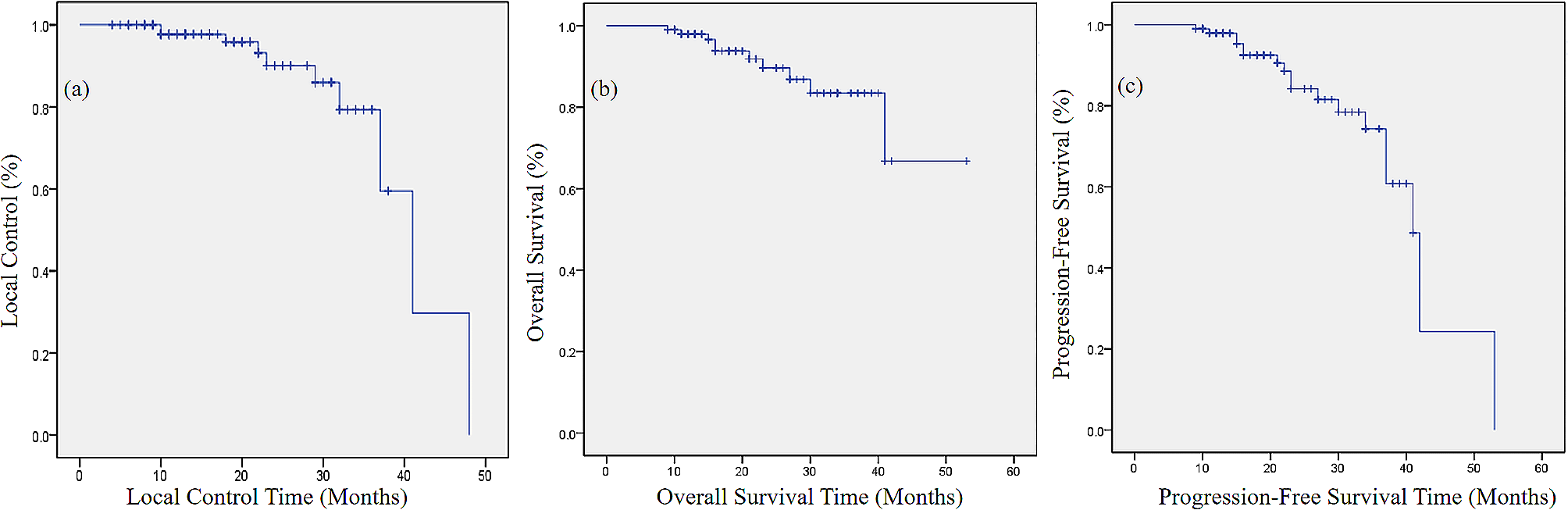
This retrospective study was performed in a real-world cohort of patients with mUC that had received SBRT to treat either OMD or OPD. Our aim was to evaluate LCR, PFS, OS and feasibility of SBRT. A high LCR was achieved and the planned SBRT could be completed in all patients, except for one case with radiation related pain in the chest wall. The median PFS and OS were around 4 and 26 months, respectively. Notably, we found a subgroup of patients (15%) achieving durable survival of at least 42 months and never requiring systemic treatment after SBRT, even though one of these subjects received subsequential SBRT at different time points due to disease progression (including against brain metastases). However, most of the patients were subsequentially treated with systemic therapy due to further disease progression after SBRT.
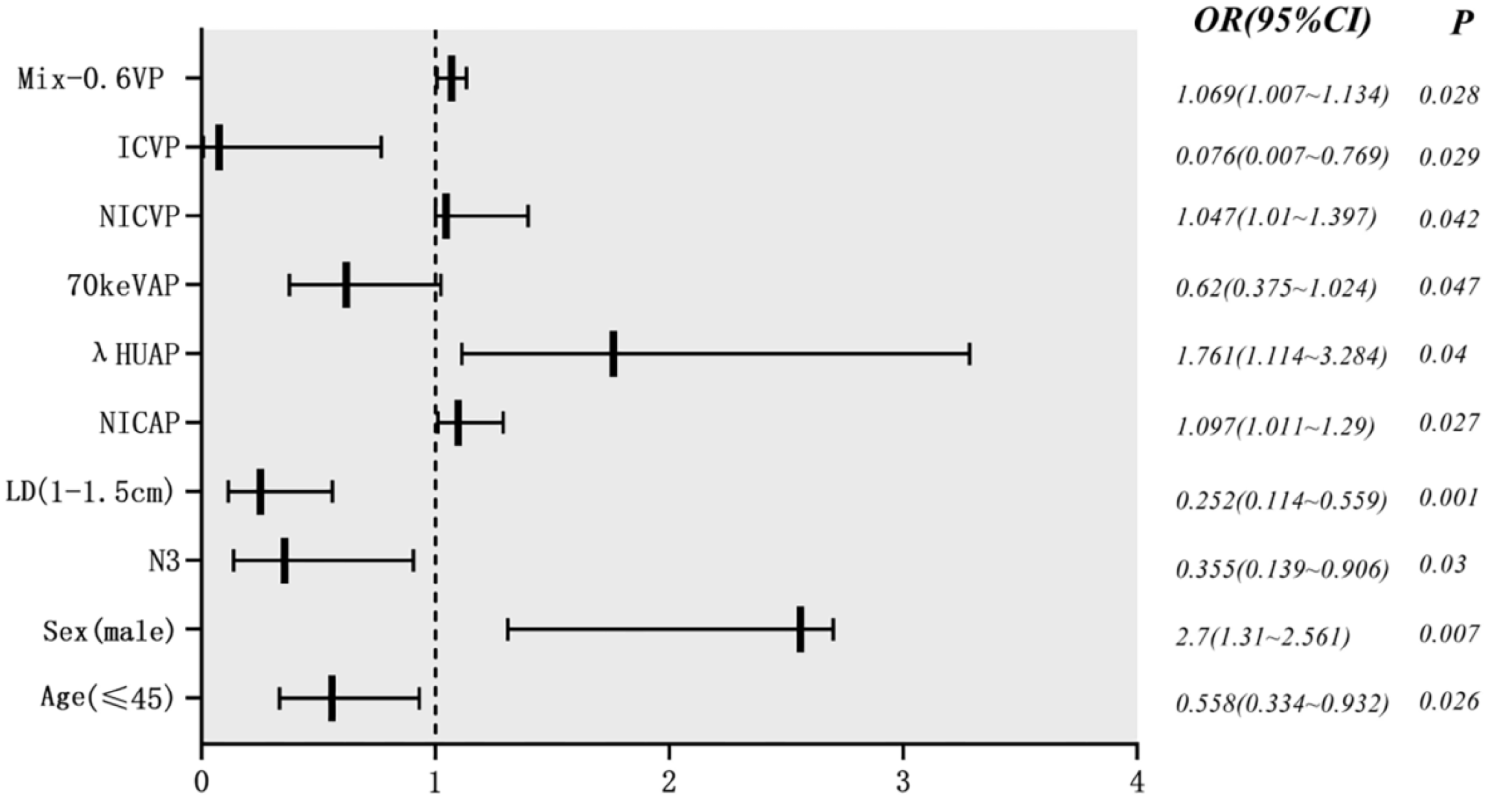
In the present cohort most patients were older male with good ECOG PS and with the primary tumour originating from the urinary bladder. In most cases the treatment intention was to eradicate OMD in the lungs and lymph nodes. Only a minority of patients had primarily metastatic disease at diagnosis and the median time between the diagnosis of muscle invasive urothelial cancer and SBRT was 23 months. Patients with only one metastasis had a statistically significant better prognosis than those with two or more metastasis.
SBRT in patients with oligometastatic mUC is poorly studied and to the best of our knowledge there is no prospective randomized study evaluating this therapeutic option. A systematic review and meta-analysis including available reports addressing SBRT in patients with oligometastatic and oligoprogressive urothelial cancer identified 6 studies with 158 patients included in total [11]. The publications included in the meta-analysis come from small and retrospective studies with significant variation regarding inclusion criteria, assessment of outcomes, etc [12,13,14,15,16,17]. , making a comparison between these studies challenging. This meta-analysis showed that most patients were older males with primary tumours in the urinary bladder, in agreement with our data, and as expected for urothelial cancer [11]. The most common site of SBRT treated metastases were in the lymph nodes (52%), whereas in our cohort metastases were located mainly in the lungs (44%). Our outcomes of interest are within what has been reported in the meta-analysis. The LCR variated between 57% and 90%, median PFS between 3 and 10 months and median OS between 15 and 51 months [11].
A Canadian prospective, non-randomised study included 137 patients with different solid tumours (including genito-urinary) and extracranial OMD suitable for local approach, and with at least one lesion able to be treated with SBRT. 78% of the patients had only one metastatic lesion and the median follow-up was 36 months. The authors observed a plateau in the PFS curve at 36 months of around 18% similarly to our findings in the present study, indicating that there is a subpopulation of patients which achieves good clinical benefit of the given SBRT. The cumulative local progression rate at 36 months was 38% and PFS was accompanied by preservation of quality of life, good symptom control and less need of systemic therapy [18].
SBRT has been shown to be a beneficial therapeutic option in patients with other solid tumours as well, including renal cell cancer and lung cancer. The local tumour control rate has been reported high, SBRT was well tolerated, and some patients achieved a long-term clinical benefit [19, 20].
The main limitation of our study is the retrospective nature of the data without a control arm. Furthermore, the cohort is small and heterogenous regarding primary tumour location, distribution pattern of metastases, and previous treatments. However, the data is generated from real-world patients with a long follow-up and indicates that selected patients with solitary metastases may achieve long term OS without the need of subsequent systemic therapy.
Our cohort includes patients treated between 2009 and 2022 and many drugs, including immunotherapy, have been approved in this field since then and there is more to come [3, 5,6,7, 21, 22]. Toxicities and costs of these new regimens are nonetheless significant and delaying or avoiding systemic therapy may be beneficial and cost saving. In addition, OPD during immunotherapy is a well-known phenomenon and there is evidence that local therapy against OPD may result in durable disease control [23]. Besides, Daro-Faye et al. have demonstrated that radiation and immunotherapy may have synergistic anti-tumoral response in urothelial cancer [24] and emphasize the great need of more contemporary research in this field.







留言 (0)