
記住我

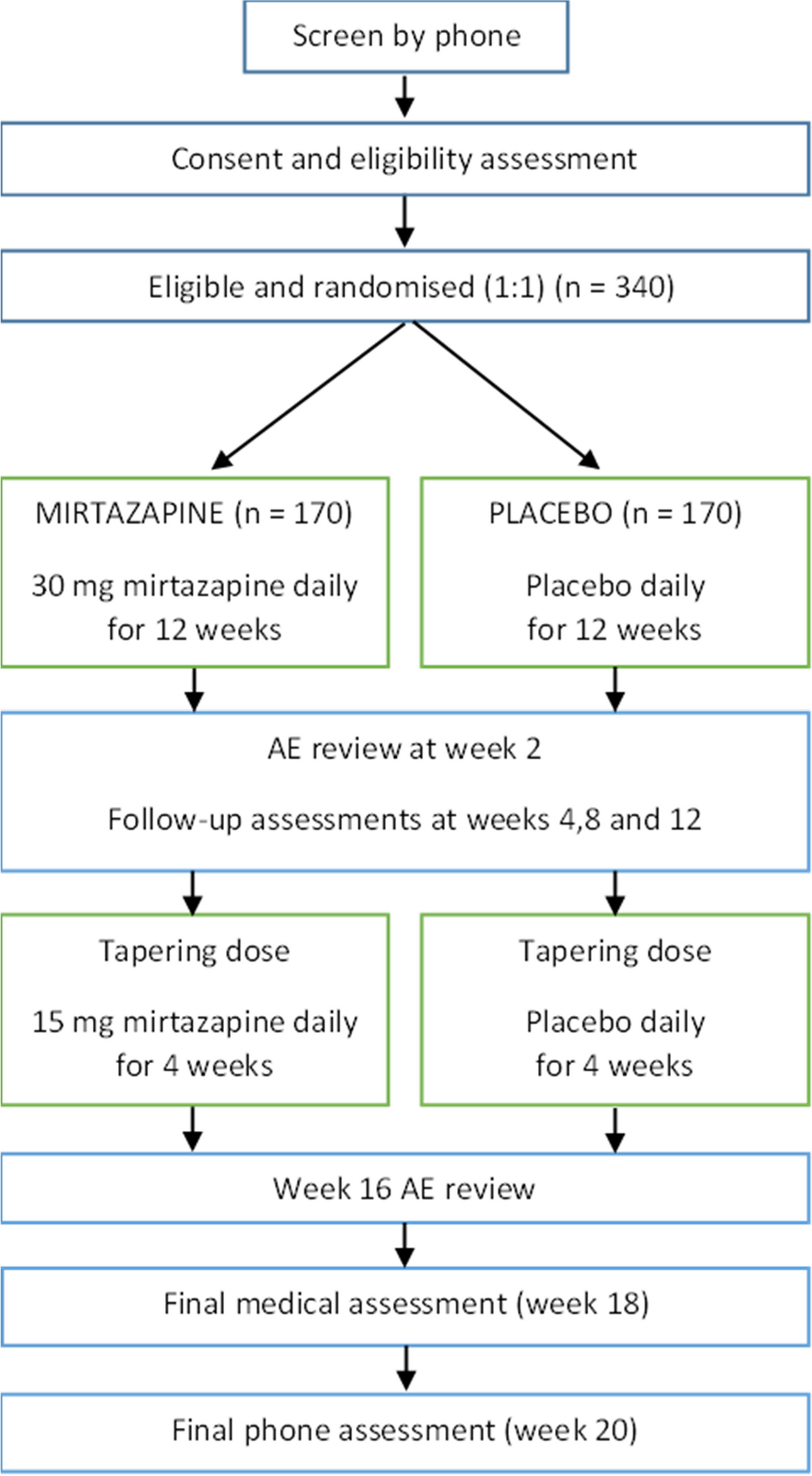




The MRC recommendations used to conceptualise the complex intervention components includes applying a theory-based approach to guide the process evaluation. We will apply two theoretical frameworks: the Theoretical Domains Framework (TDF) [14] and Reach Effectiveness, Adoption, Implementation and Maintenance (RE-AIM) [15], to analyse results and synthesise findings from qualitative and quantitative data collection methods. The study design and timepoints of measurement are in Fig. 1 and Table 1.
Fig. 1
Process evaluation design and conduct. mILOA, Modified Iowa Level of Assistance Score; EQ-5D-5L, EuroQol 5D-5L; ICECAP-O, ICEpop CAPability measure for Older people; short FES-I, Short Falls Efficacy Scale—International
Table 1 Schedule of trial follow-up and proceduresTo determine translation and behaviour change success of HIPSTER, the RE-AIM framework will be applied. This framework effectively evaluates public health interventions by assessing outcomes against five key dimensions: Reach, Effectiveness, Adoption, Implementation and Maintenance [16]. We will report on all domains across individual and organisational levels, where appropriate [15, 16]. The outcomes assessed (Table 2) include participant characteristics, participation rates, intervention completion, intervention effectiveness and characteristics of staff delivering the intensive physiotherapy. Key outcomes will be reported and analysed according to the clinical protocol [10]. Categorical data will be summarised in counts and percentages, with numerical data summarised as either means and standard deviations or medians and interquartile range depending on distribution of data. Qualitative data will be analysed using thematic analysis. The TDF will be applied to understand individual behaviour change success. The TDF is a framework combining different theories of behaviour change to identify factors affecting healthcare professional behaviour and guide more targeted implementation interventions [17]. It will be used as a coding framework to understand clinician responses to the pre- and post-implementation surveys [14, 18].
Table 2 RE-AIM elements and outcomes assessedProcess evaluation design and conductA mixed methods study design will be undertaken in parallel to the HIPSTER trial to evaluate the process of HIPSTER at the intervention level, patient and carer level and clinician level.
Intervention levelTo determine translation at an intervention level, the RE-AIM framework will be applied. A site initiation visit will be completed, providing education about current evidence, existing gaps in the literature and aims of the HIPSTER Trial. No additional training will be provided for staff delivering the intervention. The intervention therapy delivered will be determined by the physiotherapist’s assessment of the individual patient. The physiotherapy review will aim to progress functional gains achieved in the usual care session including increasing independence with mobility, gait aid progression and increasing walking distance. The allied health assistant review will practice achievements gained during the usual care review. The key difference in management between usual care and the intervention group is the increased frequency of physiotherapy and allied health assistant sessions. There should be no change to usual care with all discharge and follow-up determined by usual practices at the site. We will assess any changes to usual care over the course of the trial, including changes to clinician behaviours. Sites will maintain an intervention log for each participant randomised to the intervention group. Staff delivering the intervention will complete it at the end of each session. The intervention log will contain the number of intervention sessions delivered per resource (Physiotherapist or Allied Health Assistant), the duration of the session (minutes) and a brief description of the intervention provided (e.g. ambulation, exercises). Any missed intervention sessions will be documented, and an explanation provided. These data will track intervention fidelity and be summarised by percentage of planned sessions delivered. Intervention completion will be defined as those that received their designated therapy for at least 4 days in the acute hospital.
The key components of the intervention assessed by RE-AIM are outlined in Table 2. The reach of the intervention will be determined by the percentage of eligible participants who participate and their characteristics. Intervention effectiveness will be evaluated by clinical outcomes (Table 1 and Fig. 1) as explained in our trial protocol [9], adverse events and patient experience (semi-structured interviews with questions focussing on the perceived effect of the intervention). The primary clinical outcome is total hospital length of stay (days). Secondary clinical outcomes include functional mobility assessed by the Modified Iowa Level of Assistance Score (mILOA) and completed on day 7 following surgery; health-related quality of life and falls efficacy will be assessed at all follow-up timepoints and measured through EuroQol 5D-5L (EQ-5D-5L), ICEpop CAPability measure for Older people (ICECAP-O) and Short Falls Efficacy Scale—International (FES-I). Healthcare utilisation and the associated costs will be collected through monthly phone calls with the participant, and the collection of health systems costs from Health Services Australia Data (incorporating Medical Benefits Schedule and Pharmaceutical Benefits Scheme) over the 12-month follow-up period. Adverse events as defined by GCP standards will include hip and non-hip related in-hospital and out-of-hospital events. The Adoption of the intervention including health care professional characteristics, experience and perspectives of intensive therapy will be gathered through pre- and post-clinician surveys. We will record intervention completion, the number and components of the intervention delivered including total physiotherapy and allied health assistant time and adaptations made for implementation. Maintenance at an individual level will be measured by patient outcomes across at 12 months following surgery (e.g. quality of life measured using EQ-5D-5L) as well as the participant and carer experience of the intervention and the factors supporting their recovery. Maintenance at an organisational level will be measured by intention to continue delivering the intervention at 6 months following trial completion, including local funding models and modifications made, and the intensity of the intervention delivered.
Participant and carer levelClinical outcomes and their collection method are explained in detail in our published protocol [9]. Eligible patients will be approached to consent to the trial during the perioperative phase. They will be included if they fulfil the following criteria: age \(\ge\) 65 years old, admitted from home with a hip fracture (either subcapital or intertrochanteric) and managed surgically. They will be excluded if they were unable to mobilise (with or without a gait aid prior to the surgery) and are not allowed to full-weight-bear or weight-bear-as-tolerated. Once consented, baseline data will be collected at hospital admission with key follow-up assessment timepoints occurring at day 7, 6 weeks, 120 days and 12 months following surgery. At initial study consent, participants or their proxy decision-maker will be invited to participate in semi-structured interviews at 6 weeks following surgery. At the 6-week review with the blinded assessor, participants or their carers will be asked if they consent to be contacted by an experienced qualitative researcher who is independent of the site clinical and research staff. Those who consent and are eligible (have recall of the acute inpatient hospital admission) will be contacted to participate in a semi-structured interview. The participants will be asked about their experience of intensive therapy and their recovery and discharge from hospital as well as barriers and facilitators to participation in the intervention, with an interview guideline developed using RE-AIM framework (supplementary material A). Interviews will be conducted via the telephone, at a time of the participant’s preference. A sampling framework will be applied to ensure diversity across hospital, gender and presence of a carer. Interviews will be transcribed verbatim within 6 weeks of completion of the interview. All participant discussions and responses will be coded to ensure participants cannot be identified from their responses. Two researchers will independently undertake line by line analysis of the coded transcripts, to generate descriptive themes [19]. The two researchers will refine the descriptive codes into themes and subthemes through iterative discussion [20]. Representative quotes from participants will be used to illustrate the identified themes. Interviews will continue until data saturation is reached, i.e. when no new themes emerge from consecutive interviews.
Clinician levelPre-implementation and post-implementation clinician surveys linked to domains of the TDF will explore behaviours that act as barriers and facilitators to implementation of HIPSTER. Any clinician involved in the care of patients following hip fracture will be invited via email to anonymously participate in an online survey (Qualtrics®, UT, USA) by their site principal investigator prior to the commencement of recruitment. The pre-implementation online survey will comprise 25 questions each relating to the domains of the TDF (Table 3) as well as an additional five questions relating to the study protocol. Participants will be asked to rate level of agreement to a statement using a six-level Likert scale ranging from ‘completely agree’ to ‘completely disagree’. These same questions will be repeated in the post-implementation survey. Free text options will also allow clinicians to list any perceived barriers and facilitators to implementation of intensive therapy following hip fracture. The post-implementation survey will be distributed 7 days following completion of participant recruitment to prevent unblinding staff. The survey will include an additional 28 statements and short answer questions relating to barriers and facilitators to implementation, suitability of the site and trial design and likelihood to continue providing high-intensity therapy following hip fracture. In both surveys, we will collect demographic information about the clinician, their qualifications, years of experience and professional delegation. We will aim to collect at least the same number of pre-implementation and post-implementation surveys from each of sites.
Table 3 Survey evaluation of clinician perspective on providing intensive physiotherapy following hip fracture surgerySurvey responses will be reported descriptively with the number and proportion of respondents. Themes emerging from free text responses will be mapped to the TDF components [14]. The comparison of pre- and post-implementation survey responses will enable differentiation between perceived and experienced barriers and facilitators, which will be used to guide future implementation. These clinician experiences will help with the creation of interventions and an implementation toolkit to target key behaviours of change with the goal of facilitating sustainable implementation.
Logic modelAs per best-practice methods for evaluation of complex interventions [10], a logic model was created outlining key factors that may influence implementation, proposed causal mechanisms and target outcomes (Fig. 2).
Fig. 2
Logic model for the process evaluation of HIPSTER
留言 (0)