Background and rationale
Uterine fibroids are common benign tumors in the uterine smooth muscle of reproductive-age women [1]. Patients may be asymptomatic, though some have heavy menstrual bleeding, prolonged menses, dysmenorrhea, pelvic pressure symptom, and anemia [1]. The severity of symptoms depends on the location, size, and number of fibroids. Also, uterine fibroids are sometimes responsible for infertility and early miscarriage [2, 3]. These significantly impact patients’ daily activities and can impair quality of life (QOL) [4, 5].
Uterine fibroids can be treated surgically or with pharmacotherapeutics [1]. Treatment choice depends on the patient’s age, symptoms, and the tumor’s number, size, and location. In addition, the patient’s desire to preserve fertility is vital in determining the treatment plan. Surgical treatments include total hysterectomy, myomectomy, endometrial ablation, uterine artery embolization, transcervical resection, and focused ultrasound surgery. There are three approaches to total hysterectomy and myomectomy: open, vaginal, and laparoscopic. Decades ago, uterine fibroids were considered a disorder in women past childbearing age; thus, a hysterectomy was standard care [6]. However, with the change in women’s lifestyles, such as late marriage and childbirth, women with fibroids may still want to have a child. Thus, myomectomy [1] is considered the preferred surgical procedure. Furthermore, compared to open myomectomy, the laparoscope procedure is preferred because patients usually do not develop a fever, have milder postoperative pain, and have a shorter hospital stay [7]. Thus, minimally invasive laparoscopic myomectomy (LM) is becoming the norm.
In women scheduled to undergo LM, a gonadotropin-releasing hormone (GnRH) agonist or GnRH antagonist may be administered to improve operative outcomes. These agents, as they reduce sex hormone levels and induce amenorrhea, help restore hemoglobin levels, shrink myomas, and improve myoma-related symptoms.
The 2017 Cochran Collaboration Systematic Review of therapy before surgery for uterine fibroids reported that GnRH agonist therapy compared to placebo, improved intraoperative and postoperative outcomes of LM [8]. These were a shorter operative time, a decrease in intraoperative blood loss that reduces the risk of developing postoperative anemia, and a decrease in uterine and fibroid volume. In addition, another meta-analysis of GnRH agonists versus placebo before LM reported a decrease in intraoperative blood loss and an increase in postoperative hemoglobin levels [9].
However, GnRH agonists such as leuprorelin induce an initial transient increase in GnRH levels (flare-up) with a subsequent reduction in sex hormones triggering GnRH receptor downregulation and desensitization. On the other hand, the competitive GnRH receptor antagonist relugolix does not trigger a flare-up, and its effects are immediate.
Relugolix is a small-molecule oral GnRH antagonist used to treat uterine fibroids and endometriosis in Japan. In a Japanese phase 3 study comparing relugolix and leuprorelin treatments in patients with uterine fibroids and heavy menstrual bleeding [10], the noninferiority of relugolix to leuprorelin in reducing the bleeding was confirmed. In addition, both groups had similar efficacies in reducing the size of uterine fibroids. Furthermore, the severity and incidence of adverse events (AEs) were similar in the relugolix and leuprorelin groups.
Japan Society of Gynecologic and Obstetric Endoscopy and Minimally Invasive Therapy (JSGOE) Guidelines for Endoscopic Surgery in Obstetrics and Gynecology [6] reports that the oral GnRH antagonist relugolix available in 2019 can now be prescribed to treat patients with uterine fibroids. Unlike GnRH agonists, this formulation does not cause a flare-up and can improve uterine fibroid symptoms and potentially reduce fibroid volume. However, preoperative use of relugolix in patients undergoing LM has not been tested in a randomized controlled trial (RCT).
Objectives
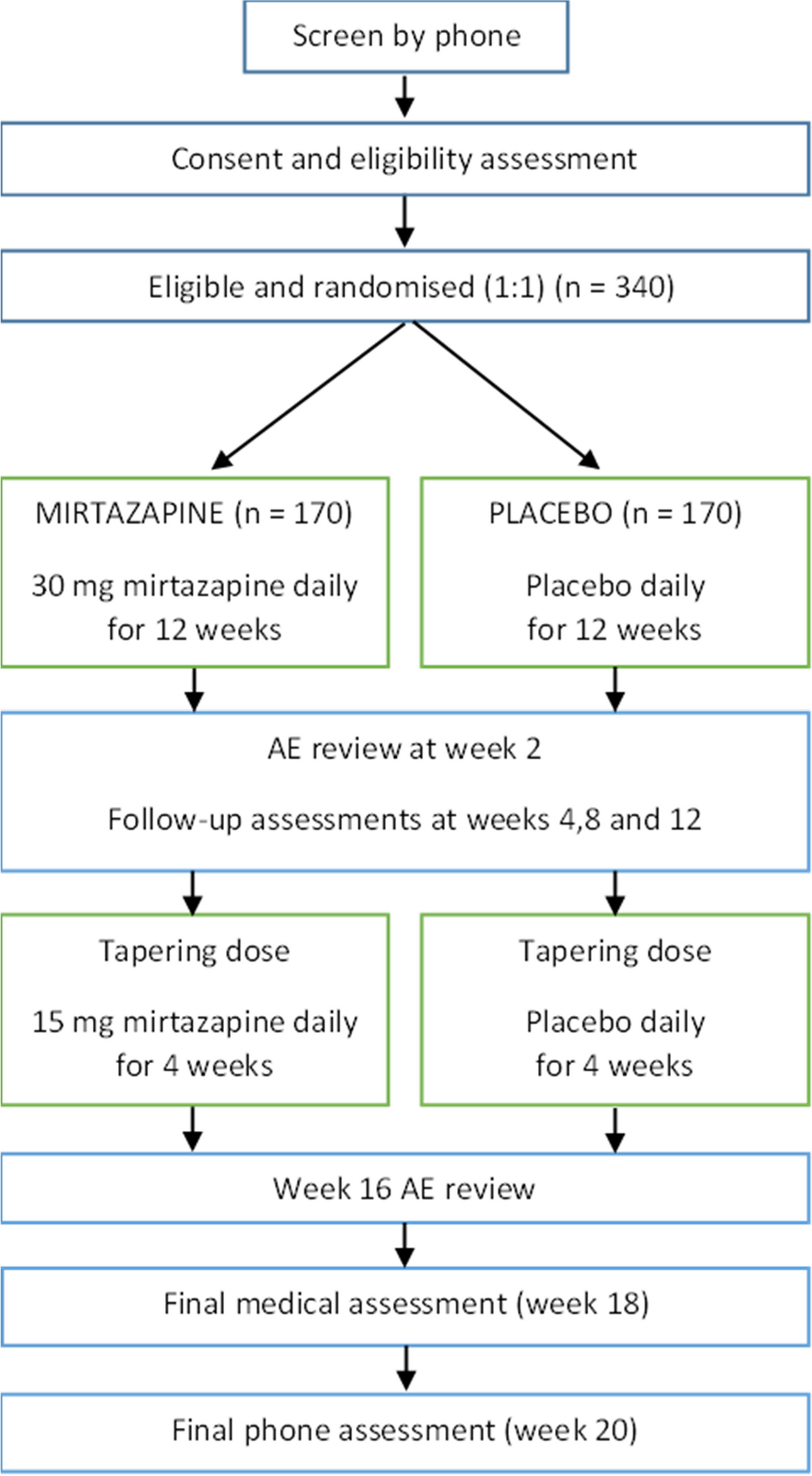
Thus, with the overall aim of improving operative outcomes of LM, the study’s hypothesis is to test the 12-week preoperative noninferiority of relugolix (40 mg orally, once daily) versus leuprorelin (1.88 mg, or 3.75 mg, three injections, once every 4 weeks) to reduce intraoperative blood loss.
Secondary objectives are to (1) assess other surgical outcomes besides intraoperative bleeding, (2) measure changes in fibroid size and uterine volume, (3) measure changes in hemoglobin levels, and (4) observe changes in menopausal-like symptoms, disease-specific QOL, and the safety of treatments.
Trial design
The design is a multi-center, randomized, parallel-group, noninferiority trial, which will be conducted as a “specified clinical trial” according to the Clinical Trials Act in Japan. Randomization will be performed using the minimization method with a 1:1 allocation of participants to receive relugolix or leuprorelin.






留言 (0)