Cervical cancer is the second most common female cancer in developing countries [8]. Cervical cancer patients in China accounted for one-fifth of the world’s total, which posed a serious threat to the lives and health. According to the NCCN guidelines, it recommended that EBRT and concurrent chemotherapy combined with brachytherapy as the standard treatment for LACC [7]. As for EBRT, IMRT is currently the most mainstream radiotherapy technique which can provide accurate dose distribution in the irradiated target regions. VMAT is a novel form of IMRT, which could shorten treatment time, deliver more accurate dose distribution, and better protection for the adjacent normal tissues. As for brachytherapy, compared to conventional 2D brachytherapy, image-guided adaptive brachytherapy could allow a higher dose of PTV and spare the OARs. MRI-guided adaptive brachytherapy could provide a better definition of the lesion and involved parametria, which was recommended as gold standard imaging for cervical cancer contours. However, it also has disadvantages such as cost issues, long scanning time, and the lack of MRI-compatible applicators in many institutions. CTGAB has more frequently been used instead as it is readily available, more widespread, and more affordable in many centers, especially in developing countries. Considering that there were limited data available on the clinical efficacy and the safety of VMAT combined with CTGAB, therefore, this study aimed to retrospectively report the treatment outcomes of CTGAB for 102 patients with LACC treated in China.
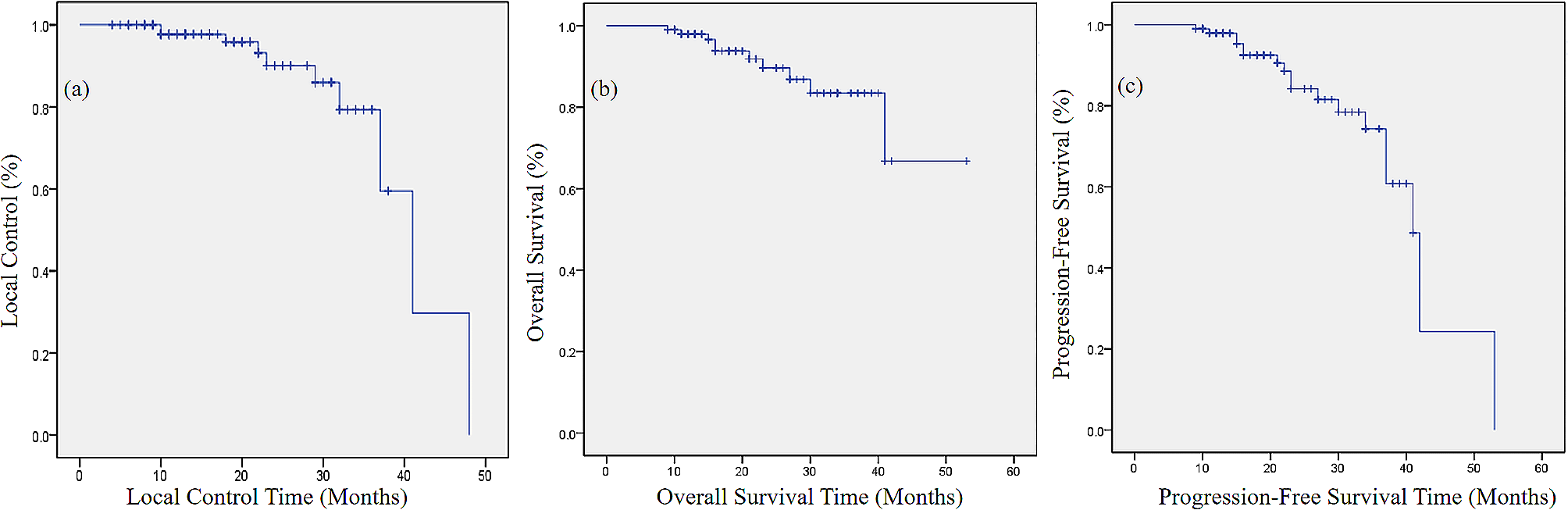
Table 4 summarizes the clinical outcomes of image-guided brachytherapy mentioned in this study. In our retrospective study, the 2-year rates for OS, PFS, and LC were 89.6%, 84.2%, and 90.1%, respectively. And the 3-year rates for OS, PFS, and LC were 83%, 74.3%, and 79.3%, respectively. Droge et al. compared the outcomes and toxicities with VMAT to conventional 3D-CRT, and they demonstrated that VMAT could reduce the toxicities and improve long-term survival. They reported that the 2-year OS and PFS were 90% and 86%, respectively, which was in concordance with ours [9]. A study that was based on MRI-guided adaptive brachytherapy combined with IMRT analyzed 128 patients with cervical cancer. They observed that the 2-year OS was 85% and the 3-year OS was 76.6%, which was inferior to ours. However, they reported that the 2-year LC was 91.6%, slightly higher than ours, which was possibly caused by the inclusion of early-stage cervical cancer [10]. Chi et al. analyzed 97 patients who were treated with MRI-guided adaptive brachytherapy. They reported that the 2-year OS was 83.5% and the 2-year LC was 94.8%. Their 2-year LC was higher than ours, which was possibly caused by the proportion of patients with advanced cervical cancer staging was relatively higher in our study [11].
Table 4 The outcome and the dosimetric parameters of image-guided adaptive brachytherapyA meta-regression analysis retrieved 13 series reporting on 1299 patients to analyze the correlation between the D90% of the HR-CTV and LC. They demonstrated that there was a significant correlation between the D90% of the HR-CTV and the probability of achieving LC. They suggested that the D90% of the HR-CTV associated with a 90% probability of achieving LC was 81.4 Gy and the D90% of 90 Gy corresponded to 95% of LC [16]. Schmid et al. compared the spatial dose distribution with a matched-pair analysis and found that the average D90% of the HR-CTV in patients with local recurrence was 77 Gy, while the average D90% of the HR-CTV in patients with continuous complete local remission was 95 Gy [17]. The American Brachytherapy Society (ABS) guideline recommended that the D90% of the HR-CTV > 85 Gy to maintain a satisfactory LC. Mazeron et al. retrospectively analyzed 225 patients and demonstrated that the LC was 91% when the D90% of the HR-CTV was > 85 Gy [18]. Dimopoulos et al. analyzed 141 patients and found that the LC was > 95% when the D90% of the HR-CTV was > 87 Gy [19]. Murakami et al. analyzed 42 patients with cervical cancer who were treated with conventional 3D-CRT and CTGAB, and they reported that 2-year LC was 80.2%, which was possibly caused by the median D90% of the HR-CTV was only 70.3 Gy [12]. In recent research, Yoshio et al. analyzed 97 patients who were treated with CTGAB and reported that the 2-year LC was 87%, which was possibly caused by the median D90% of the HR-CTV was only 66.3 Gy [13]. In our retrospective study, the average cumulative and the median D90% of the HR-CTV were 92.26 Gy and 92.65 Gy, respectively, which could explain why our LC was superior to most studies.
Concerning the anatomical proximity between the lesion and OARs, while increasing the D90% of the HR-CTV, it was inevitable that it would also increase the dose of OARs, which could increase the incidence of toxicities. The incidence of gastrointestinal and urinary toxicities varied from 0.9 to 9.0% among different studies. In our retrospective study, grade ≥ 3 gastrointestinal and urinary toxicities occurred in 4.9% and 0.98%, respectively. And 1.96% of patients were observed grade ≥ 4 gastrointestinal toxicities. In addition, the average cumulative D2cm3 in the rectum, the bladder, the colon, and the small intestine were 78.07 Gy, 93.20 Gy, 63.55 Gy, and 61.07 Gy, respectively. An EMBRACE II study analyzed 960 patients undergoing EBRT combined with brachytherapy. They observed that the incidence of grade 2–4 proctitis is 26% when the patient’s cumulative D2cm3 of the rectum ≥ 75 Gy [20]. In our prospective study, the patient’s cumulative D2cm3 of the rectum ≥ 75 Gy, the incidence of grade 2–4 proctitis is 7.5%. Our incidence of proctitis was lower, which was possibly caused by more stringent dose constraints of the rectum when improving the D90% of the HR-CTV and more active follow-up for preventing toxicities. Kamran et al. analyzed 56 patients with LACC to compare LC, OS, and toxicities between CTGAB and MRI-guided brachytherapy. And they demonstrated there was no difference in toxicities between the two guided methods [15]. Ribeiro et al. analyzed 170 cervical cancer patients who were treated with MRI-guided brachytherapy after initial radiotherapy. They observed that the incidence of grade 3–4 gastrointestinal toxicity is 5%, while the incidence of gastrointestinal toxicity in the CTGAB we analyzed was 4.9%, which suggested that the efficacy and safety of CTGAB are acceptable [14].
In conclusion, the combination of VMAT and CTGAB for LACC has good effects in LC, OS, and PFS, and an acceptable incidence of toxicities. In developing countries, due to limitations in economic and medical resources, to provide effective treatment for more cervical cancer patients, CTGAB can be used as a recommended treatment method.
Limitation
This study had some limitations. First, the sample size is relatively small. Second, the study was established based on cases from a single center. Further studies are needed at different centers to validate our results. Third, this study was developed based on a retrospective cohort. Prospective cohorts are needed in future studies for further validation.







留言 (0)