
記住我







Health-care costs in the United States are rising at unsustainable rates that cannot be explained by inflation, population growth, or improvements in the quality of care1. Value-based health care is 1 strategy that aims to fundamentally restructure health-care delivery, measurement, and reimbursement in order to increase value, defined by Porter et al. as health outcomes relative to costs2–5. Given the growing financial burden of musculoskeletal care in the U.S., value-based initiatives have received increasing attention in the field of orthopaedic surgery6–10.
Increasing value necessitates the accurate measurement of health-care costs in order to complete the value equation and to identify opportunities to optimize the care pathway11–13. Time-driven activity-based costing (TDABC) is 1 accounting methodology that measures costs by integrating resource expenditure (i.e., quantity and time) with the associated per-unit cost required to deliver care on a procedure-specific basis14–16. By leveraging this “bottom-up” approach, TDABC accounts for heterogeneity between care cycles and has been shown to outperform traditional hospital accounting systems by delivering lower costs, improved accuracy, and actionable insights17–20. TDABC has previously been employed by health organizations to characterize episode-of-care costs21–25 and to improve value11,12,23,26–29.
Despite the rapidly expanding indications for, and utilization of, hip arthroscopy over the past 2 decades, its costs have not yet been investigated with use of TDABC30–32. Previous studies have assessed the gross cost and relative cost-effectiveness of hip arthroscopy; however, available analyses have been limited by their derivation of costs from insurance reimbursements, hospital charges, or national averages—all of which have been criticized for limited accuracy and a lack of granularity33–39. Thus, further investigation is needed to elucidate the factors underlying variation in the true cost of hip arthroscopy.
Therefore, the purposes of this study were to employ TDABC to characterize the cost composition of outpatient hip arthroscopy for labral pathological conditions and to identify factors that drive variation in cost. We hypothesized that there exists a wide variation in cost that is moderately (i.e., 30% to 50%) explained by surgeon and procedure-specific features36,40,41.
Materials and Methods Sample and Study DesignFollowing institutional review board approval (Mass General Brigham IRB #2022P002843), all hip arthroscopy procedures performed within a single, large urban health-care system between June 2015 and November 2022 were identified with use of CareMeasurement (Avant-garde Health). This software enabled the collection of patient-level electronic health record (EHR) data, such as staff-entered time stamps, supplies utilized, and associated supply-purchasing costs. Procedures were included if the patient was ≥18 years old, hip arthroscopy was clinically indicated to address labral pathological conditions, and the procedure was performed by a surgeon who completed ≥20 total hip arthroscopy procedures during the study period. This arbitrary cutoff of 20 surgeries was selected to ensure both statistical robustness (i.e., by avoiding overfitting in the multivariable model) and clinical relevance (i.e., by including surgeons with enough volume to be proficient while maximizing study generalizability)42. This cutoff ultimately resulted in the exclusion of 2 surgeons who performed 5 and 6 procedures, respectively, over the study period. Additionally, procedures with total costs in the upper (≥95th) and lower (≤5th) percentiles were manually reviewed for anomalies in order to exclude those that demonstrated unreconcilable documenting errors or discrepancies. Notably, these inclusion and exclusion criteria resulted in the inclusion of some hip arthroscopy cases that included concomitant intra-articular procedures (e.g., microfracture), as excluding such cases would artificially deflate cost variation.
Time-Driven Activity-Based CostingTDABC was performed in accordance with guidelines established by Kaplan, Anderson, and other experts14,16,27,43–45. Briefly, applying TDABC on a patient-specific basis requires outlining process maps to encompass the relevant steps of the care pathway, determining and quantifying the resources required during each step, multiplying the resources expended by their associated per-unit cost, and summing these products to quantify the total cost for a given episode of care. Additional details regarding our application of TDABC are provided in Appendix 1 and Appendix Tables 1, 2, and 321–24,27,29,40,46.
Data Collection and OutcomesData regarding patient characteristics were manually extracted from the EHR and included age, body mass index (BMI), gender, race, ethnicity, American Society of Anesthesiologists (ASA) classification, previous hip surgeries, and insurance status. Granular procedure-specific features were manually obtained from operative notes and included the surgeon, surgery center, members of the provider team, and arthroscopic interventions performed. Of note, “labral augmentation” refers to labral repair with augmentation via a capsular autograft47,48. Procedure-specific time stamps and supply costs were extracted with use of CareMeasurement and were subsequently verified during chart review.
Statistical AnalysisAll costs were calculated in U.S. dollars and, per institutional policy, subsequently multiplied by an undisclosed constant to normalize the study mean for the total cost to 100 in order to protect the confidentiality of internal hospital cost data; this normalization preserved relative values and had no impact on the subsequent statistical analysis. Descriptive statistics are presented as means and standard deviations (SDs) for continuous variables and as frequencies and percentages for categorical variables. Given the large sample size, the Kolmogorov-Smirnov test and quantile-quantile plots were utilized to assess normality49. Such testing revealed that the cost data approximated a normal distribution; thus, parametric tests were employed for untransformed costs. Associations between costs and continuous variables were explored with use of the Pearson correlation coefficient (r), whereas costs were compared between categorical variables with use of the unpaired t test or 1-way analysis of variance, as appropriate. Multivariable linear regression was performed to identify factors independently associated with total costs, controlling for patient characteristics, procedure-specific factors, surgeon, and surgery center. Model variables were selected on the basis of previous literature, clinical relevance, unadjusted analyses, and information criteria (i.e., the Akaike information criterion and Bayesian information criterion)50. Analyses were performed with use of R (R Foundation for Statistical Computing; version 4.2.1). Significance was set at p < 0.05.
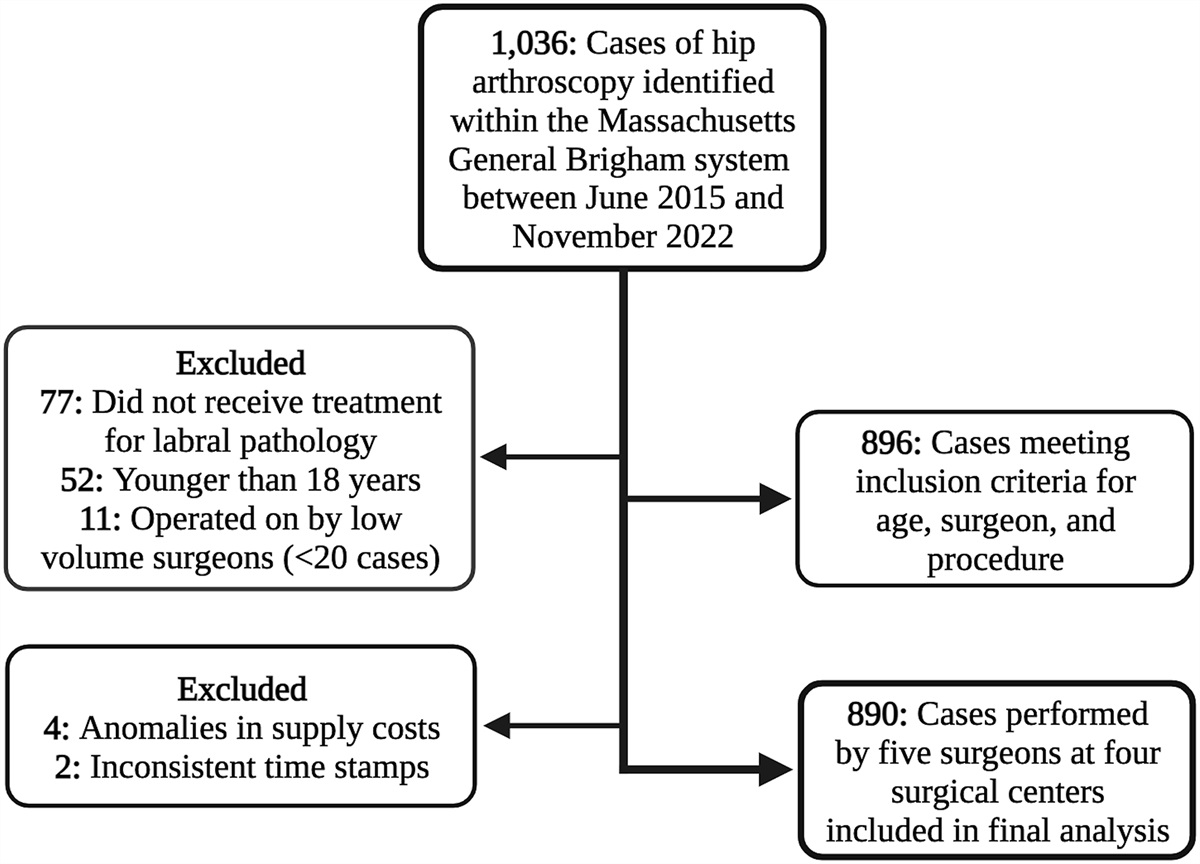
Results ParticipantsOf the 1,036 procedures screened for the study, 890 met the inclusion criteria (Fig. 1). Procedures were performed by 5 surgeons operating at 4 outpatient surgery centers within a single institution. The study sample consisted of 515 women (57.9%) and 375 men (42.1%), with a mean age (and SD) of 37.1 ± 12.7 years and a mean BMI of 26.6 ± 4.7 kg/m2. Most of the procedures were performed in patients who were White (90.6%) or not Hispanic (93.4%). The most common method of labral management was labral repair (59.7%), and the most commonly performed type of osteoplasty was femoral osteoplasty with acetabular rim trimming (45.7%; Table I).
 Fig. 1:
Fig. 1: Flowchart detailing the selection process for the study sample.
TABLE I - Characteristics of the Study Population (N = 890)* Variable Mean ± SD or No. (%) Year of surgery 2015 9 (1.0%) 2016 61 (6.9%) 2017 86 (9.7%) 2018 142 (16.0%) 2019 93 (10.4%) 2020 142 (16.0%) 2021 180 (20.2%) 2022 177 (19.9%) Age (yr) 37.1 ± 12.7 BMI (kg/m 2 ) 26.6 ± 4.7 Gender Female 515 (57.9%) Male 375 (42.1%) Race Asian 23 (2.6%) Black or African American 22 (2.5%) White 806 (90.6%) Other 21 (2.4%) Unavailable 18 (2.0%) Ethnicity Hispanic or Latino 34 (3.8%) Not Hispanic or Latino 831 (93.4%) Unavailable 25 (2.8%) ASA class 1 380 (42.7%) 2 476 (53.5%) 3 34 (3.8%) Previous ipsilateral surgery 30 (3.4%) Previous contralateral surgery 85 (9.6%) No. of suture anchors 3.1 ± 1.1 Osteoplasty type Acetabuloplasty 162 (18.2%) Femoroplasty 224 (25.2%) Combined 407 (45.7%) None 97 (10.9%) Labral procedure Debridement 76 (8.5%) Repair 531 (59.7%) Augmentation† 266 (29.9%) Reconstruction 17 (1.9%) Capsular management Interportal capsulotomy with repair 259 (29.1%) Interportal capsulotomy without repair 120 (13.5%) T-capsulotomy with repair 206 (23.1%) T-capsulotomy without repair 8 (0.9%) Puncture capsulotomy 297 (33.4%) Surgeon Surgeon 1 297 (33.4%) Surgeon 2 275 (30.9%) Surgeon 3 231 (26.0%) Surgeon 4 52 (5.8%) Surgeon 5 35 (3.9%) Surgery center Surgery center A 366 (41.1%) Surgery center B 254 (28.5%) Surgery center C 177 (19.9%) Surgery center D 93 (10.4%) Insurance Government 93 (10.4%) Private 763 (85.7%) Workers’ Compensation or MVA claims 34 (3.8%)*MVA = motor vehicle accident.
†Labral augmentation refers to labral repair with augmentation via capsular autograft47,48.The normalized total cost of hip arthroscopy per procedure ranged from 43.4 to 203.7 (mean, 100 ± 24.2; Fig. 2). On average, supply costs accounted for 48.8% of total costs, and labor costs accounted for the remaining 51.2% (fixed, 8.5%; variable, 42.7%; Fig. 3). The majority (91.5%) of total costs were incurred during the intraoperative phase, with the remaining costs incurred during the preoperative (5.5%) and postoperative phases (3.0%; Table II). Relevant time metrics by phase are summarized in Table III. Between procedures in the 10th and 90th percentiles for total costs, there was a 1.8-fold variation in total costs, a 2.5-fold variation in supply costs, and a 1.8-fold variation in labor costs. Further analysis of procedures in the 10th and 90th percentiles for supply costs identified a 5.0-fold variation in the costs of implants (i.e., suture anchors and allografts), a 1.3-fold variation in the costs of individual anchors from different manufacturers, and a 3.1-fold variation in the costs of other supplies (e.g., disposables). Total cost was strongly correlated with operative time (r = 0.81; 95% confidence interval [CI], 0.78 to 0.83; p < 0.001), labor costs (r = 0.80; 95% CI, 0.78 to 0.83; p < 0.001), and supply costs (r = 0.89; 95% CI, 0.88 to 0.90; p < 0.001). Normality testing revealed that cost data followed a normal distribution (D = 0.0253; p = 0.62; see Appendix Fig. 1).
 Fig. 2:
Fig. 2: Scatterplot depicting variation in the normalized cost of outpatient hip arthroscopy for labral pathological conditions. Each point represents an individual procedure, with the procedure number denoted by its position on the x axis.
 Fig. 3:
Fig. 3: Cost composition of outpatient hip arthroscopy stratified by labor and supply costs (Fig. 3-A) and phases of the care cycle (Fig. 3-B).
TABLE II - Normalized Cost Estimates for the Hip Arthroscopy Care Cycle Variable Mean ± SD Total cost 100.0 ± 24.2 Total supply cost 48.8 ± 16.1 Implant and/or allograft costs 15.8 ± 9.2 Other (e.g., disposables) costs 33.0 ± 12.9 Total labor cost 51.2 ± 12.3 Fixed labor cost 8.5 ± 0.2 Variable labor cost 42.7 ± 12.2 Preoperative cost 5.5 ± 0.1 Intraoperative cost 91.5 ± 24.2 Postoperative cost 3.0 ± 0.2*OR = operating room. Values are given as the mean ± SD.
A positive correlation (r = 0.41; p < 0.001) between total cost and operative year was demonstrated throughout the study period. Patient characteristics that were significantly associated with higher costs were younger age (r = −0.24; p < 0.001), Black race (e.g., mean normalized costs of 111.0 [Black patients] versus 99.2 [White patients]; p = 0.023), and male gender (106.1 [male] versus 95.6 [female]; p < 0.001). However, total cost was not found to be significantly associated with BMI, ethnicity, ASA class, previous ipsilateral or contralateral hip surgery, or insurance coverage (p > 0.05 for all). Regarding operative features, the more labor-intensive labral management methods (i.e., repair, augmentation, or reconstruction), osteoplasty types (e.g., combined femoroacetabular decompression), and capsular management techniques (e.g., interportal capsulotomy with repair) were associated with significantly higher total costs (p < 0.001; Table IV).
TABLE IV - Unadjusted Analyses Exploring Associations Between Study Characteristics and Normalized Total Costs* Variable Pearson Correlation Coefficient (95% CI) P Value Year of surgery 0.41 (0.35, 0.46) <0.001 Age −0.24 (−0.30, −0.17) <0.001 BMI 0.03 (−0.03, 0.09) 0.37 Variable Mean Normalized Cost (95% CI) P Value Gender <0.001 Female 95.6 (93.6, 97.6) Male 106.1 (103.6, 108.6) Race 0.023 Asian 102.6 (95.1, 110.1) Black or African American 111.0 (100.0, 122.0) White 99.2 (97.6, 100.8) Other 105.6 (92.0, 119.2) Unavailable 112.1 (94.3, 129.9) Ethnicity 0.15 Hispanic or Latino 104.3 (95.0, 113.6) Not Hispanic or Latino 99.6 (98.0, 101.2) Unavailable 107.7 (96.1, 119.3) ASA class 0.38 1 100.6 (98.4, 102.8) 2 99.2 (96.9, 101.5) 3 104.5 (93.3, 115.7) Previous ipsilateral surgery 0.82 Yes 99.0 (85.7, 112.3) No 100.0 (98.4, 101.6) Previous contralateral surgery 0.12 Yes 103.9 (98.2, 109.6) No 99.6 (97.9, 101.3) Osteoplasty type <0.001 Acetabuloplasty 89.4 (86.5, 92.3) Femoroplasty 95.1 (92.7, 97.5) Combined 114.1 (112.1, 116.1) None 70.1 (66.5, 73.7) Labral procedure <0.001 Debridement 64.2 (60.0, 68.4) Repair 104.6 (102.7, 106.5) Augmentation† 97.8 (95.9, 99.7) Reconstruction 149.8 (134.8, 164.8) Capsular management <0.001 Interportal capsulotomy with repair 117.5 (114.8, 120.2) Interportal capsulotomy without repair 70.0 (65.8, 74.2) T-capsulotomy with repair 100.4 (96.9, 103.9) T-capsulotomy without repair 118.2 (93.0, 143.4) Puncture capsulotomy 96.1 (94.0, 98.2) Insurance 0.064 Government 94.5 (88.8, 100.2) Private 100.6 (98.9, 102.3) Workers’ Compensation/MVA claims 102.2 (91.6, 112.8)*Boldface denotes significance. MVA = motor vehicle accident.
†Labral augmentation refers to labral repair with augmentation via capsular autograft47,48.Consistent with the unadjusted analyses, multivariable linear regression revealed that gender, age, the type of osteoplasty, and the method of labral management explained significant variation in total costs, whereas BMI and ASA class were not significant contributors to cost variation. Interestingly, no significant association was found between costs and operative year from 2015 to 2019 (p > 0.1), whereas procedures occurring between 2020 and 2022 were associated with significantly higher costs (p < 0.05 for all). The linear regression model that incorporated these factors as well as operating surgeon and surgery center explained 75.0% of the observed variation in total costs. Notably, the method of labral management independently explained the most variation in total costs (partial R2 = 0.332), followed by the operating surgeon (partial R2 = 0.326), osteoplasty type (partial R2 = 0.087), and surgery center (partial R2 = 0.086; Table V).
TABLE V - Multivariable Linear Regression of Study Characteristics Underlying Variation in Normalized Total Costs* Variable Mean Difference 95% CI Partial R2† P Value Lower Upper Patient characteristics Age, per 1-year increase −0.08 −0.16 −0.01 0.005 0.032 BMI, per 1-unit increase 0.01 −0.18 0.19 <0.001 0.945 Male gender 4.98 3.17 6.80 0.032 <0.001 ASA class‡ <0.001 2 0.04 −1.81 1.89 0.966 3 1.38 −3.33 6.09 0.566 Procedure-specific factors Year of surgery§ 0.036 2016 7.00 −2.03 16.03 0.129 2017 7.38 −1.54 16.31 0.105 2018 7.00 −1.78 15.78 0.118 2019 7.45 −1.46 16.36 0.101 2020 13.83 5.02 22.63 0.002 2021 12.15 3.36 20.94 0.007 2022 11.18 2.38 19.99 0.013 Osteoplasty type# 0.087 Acetabuloplasty 5.19 1.38 9.00 0.008 Femoroplasty 8.22 4.85 11.60 <0.001 Combined 14.60 10.86 18.34 <0.001 Labral procedure** 0.332 Repair 23.68 20.10 27.27
留言 (0)