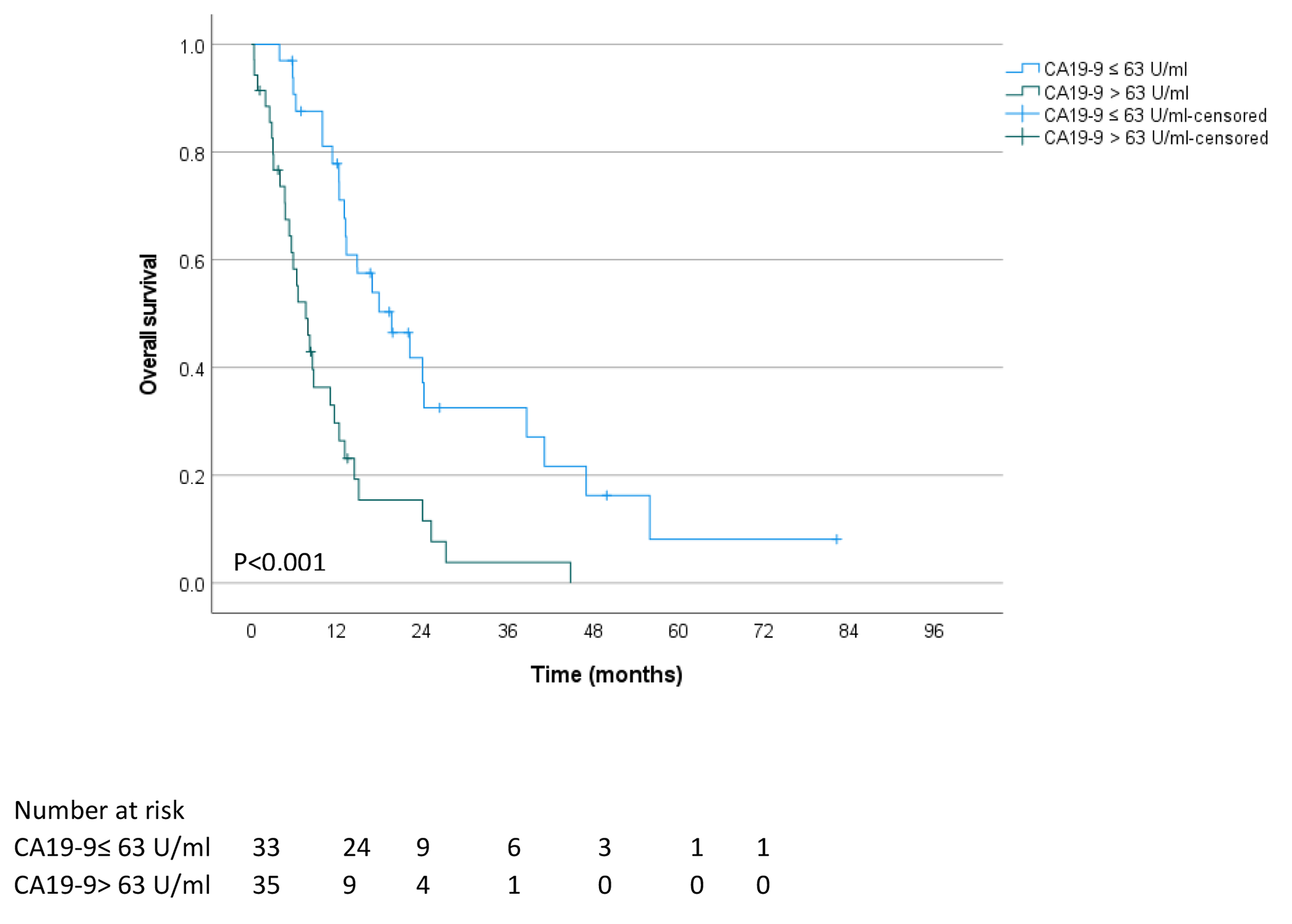
The primary endpoint was local control rate (LCR) at 6 months, and the secondary endpoint was overall survival (OS). Multivariate logistic regression was used to determine the factors associated with treatment efficacy, and cut-off values were determined by receiver operating characteristic (ROC) curve analysis. Local tumor response was evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST1.1) criteria, and complications were scored according to the criteria set by the Radiation Therapy Oncology Group/European Organisation for Research and Treatment of Cancer Late Radiation Morbidity Score.
Follow-up assessments were performed at 1, 2, 4, 6, 9, and 12 months after the procedure, and after 1 year, the patients were followed up every 6 months. The follow-up clinical evaluations mainly included physical examination, CT scans, and magnetic resonance imaging (MRI).The total follow-up period was 5years.
Statistical analysis
Statistical analysis was performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). If a patient underwent particle implantation at two or three different sites, each site was considered separately when LCR was analyzed. The Kaplan-Meier method was used to estimate survival rates. The paired t-test was used to compare the parameters of the preoperative plan and the actual postoperative results. The Wilcoxon rank–sum test was used for univariate analysis, and the Cox regression model was used for multivariate analysis. The selected common independent variables were analyzed by ROC curve analysis, and the area under the curve (AUC) was calculated. P < 0.05 was considered to indicate statistical significance.




留言 (0)