Study Design
This was a prospective, multicenter, core laboratory-adjudicated, single-arm trial. The trial was independently monitored by a data safety monitoring board and clinical events committee (CEC) that reviewed and adjudicated all adverse events throughout the 24-month period following DCB treatment. Independent duplex ultrasound (DUS) (VasCore, Massachusetts General Hospital, Boston, MA, USA) and angiography (Beth Israel Deaconess Medical Center Cardiovascular Imaging Core Laboratory, Boston, MA, USA) core laboratories analyzed procedural and follow-up images. The trial was conducted in accordance with the Declaration of Helsinki, good clinical practice guidelines, and applicable laws.
Study Population
Inclusion and exclusion criteria are summarized in the supplemental table. In brief, chronic symptomatic lower limb ischemia (classes 2–4 according to Rutherford’s classification) due to stenotic or non-stented restenotic lesions with a total lesion length ≤ 18 cm or totally occlusive lesions with a length of ≤ 10 cm involving the SFA and proximal PA was eligible. Prior to enrollment, written informed consent was obtained from all patients in accordance with the protocols approved by the institutional review boards at each investigational site.
Description of TCD-17187 DCB
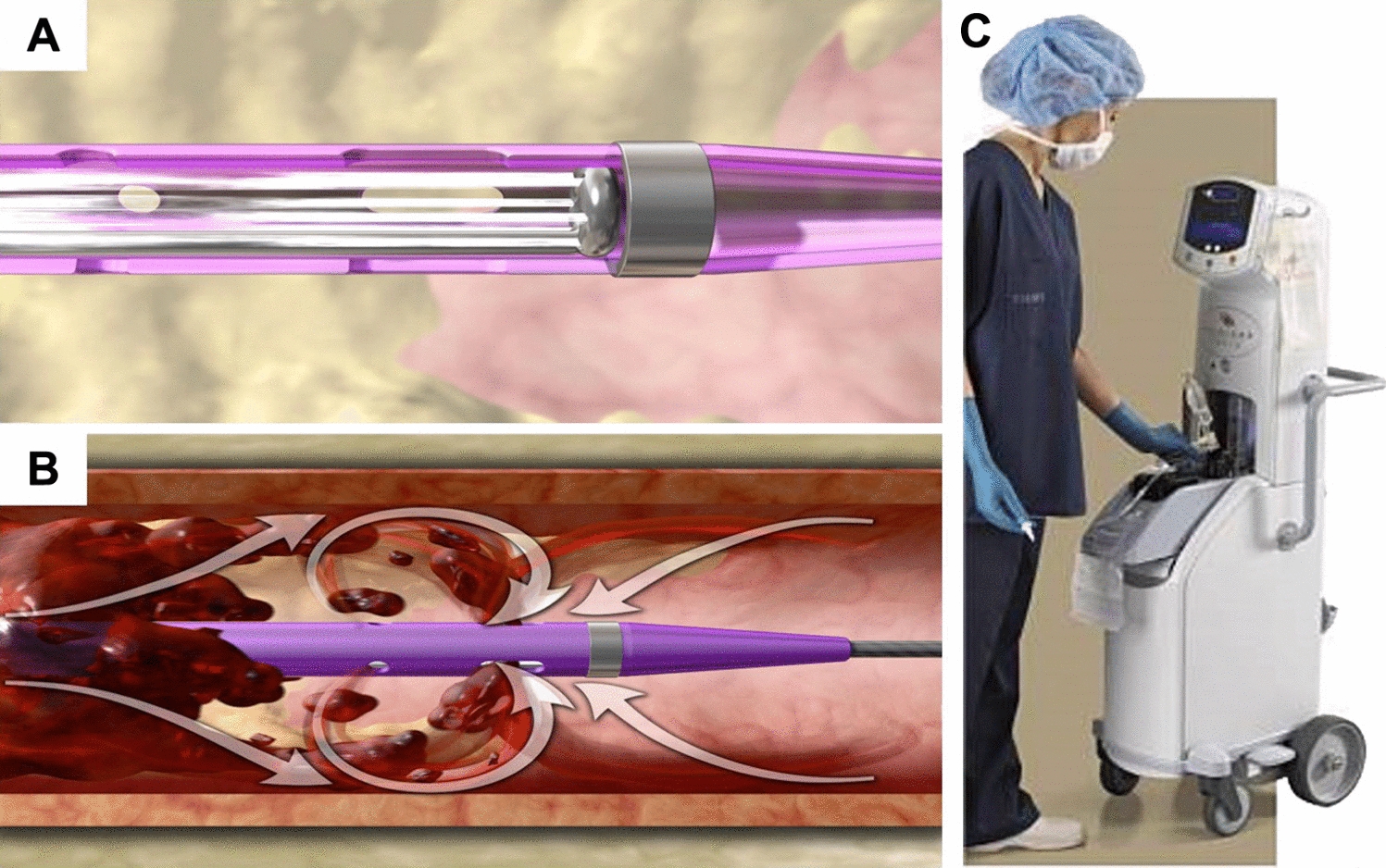
TCD-17187 (Terumo Corporation, Tokyo) has obtained CE but is not yet available in the market. It is coated with 3.2 μg/mm2 of PTX as an antiproliferative agent and a low-molecular-weight excipient L-SEE, which has hydrophobic groups that have affinity for PTX and hydrophilic groups that have affinity for water. The surface of the TCD-17187 DCB is uniformly coated with small PTX microcrystals, aiming an improvement in drug retention during balloon delivery and promotion of PTX release during balloon expansion by optimizing the balance between the two groups.
Intervention Procedure and Follow-Up
Dual antiplatelet therapy (DAPT) was required prior to the index procedure. At the time of initial angiography, the status of in-flow and out-flow was evaluated to ascertain whether the patient was a suitable candidate for this trial. Heparin was administered at the beginning of the procedure, and an activated clotting time of 250 s was maintained throughout the procedure. Pre-dilatation was mandated, but no special PTA (percutaneous transluminal angioplasty) balloons including cutting or scoring balloons were allowed for pre-dilatation. DCB size was to have the same diameter as the reference vessel in a 1:1 balloon-to-vessel ratio. The recommend inflation time of the DCB was at least 180 s. Post-dilatation with a standard PTA balloon was allowed at the discretion of the operator. Provisional stenting was allowed only in the event of PTA failure after repeated and prolonged balloon inflations. PTA failure was defined as a residual stenosis ≥ 50% or major flow-limiting dissection (≥ Grade D on NHBLI). DAPT (100 mg/day aspirin with 75 mg/day clopidogrel or 3.75 mg/day prasugrel) was continued for at least 1 month after the index procedure. Follow-up was conducted at 30 days, 6 months, 1 year, and 2 years after the index procedure. The final follow-up was planned at 3 years postoperatively.
Demographic characteristics, comorbidities, ankle–brachial index (ABI), Rutherford classification, quality of life, angiographic lesion characteristics, and concomitant medications were recorded preoperatively. Intraoperatively, procedural details such as pre-dilatation and DCB use (size, dilatation pressure, dilatation time, angiographic procedural success, etc.) were evaluated. At each follow-up, we evaluated primary patency using DUS and assessed for any major adverse events (MAE) or other adverse events.
Definitions
Primary patency was defined as core laboratory-assessed DUS peak systolic velocity ratio < 2.4 in the absence of CD-TLR. CD-TLR was defined as re-intervention at the target lesion due to recurrence of symptoms with ≥ 50% restenosis by core laboratory assessment, worsening of Rutherford classification, or decreasing ABI > 0.15, when compared with post-procedure baseline. Major amputation was defined as amputation of the limb above the ankle. Technical success was defined as residual stenosis in the treated segment of 30% or less without grade D or greater vessel dissection. Procedural success was defined as achieving technical success without the occurrence of a MAE during the index procedure. An MAE was defined as a composite of device- and procedure-related 30-day death, or an index limb major amputation and/or CD-TLR during follow-up.
Study Outcome Measures
The primary efficacy outcome measure was primary patency after the index procedure up to 24 months. The secondary efficacy outcome measures comprised (1) freedom from CD-TLR, (2) change in ABI, (3) clinical improvement based on the Rutherford classification, and (4) the Walking Impairment Questionnaire (WIQ) score throughout the follow-up period. The primary safety outcome measure was the MAE rate. AEs were evaluated at 30 days, 6 months, 1 year, and 2 years. Death, repeat revascularization, and amputation were independently adjudicated by the CEC.
Statistical Analysis
For effectiveness, the analysis dataset included all enrolled patients in the study except one patient who was adjudicated as having no ischemic vascular stenosis/occlusion. The Kaplan–Meier method was used to evaluate time-to-event data for primary patency at 24-month follow-up. In the exploratory data analysis, the hazard ratio was calculated using a univariate Cox regression model to examine patient, lesion, and procedure characteristics that may affect primary patency. For multivariate analysis with Cox regression model, the backward elimination was used with an elimination criterion of p value ≥ 0.1. Continuous variables were expressed as the mean ± standard deviation. Categorical variables were presented as counts and proportions.
Statistical analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC, USA).

留言 (0)