
記住我







Establishing the optimal coronal alignment for patients undergoing knee arthroplasty is a considerable challenge and a contentious topic in contemporary reconstructive knee surgery1. Historically, the mechanical hip-knee-ankle angle (HKA) has been the primary metric for quantifying coronal alignment, even though it is influenced by cartilage loss and joint-space narrowing. To date, a double-limb-stance full-leg anteroposterior radiograph of the lower limb is widely utilized to define the coronal alignment of the lower limb. However, with the increasing adoption of computed tomography (CT) scans in preoperative planning, there arises an opportunity to estimate the coronal alignment with use of the CT scanogram. More recently, the arithmetic HKA (aHKA) has emerged as a method that could estimate constitutional coronal alignment in the arthritic population2. The aHKA angle utilizes preoperative measurements of the medial proximal tibial angle (MPTA) and lateral distal femoral angle (LDFA) and is characterized by its reliance on osseous landmarks rather than the spatial relationship between the tibia and femur. This approach ensures that the measurements are not influenced by joint-space narrowing, tibiofemoral subluxation, or medial ligamentous laxity3,4. Its predictive value has been demonstrated in both arthritic2 and nonarthritic populations4, as well as in comparisons of the arthritic knee with the unaffected contralateral limb5.
The objective of the present study was to evaluate the correlation in measurements of the lower-limb coronal alignment between traditional long-leg radiographs (LLRs) and CT scanograms that were made during the preoperative planning phase. On the basis of published evidence showing a good correlation between these imaging modalities in measuring the lower-limb mechanical axis6,7, we hypothesized that no significant differences would be found between the 2 in the present study. Moreover, we aimed to identify whether any variables, such as demographic characteristics, the radiographic positioning of the lower limb, the time between LLRs and CT scans, and the severity of the original deformity, were associated with larger discrepancies between the 2 imaging modalities.
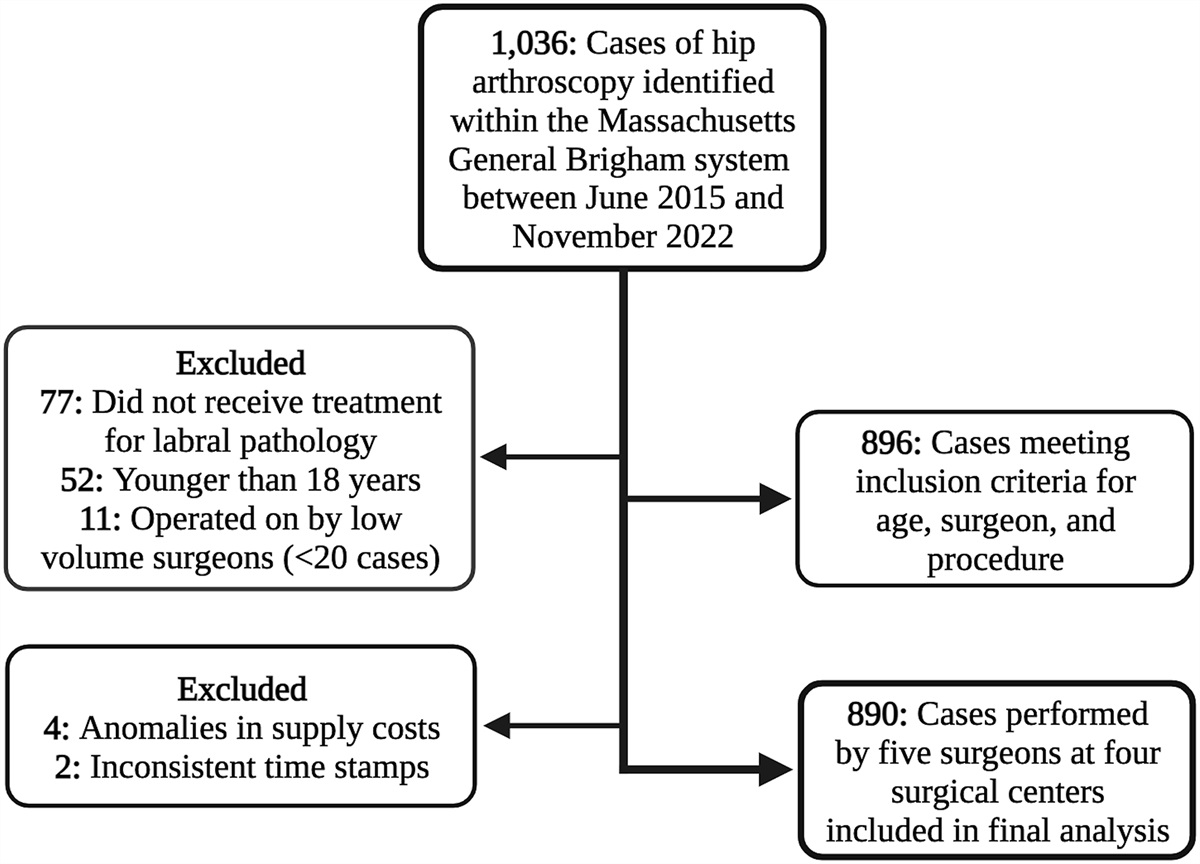
Materials and Methods Study PopulationThis multicenter cohort study was conducted across 3 tertiary centers in the United Kingdom, Belgium, and Luxembourg. The study was individually registered and approved at each institution (reference numbers 23058, 230607, and CSS2014-2307) and included 300 adult patients of any age (100 consecutive patients per participating center) undergoing primary robotic-arm-assisted total knee arthroplasty (TKA) or unicompartmental knee arthroplasty (UKA) for symptomatic knee osteoarthritis (Fig. 1). Following screening, participants with available preoperative LLRs and CT scanograms were enrolled into the study. Patients undergoing revision surgery for any cause, patients with an ipsilateral hip or ankle implant, and patients with a previous osteotomy or posttraumatic deformity of the femur or tibia were excluded.
 Fig. 1:
Fig. 1: Flowchart depicting the patient selection process.
Imaging TechniquesTwo centers utilized conventional radiography to make the LLRs, whereas the third employed the EOS 3D biplanar low-dose imaging system (EOS Imaging). Given our secondary aims to identify variables that had the potential to be associated with greater discrepancies between the 2 imaging modalities and to emulate pragmatic practice when conducting the CT scan, we endeavored to adjudicate the rotation of the lower limb8.
To that end, we introduced the concept of the CT limb rotational angle (CRA), which represents the angle subtended by the posterior condylar axis (PCA) and a horizontal line; positive values denote external rotation and negative values denote internal rotation. The PCA was defined as a line connecting the posterior margins of the medial and lateral femoral condyles (Fig. 2). Additionally, we recorded the time interval between when the LLRs and CT scanograms were made (hereafter referred to as the “time between scans”).
 Fig. 2:
Fig. 2: Depiction of the posterior condylar axis (PCA) and CT limb rotational angle (CRA).
MeasurementsA comprehensive range of measurements was utilized to assess coronal knee alignment (Figs. 3-A and 3-B). These measurements included the femoral mechanical axis (fMA), tibial mechanical axis (tMA), LDFA, MPTA, HKA, aHKA, joint line obliquity (JLO), and joint-line convergence angle (JLCA), which was measured on an LLR, a CT scanogram, and a weight-bearing anteroposterior radiograph. The precise definitions and methods of calculation for each measurement are detailed in Table I. To minimize detection bias, the researchers conducting the measurements were blinded to the results of other measurements throughout the study.
 Fig. 3-A:
Fig. 3-A: The hip-knee-ankle angle (HKA), femoral mechanical axis (fMA), and tibial mechanical axis (tMA).
 Fig. 3-B:
Fig. 3-B: The lateral distal femoral angle (LDFA), medial proximal tibial angle (MPTA), joint-line convergence angle (JLCA), fMA, and tMA.
TABLE I - Definitions and Calculation Methods for Knee Alignment Measurements* Measurement Definition Femoral mechanical axis (fMA) Line from the center of the femoral head to the top of the femoral notch Tibial mechanical axis (tMA) Line from the midpoint of the tibia at the knee joint (i.e., the center of the tibial spine) to the center of the tibial plafond at the ankle Lateral distal femoral angle (LDFA) Lateral angle subtended by the fMA and a line drawn across the distal femoral articular surface Medial proximal tibial angle (MPTA) Medial angle subtended by the tMA and a line drawn across the tibial articular surface at the most distal points Hip-knee-ankle angle (HKA) Medial angle between the fMA and the tMA Arithmetic hip-knee-ankle angle (aHKA) Calculated by subtracting the LDFA from the MPTA Joint line obliquity (JLO) Calculated by adding the LDFA and the MPTA Joint-line convergence angle (JLCA) Measured on LLR, CT scanogram, and weight-bearing anteroposterior radiograph to gauge intra-articular deformity*LLR = long-leg radiographs, CT = computed tomography.
The primary objective of this study was to evaluate the correlation between LLRs and CT scanograms in measuring the coronal alignment of the lower limb. In addition, we utilized regression models to identify variables that were associated with greater discrepancies in measurements between the 2 imaging modalities and further explored the agreement between the imaging modalities at various levels of those variables. Sensitivity analyses were also conducted to determine if the agreement between the LLRs and CT scanograms differed when these modalities were utilized to examine patients with medial or lateral osteoarthritis.
Power Analysis and Sample Size CalculationTo determine the required sample size, we conducted a priori power analyses. Our aim was to ensure sufficient statistical power to identify even a marginal effect size and correlation between the 2 imaging modalities. To achieve a statistical power of 0.9 for detecting a correlation coefficient of 0.2 at a significance level of 0.05, a minimum of 259 paired observations were necessary9,10. To account for potential data loss, outliers, or unforeseen circumstances that could impact our analysis, our study included a total of 300 paired observations.
Statistical AnalysisThe correlation between the 2 imaging modalities was quantified with use of either the Pearson or Spearman correlation coefficient, depending on the data distribution. Furthermore, Bland-Altman plots were utilized to assess the agreement between the 2 methods, to visualize outliers, and to detect potential systematic bias. These plots illustrate the 95% limits of agreement, determined by the mean difference ± 1.96 standard deviations (SDs), and indicate the expected range of agreement within which the measurements from both methods were anticipated to fall. To evaluate interobserver agreement, intraclass correlation coefficients were calculated with use of a 2-way mixed-effects model with absolute agreement. To identify factors contributing to larger discrepancies between the 2 imaging modalities, hierarchical multivariable linear regression models were employed. These models adjusted for demographic factors (age and gender), time between scans, the CRA, and the magnitude of the original deformity (the preoperative JLCA angle). Additionally, to assess the agreement between LLRs and CT scanograms across different levels of variables that were associated with larger discrepancies in the multivariable model, we calculated and plotted the mean difference between the 2 modalities for each radiographic parameter at various levels of the variables. We implemented a systematic approach starting at a threshold of 1 and proceeding with sequential 1-unit increases. This approach allowed a granular analysis of how agreement changed with incremental differences in a variable. For each threshold, a subset of the cohort was selected on the basis of observations that fell within the positive and negative values of the threshold. The mean difference between the imaging modalities was then calculated for these subgroups. A 2-tailed p value of <0.05 was set as the level of significance.
ResultsThe mean age of our study population was 69 years (range, 40 to 87 years), and female patients constituted 41% of the total cohort (Table II). Most (83.7%) of the patients underwent TKA. The remaining patients underwent UKA, which involved the medial compartment in 95.9% of those patients. The median JLCA based on an anteroposterior radiograph of the arthritic knee was 3.4° (quartile 1 to quartile 3, 1° to 5°). The median CRA was 5° (quartile 1 to quartile 3, 1.2° to 10.5°).
TABLE II - Baseline Characteristics and Demographics of the Study Cohort (N = 300)* Variable Patients Undergoing Robotic-Arm-Assisted TKA or UKA Age (yr) 69 (40-87) Gender (no. [%] of patients) Female 122 (40.7) Male 178 (59.3) Laterality (no. [%] of patients) Right 155 (51.7) Left 145 (48.3) Procedure (no. [%] of patients) TKA 251 (83.7) UKA 49 (16.3) Medial 47 (95.9) Lateral 2 (4.1) JLCA†(deg) 3.4 (1, 5) Preoperative intra-articular deformity (no. [%] of patients) Valgus (JLCA < −0.5°) 45 (15) Neutral (−0.5° ≤ JLCA ≤ 0.5°) 19 (6.3) Varus (JLCA > 0.5°) 236 (78.7) CRA (deg) 5 (1.2, 10.5) KL grade, medial compartment (no. [%] of patients) 0 0 1 1 (0.3) 2 38 (12.7) 3 89 (29.7) 4 172 (57.3) KL grade, lateral compartment (no. [%] of patients) 0 1 (0.3) 1 22 (7.3) 2 118 (39.3) 3 120 (40) 4 39 (13) Time between LLRs and CT scanogram (days) 0 (0, 40)*Categorical variables are presented as the absolute number, with the percentage in parentheses. Continuous variables are presented as the median, with quartiles 1 and 3 in parentheses, except for age, which is given as the mean, with the range in parentheses. KL = Kellgren-Lawrence system for the classification of osteoarthritis.
†Based on an anteroposterior knee radiograph.
Table III displays the radiographic measurements obtained from the 2 imaging modalities. The median HKA was 174.6° (quartile 1 to quartile 3, 171.8° to 179.1°) on LLRs and 174.8° (quartile 1 to quartile 3, 171.6° to 179°) on CT scanograms, with a mean difference of 0.37°. The mean aHKA was −1° on LLRs and −2.3° on CT scanograms, with a mean difference of 1.3°. The mean JLO was 175.20° on LLRs and 174.45° on CT scanograms, with a mean difference of 0.75°.
TABLE III - Comparison of Radiographic Measurements Between LLRs and CT Scanograms Variable LLR*(deg) CT Scanogram*(deg) Mean Difference ± SD (deg) Correlation Coeff. P Value HKA 174.6 (171.8, 179.1) 174.8 (171.6, 179) 0.37 ± 2.6 0.912† <0.001 LDFA 88.13 ± 3 88.39 ± 3.2 −0.26 ± 1.6 0.871‡ <0.001 MPTA 87.1 ± 3.3 86 ± 3.7 1.1 ± 2.1 0.820‡ <0.001 aHKA −1 ± 5.1 −2.3 ± 5.3 1.3 ± 2.5 0.883‡ <0.001 JLO 175.20 ± 3.9 174.45 ± 4.4 0.75 ± 2.7 0.778‡ <0.001 JLCA 3.3 (0.8, 5.3) 2 (0.3, 3.2) 1.1 ± 2.3 0.690† <0.001*Variables are presented as the mean ± SD or as the median with quartiles 1 and 3 in parentheses.
†Spearman correlation coefficient.
‡Pearson correlation coefficient.
The intraclass correlation coefficient ranged from 0.952 to 0.988 for the different variables, suggesting excellent interobserver agreement. Table III demonstrates the correlation between LLRs and CT scanograms across various metrics utilized to characterize the lower-limb constitutional alignment. The results collectively suggested a strong and significant correlation (p < 0.001) between the 2 imaging modalities for all studied parameters. The JLCA was the metric with the weakest correlation, but it still demonstrated substantial agreement (Spearman correlation, 0.690).
Figure 4 illustrates the Bland-Altman plots for the different variables. The percentage of observations that fell within the limits of agreement was 96.6% for the MPTA, 95.7% for the aHKA, 94.3% for the LDFA, 94.6% for the HKA, and 94% for the JLCA.
 Fig. 4:
Fig. 4: Bland-Altman plots for the JLCA, LDFA, MPTA, and aHKA. The solid red lines represent the 95% limits of agreement (±1.96 SDs), and the solid blue line represents the mean.
Sensitivity AnalysisA subgroup analysis was conducted to evaluate the impact of the initial deformity on the agreement between the 2 imaging techniques. Separate correlational analyses were performed for patients with an initial varus deformity (i.e., a JLCA of >0° on a weight-bearing anteroposterior radiograph) and those with an initial valgus deformity (i.e., a JLCA of <0° on a weight-bearing anteroposterior radiograph). The findings suggest that the correlation for the aHKA was comparable between valgus and varus knees (correlation coefficients of 0.855 and 0.844, respectively) but that the correlation for most of the other measured variables was marginally weaker for valgus knees, with correlation coefficients ranging from 0.412 for the JLCA to 0.845 for the LDFA (Table IV).
TABLE IV - Correlation of Radiographic Measurements Between LLRs and CT Scanograms of Knees with a Preoperative Varus or Valgus Intra-Articular Deformity Variable Preoperative Varus Intra-Articular Deformity* Preoperative Valgus Intra-Articular Deformity† LLR‡(deg) CT Scanogram‡(deg) Correlation Coeff. P Value LLR‡(deg) CT Scanogram‡(deg) Correlation Coeff. P Value HKA 173.8 (171, 176.7) 173.9 (170.9, 176.5) 0.873§ <0.001 186.65 (181.92, 190.2) 184.3 (181.4, 187.1) 0.839§ <0.001 LDFA 88.76 ± 2.64 89 ± 2.89 0.862# <0.001 85.17 ± 3.1 85.4 ± 2.7 0.845# <0.001 MPTA 86.50 (84.8, 88.3) 85.4 (83.1, 87.5) 0.826§ <0.001 89.60 ± 2.7 89.2 ± 2.7 0.797# <0.001 aHKA −2.2 ± 4.3 −3.6 ± 4.6 0.844# <0.001 4.4 ± 4.3 3.7 ± 4.1 0.855# <0.001 JLO 175.3 ± 4 174.4 ± 4.5 0.825# <0.001 174.80 ± 3.7 174.6 ± 3.6 0.769# <0.001 JLCA 4 (2.4, 5.7) 2.25 (1.2, 3.6) 0.518§ <0.001 −2.1 (−3.47, −0.72) −1.35 (−2.07, −0.52) 0.412§ 0.002*A JLCA of >0° on a weight-bearing radiograph.
†A JLCA of <0° on a weight-bearing radiograph.
‡Variables are presented as the mean ± SD or as the median with quartiles 1 and 3 in parentheses.
§Spearman correlation coefficient.
#Pearson correlation coefficient.
After adjustments were made for age, gender, the time between scans, and the CRA, linear regression models showed that the magnitude of the original deformity (i.e., the absolute value of the JLCA on a weight-bearing anteroposterior radiograph) was significantly associated with the absolute difference in JLCA measurements between LLRs and CT scanograms (β = 0.220; 95% confidence interval [CI], 0.132 to 0.308; p < 0.001).
After adjusting for age, gender, laterality, preoperative deformity (JLCA), and the time between scans, the absolute value of the CRA was associated with the discrepancy in MPTA measurements between LLRs and CT scanograms (β = 0.064; 95% CI, 0.037 to 0.091; p < 0.001). An association between the absolute value of the CRA and the error in measurements was also noted for the HKA (β = 0.049; 95% CI, 0.019 to 0.079; p = 0.002), JLO (β = 0.094; 95% CI, 0.061 to 0.128; p < 0.001), and aHKA (β = 0.038; 95% CI, 0.007 to 0.069; p = 0.017). No significant association was found for the LDFA (β = 0.14; 95% CI, −0.004 to 0.033; p = 0.132) or JLCA (β = −0.005; 95%, CI −0.034 to 0.023; p = 0.715).
Evaluating Agreement at Different JLCA and CRA ThresholdsTo evaluate agreement between the imaging modalities at different levels, we calculated and plotted the mean difference for each radiographic parameter at various thresholds of the CRA and the JLCA (Tables V and VI, Figs. 5 and 6).
TABLE V - Mean Differences in Radiographic Measurements Between CT Scanograms and LLRs at Different Thresholds of the Absolute CRA* CRA Threshold MPTA LDFA JLCA JLO aHKA HKA 1 −0.584 −0.188 −2.332 −0.772 −0.396 0.964 2 −0.730 0.063 −1.153 −0.611 −0.793 0.472 3 −0.858 0.291 −1.301 −0.480 −1.149 0.473 4 −0.753 0.271 −1.318 −0.4140 −1.045 0.292 5 −0.651 0.259 −1.279 −0.353 −0.926 0.289 6 −0.659 0.331 −1.244 −0.294 −1.006 0.152 7 −0.724 0.321 −1.121 −0.376 −1.059 −0.013 8 −0.731 0.327 −1.134 −0.379 −1.071 −0.076 9 −0.740 0.327 −1.108 −0.389 −1.079 −0.128 10 −0.776 0.319 −1.014 −0.434 −1.106 −0.182 11 −0.743 0.342 −0.998 −0.379 −1.110 −0.179 12 −0.812 0.342 −0.995 −0.449 −1.178 −0.209 13 −0.785 0.350 −1.065 −0.415 −1.158 −0.205 14 −0.805 0.336 −1.102 −0.448 −1.163 −0.189 15 −0.811 0.326 −1.108 −0.467 −1.158 −0.188 16 −0.839 0.310 −1.113 −0.510 −1.169 −0.214 17 −0.824 0.315 −1.110 −0.490 −1.158 −0.211 18 −0.886 0.346 −1.116 −0.521 −1.252 −0.257 19 −0.891 0.335 −1.124 −0.537 −1.244 −0.271 20 −0.975 0.290 −1.152 −0.666 −1.281 −0.274 21 −1.009 0.282 −1.160 −0.709 −1.308 −0.326 22 −1.018 0.285 −1.165 −0.715 −1.319 −0.318 23 −1.023 0.287 −1.176 −0.719 −1.327 −0.316 24 −1.023 0.287 −1.176 −0.719 −1.327 −0.316 25 −1.014 0.288 −1.170 −0.709 −1.318 −0.311 26 −1.014 0.288 −1.164 −0.708 −1.318 −0.311 27 −1.010 0.272 −1.158 −0.720 −1.299 −0.322 28 −1.006 0.271 −1.159 −0.717 −1.293 −0.320 29 −1.007 0.265 −1.145 −0.725 −1.289 −0.337 30 −1.007 0.265 −1.145 −0.725 −1.289 −0.337 31 −1.007 0.265 −1.145 −0.72
留言 (0)