
記住我





Low back pain (LBP) is an increasingly prevalent musculoskeletal disorder, with a lifetime prevalence of 84%.38 Low back pain was responsible for 63.7 million years of living with disability worldwide in 2019.3 Serious pathologies or specific causes contribute only 10% of LBP presentations.18 Most LBP presentations are nonspecific, a reflection of the intricate interplay of biopsychosocial factors and comorbidities.11
The management of LBP is a major challenge in clinical practice due to its recurrent nature, varying pain intensities, and different biopsychosocial factors. Historically, the approach to LBP management has relied on a temporal classification system that categorizes pain into acute (less than 6 weeks), subacute (6–12 weeks), and chronic (more than 12 weeks) phases.36 Initially, this classification system was based on the assumption that acute, nonspecific LBP leads to significant recovery shortly after onset.4 Understanding the heterogeneity of LBP presentations necessitates a shift away from traditional classification systems.19 It calls for more individualized approaches that can accurately reflect the nonlinear and variable trajectories acute LBP can undertake over time,9,19 with many individuals experiencing recurrences5 and incomplete recovery.14 Analytical approaches such as latent class analysis (LCA) have come to the forefront to capture the complex transitions typical of LBP trajectories, focusing on individual pain reports rather than broad time-based categories.2,7,8,20
Emerging research using LCA to identify individual trajectories in acute LBP has begun highlighting the diversity of trajectories and the influence of different biopsychosocial factors at baseline. Downie et al.6 evaluated 1585 patients over 12 weeks and found 5 pain trajectory groups. These were rapid recovery by week 2 (35.8%), recovery by week 12 (34.3%), incomplete recovery (14.0%), fluctuating pain (10.5%), and persistent high pain (5.4%). Factors such as higher pain intensity and workers' compensation correlated with the persistent high-pain group, and beliefs about pain persistence were associated with nonrecovery. Schuller et al.,31 who studied 1377 LBP patients with mixed pain durations over 6 months, identified 3 trajectories: persistent high pain (n = 226), persistent pain with substantial improvement (n = 578), and mild pain with moderate improvement (n = 313). Baseline factors such as male gender and previous specialist consultations had limited predictive value. Da Silva et al.32 studied 542 older adults over 12 months, distinguishing 3 trajectories: pain recovery (n = 31), incomplete recovery (n = 253), and persistent severe pain (n = 258). Factors such as low education and depressive symptoms correlated with the persistent severe LBP trajectory.
However, there is a paucity of inception cohort studies investigating the trajectories from the onset of a new episode of acute LBP over one year. To address this knowledge gap, the primary objective of our study was to conduct a community-based inception cohort study to identify distinct individual trajectories of participants with a new episode of acute LBP over one year, including participants who do not necessarily seek professional health care because of their acute LBP. Our secondary objective was to quantify the association of biopsychosocial variables at baseline with trajectory class membership.
2. Methods 2.1. Study design and settingWe conducted a longitudinal, community-based, inception cohort study to evaluate the course of acute LBP over 52 weeks. Low back pain was defined as pain between the lower edge of the 12th rib and the gluteal folds, with or without radiating pain to one or both legs.16 The study was conducted at 5 participating sites. Baseline data were collected within 4 weeks of LBP onset. Follow-up data were obtained 8, 12, 26, and 52 weeks after LBP onset. All participants gave informed consent before their first examination. The study adhered to the tenets of the Declaration of Helsinki and was approved by the local ethics committee (BASEC-No. 2016-02096). We followed the guidelines for reporting on latent trajectory studies (GRoLTS) for data analysis and reporting35 and a recently published framework for constructing and interpreting latent class trajectory models.24
2.2. Recruitment and eligibility criteriaWe recruited participants through advertisements (newspapers, flyers, mailing lists, word of mouth, local university websites, and nearby local hospitals and private practices). Participants were eligible if they (1) had acute LBP with or without leg pain of less than 4 weeks duration (in the case of a recurrent episode, participants had to be pain-free for at least 3 months before the acute pain onset), (2) were between 18 and 65 years of age, (3) had Internet access, and (4) were able to read and understand German. Participants were excluded if they met any of the following criteria: evidence of severe pathology (LBP because of trauma, tumor, infection, anomaly, or evidence of cauda equina syndrome), history of LBP surgery, current psychological problems requiring psychological treatment, and current pregnancy or first year postpartum. Eligibility criteria were determined by telephone or e-mail, and reasons for exclusion were not recorded. Investigators reconfirmed eligibility criteria before the first clinical evaluation.
2.3. Data collectionData collection included clinical assessments and online surveys, although the results of the clinical assessments are not reported in this analysis. Pain intensity as primary outcome was derived at baseline and follow-up time points from the mean of 3 self-reported 11-point numeric rating scales (NRS) for current, worst, and average pain in the past week. Online surveys included sociodemographic data (age, sex, education level, work status, and quality of life). In addition, we collected LBP-related factors on pain frequency, previous LBP episodes, referred pain, pain localization, treatment, medication, imaging, and disability (Oswestry disability index [ODI]).26 Psychological factors such as illness perception (illness perception questionnaire [IPQ]27), avoidance/endurance behavior (avoidance endurance questionnaire [AEQ]12), pain vigilance (pain vigilance awareness questionnaire [PVAQ]23), depression and stress (Depression Stress Anxiety Scale [DASS]28), anxiety (State-Trait Anxiety Inventory [STAI]33), and risk of developing persistent pain (Keele Start Back Screening Tool [STarT])17 were collected. A detailed description of the measures and a data collection schedule can be found in Supplementary files 1 (Table S1, https://links.lww.com/PR9/A228) and 2 (Table S2, https://links.lww.com/PR9/A228). Dropout was defined as missing data at 2 consecutive time points or a participant's withdrawal from the study, with reasons for withdrawal ascertained.
2.4. Statistical analysisDescriptive statistics characterized the sample at baseline. The statistical analysis included 2 phases to meet the study's objectives. A sensitivity analysis was conducted to compare baseline characteristics between participants who were retained and those who dropped out.
2.5. Phase 1: latent class linear mixed modelWe used a latent class linear mixed model (LCMM) to identify homogeneous latent class pain trajectories over time. Latent class linear mixed model extends linear mixed models and latent class growth analysis by accounting for individual variability and latent group structure.29 The time metric was measured in weeks since the onset of acute LBP (according to follow-up time points). Pain intensity as a dependent variable was measured on a continuous scale. The LCMM assumes that data are missing at random (MAR) using maximum likelihood estimation.
First, we used spaghetti plots to inspect individual pain trajectories over time visually. We then applied a stepwise procedure assuming one underlying latent class (G = 1) in the study population. We then tested additional models by increasing the latent classes (G > 1–5) to derive the best model fit for the data. We included linear, quadratic, and cubic time as fixed-effects terms in all our models (G 1–5) to account for nonlinear growth trajectories over time. The LCMM approach capitalized on its inherent flexibility to use all available data, under the MAR assumption. This enabled the inclusion of every participant's data, up to their last available measurement, ensuring comprehensive utilization of the data set despite varying levels of completeness. In addition, the model accounted for random effects associated with time, acknowledging that although there is an overarching pattern of pain over time, individual participants might exhibit unique trajectories. Furthermore, the mixture component of the model, which also incorporated linear, quadratic, and cubic time terms, was employed to detect latent subgroups within the data, identifying distinct pain trajectories over time for these subgroups. An automatic grid search function was performed with a maximum of 30 iterations from 100 random vectors of initial values to avoid converging to local maxima.15 We used Akaike information criterion (AIC),1 the Bayesian information criterion (BIC),10 the size-adjusted Bayesian information criterion (SABIC), and the Lo-Mendell-Rubin likelihood ratio test (LMR-LRT)25 as goodness-of-fit criteria to assess model fit and identify the optimal number of latent classes (G = 1–5). Goodness-of-fit criteria are based on log-likelihood and several parameters to account for model complexity. Lower BIC, AIC, and SABIC values and significant LMR-LRT tests indicate better model fit. After model selection, the average posterior probability assignment (APPA), the odds of correct classification (OCC), and relative entropy were used to assess model adequacy, with APPA greater than 0.7, OCC greater than 5.0, and relative entropy greater than 0.5 considered acceptable.24 Other criteria were a minimum class proportion of 5% and clinical relevance of latent class trajectories. The R code used for the LCMM and model comparisons is provided in Supplementary Material S4, https://links.lww.com/PR9/A228.
2.6. Phase 2: multinomial logistic regression analysisMultinomial logistic regression analysis was used to model the latent class membership as a linear function of a priori selected biopsychosocial factors at baseline, whereas the most favorable class served as the reference category. An OR >1 means that a one-unit increase in the independent variable is associated with an increased chance of being assigned to the current class compared with the reference class. We tested for multicollinearity by calculating correlations between independent variables. Categorical independent variables were dichotomized (see Supplementary Material S1, Table S1, https://links.lww.com/PR9/A228).
First, univariable multinomial logistic regression analysis was performed to calculate unadjusted ORs with 95% confidence intervals (95% CI) to identify significant associations of independent variables with latent class membership. Second, multivariable multinomial regression analysis was performed to calculate adjusted ORs with 95% CI for the effects of the remaining significant variables. We used a penalized version of multivariable analysis to account for perfect separation problems. All analyses were performed with the statistical software R (v. 4.0.5, packages “lcmm,”29 “LCTMtools,”24 “tidyLPA,”30 “nnet,”37 “arsenal,”13 “brglm2”21 and “detectseparation”22).
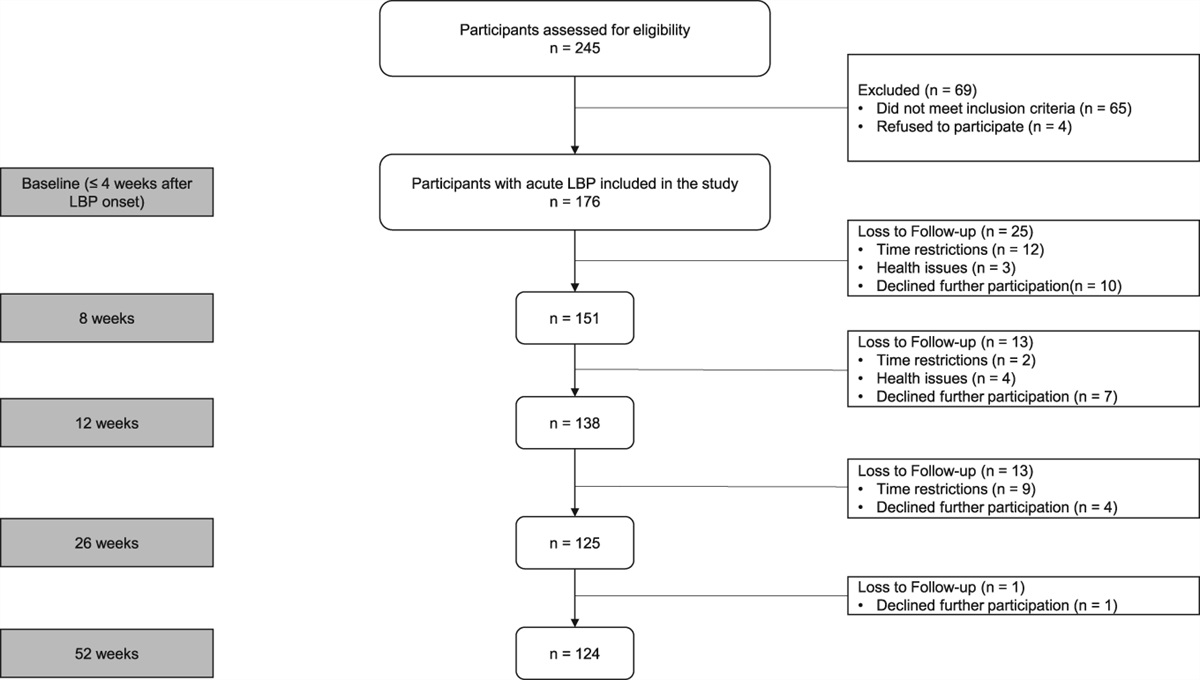
3. ResultsFigure 1 shows the study flow chart. A total of 176 participants (mean age 39.1 years, 50.9% female) with acute LBP were enrolled between November 2017 and February 2021. Overall, cumulative loss to follow-up was 25 (14.2%), 38 (21.6%), 51 (28.9%), and 52 (29.5%) at 8, 12, 26, and 52 weeks, respectively. In our analysis, 141 of the total 176 participants had at least 3 follow-up measurements, providing a robust data set for the LCMM to effectively capture the trajectories over time. Table 1 shows sample characteristics at baseline.
 Figure 1.:
Figure 1.: Flowchart of participants through the study.
Table 1 - Baseline sample characteristics for each class of the final 4-class model. All participants (n = 176) Class 1 = mild/moderate fluctuating pain (n = 95) Class 2 = delayed recovery by week 52 (n = 11) Class 3 = persistent moderate pain (n = 58) Class 4 = moderate/severe fluctuating pain (n = 12) P Sociodemographic variables Age (y)* 39.3 (13.2) 39.7 (13.2) 41.1 (13.9) 36.6 (12.5) 47.5 (12.9) 0.059 Female (%)* 89 (50.9) 42 (44.2) 7 (63.6) 30 (52.6) 10 (83.3) 0.057 Lower educational level (%)* 66 (38.6) 31 (33.7) 5 (45.5) 24 (42.1) 6 (54.5) 0.453 No work (%) 12 (6.8) 7 (7.4) 0 (0.0) 4 (6.9) 1 (8.3) 0.827 ≤Moderate QoL (%)* 72 (40.9) 34 (35.8) 5 (45.5) 25 (43.1) 8 (66.7) 0.209 LBP-related variables Pain (NRS)* 4.6 (1.6) 4.1 (1.4) 5.3 (1.5) 4.7 (1.0) 7.1 (1.5) <0.001 Daily frequent pain (%)* 117 (67.2) 60 (63.2) 7 (70.0) 41 (71.9) 9 (75.0) 0.648 ≥1 previous LBP episode (%)* 134 (77.0) 66 (69.5) 7 (70.0) 52 (91.2) 9 (75.0) 0.020 Referred pain (%) 85 (48.9) 39 (41.1) 8 (80.0) 31 (54.4) 7 (48.9) 0.062 Most disturbing pain region (%)† 0.290 Back 154 (88.5) 82 (86.3) 7 (70.0) 54 (94.7) 11 (91.7) Legs 12 (6.9) 9 (9.5) 1 (10.0) 1 (1.8) 1 (8.3) Pins/needles 5 (2.9) 3 (3.2) 1 (10.0) 1 (2.1) 0 (0.0) Other 3 (1.7) 1 (1.1) 1 (10.0) 1 (1.8) 0 (0.0) Treatment due to LBP (%)*‡ 108 (63.9) 54 (58.1) 8 (80.0) 36 (66.7) 10 (83.3) 0.200 LBP medication (%)*† 77 (44.3) 35 (36.8) 7 (70.0) 28 (49.1) 7 (58.3) 0.097 Imaging (%) 34 (19.3) 19 (20.0) 3 (27.3) 9 (15.5) 3 (25.0) 0.738 Disability (ODI)* 17.0 (10.5) 14.5 (9.4) 19.3 (12.3) 17.4 (8.8) 32.2 (12.5) <0.001 Psychological variables Illness perception: timeline (IPQ)* 2.3 (1.0) 2.2 (1.0) 2.4 (1.2) 2.5 (1.0) 2.5 (0.6) 0.444 Illness perception: control (IPQ)* 1.8 (0.6) 1.7 (0.6) 1.9 (0.5) 1.7 (0.6) 2.0 (0.7) 0.288 Illness perception: reason for pain (%)§ Bodily causes 156 (88.6) 87 (91.5) 7 (63.6) 52 (89.6) 10 (83.3) <0.001 Psychological causes 47 (26.7) 22 (23.2) 3 (27.2) 20 (34.5) 2 (16.7) <0.001 Other causes 25 (14.2) 13 (13.7) 3 (27.2) 8 (13.8) 1 (8.3) 0.003 Endurance behavior (AEQ)* 2.6 (1.1) 2.5 (1.2) 2.3 (1.1) 2.8 (1.0) 2.3 (1.4) 0.176 Avoidance behavior (AEQ)* 3.4 (1.6) 3.5 (1.6) 3.9 (1.8) 3.3 (1.5) 2.6 (1.8) 0.219 Pain vigilance (PVAQ)* 36.9 (11.3) 36.8 (11.2) 38.5 (13.9) 36.4 (10.6) 38.9 (13.7) 0.873 Depression (DASS21)* 5.3 (6.4) 5.1 (6.2) 5.3 (5.5) 4.7 (5.9) 10.2 (9.8) 0.089 Stress (DASS21)* 9.0 (7.0) 8.2 (6.5) 11.6 (7.2) 9.0 (7.2) 11.6 (10.4) 0.278 Anxiety (STAI-S)* 37.6 (10.2) 36.8 (10.4) 39.5 (7.7) 37.5 (9.4) 42.6 (13.9) 0.356 Risk stratification (%, SBT)* <0.001 Low 117 (69.6) 68 (74.7) 6 (60.0) 41 (73.2) 2 (18.2) Medium 42 (25.0) 20 (22.0) 2 (20.0) 14 (25.0) 6 (54.5) High 9 (5.4) 3 (3.3) 2 (20.0) 1 (1.8) 3 (27.3)Numbers are means (standard deviations) of participants unless stated otherwise.
Entries in bold indicate statistically significant P-values (P < 0.05).
*Variables included in the multinomial logistic regression model.
†Categorical data do not sum up to 100% due to missing values.
‡Treatment includes either general practitioner, specialist, pain specialist, psychologist, physiotherapy, massage, or chiropractic consultations due to LBP.
§Multiple answers possible.
AEQ, avoidance endurance questionnaire; DASS21, Depression Anxiety Stress Scale; IPQ, illness perception questionnaire; LBP, low back pain; NRS, numeric rating scale; ODI, Oswestry disability index; PVAQ, pain vigilance and awareness questionnaire; QoL, quality of life; SBT, Start Back Tool; STAI-S, State Trait Anxiety Inventory—State.
After visual inspection of the data (see Supplementary Material 3, Figure S3, https://links.lww.com/PR9/A228) and a significant decrease in AIC and BIC when using cubic time effects in the models, linear and quadratic models were discarded from further analyses. Details of the discarded models are provided in Supplementary Material 3 (Table S3, https://links.lww.com/PR9/A228).
Table 2 shows all models' goodness-of-fit criteria and class proportions (G = 1–5). The 5-class model had the lowest AIC, whereas the 2-class and 4-class models had the lowest BIC values. When sample size was considered, the 5-class model had the lowest SABIC. Relative entropy was adequate for all models, with 0.67, 0.72, and 0.74, respectively. Class proportions were above 5% in all models, whereas the 5-class model had 3 classes with few participants compared with only 2 classes with few participants in the 4-class model. Lo-Mendell-Rubin Likelihood Ratio Test showed a significant improvement in model fit for one additional class for each model included.
Table 2 - Goodness-of-fit criteria and class proportions for 1-class to 5-class models. Goodness-of-fit criteria LMR-LRT (P) Proportions per class % Model G AIC BIC SABIC Relative entropy Class 1 Class 2 Class 3 Class 4 Class 5 M1 1 2774.9 2809.8 2774.6 1.0 — 100 M2 2 2739.4 2790.2 2739.5 0.67 P < 0.001 64.8 35.2 M3 3 2729.5 2796.1 2729.6 0.72 P < 0.002 63.6 6.3 30.1 M4 4 2707.9 2790.3 2707.9 0.74 P < 0.001 54.0 6.2 33.0 6.8 M5 5 2702.7 2801.0 2702.9 0.74 P = 0.014 43.2 8.0 7.4 35.2 6.2Model M1-5 using cubic fixed effects for up to 5 classes.
AIC, akaike information criterion; BIC, Bayesian information criterion; G, number of classes; LMR-LRT, Lo-Mendell-Rubin likelihood ratio test (P values <0.05 indicating statistically significant improvement of model fit for one additional class); SABIC, size-adjusted Bayesian information criterion.
Table 3 shows additional model selection tools. Average posterior probability assignment ranged from 0.79 to 0.91, whereas in the 4-class model, all values were equal to or greater than 0.80. The OCC of all included models was greater than 5. Considering the similarity of the AIC values between the 4-class and 5-class models, the lower BIC value of the 4-class model, adequate additional model selection tools, and clinical relevance, the 4-class model was chosen to best represent acute LBP trajectories over one year in our data.
Table 3 - Additional model selection tools. Number of classes Model 2 Model 3 Model 4 Model 5 APPA OCC APPA OCC APPA OCC APPA OCC Class 1 0.91 5.86 0.89 5.38 0.89 7.44 0.81 10.38 Class 2 0.85 10.45 0.82 51.48 0.81 45.38 0.80 34.17 Class 3 0.79 9.13 0.80 8.76 0.81 40.20 Class 4 0.80 51.25 0.79 8.42 Class 5 0.86 84.56Model 1 not included in the table.
APPA, average posterior probability assignment (overall average probability of assignment to each class, should be >0.7 for each class); OCC, odds of correct classification (ratio of the odds of a correct classification into each class, should be >5.0).
Figures 2 and 3 illustrate the mean predicted trajectories of the final 4-class model and the detailed characteristics of each trajectory of acute LBP. Of the participants, 54.0% (n = 95) followed the “mild/moderate fluctuating pain” trajectory, which showed an initial rapid decrease in mean pain intensity from a baseline of NRS 4.1/10, followed by a pain increase at subsequent measurement points; 6.2% (n = 11) fit the “delayed recovery by week 52” trajectory, starting with a baseline mean pain intensity of NRS 5.3/10 and experiencing a gradual decrease in pain intensity over time. 33.0% (n = 58) matched the “persistent moderate pain” trajectory, maintaining a consistent moderate pain level after an initial mean intensity of NRS 5.3/10. Finally, 6.8% (n = 12) aligned with the “moderate/severe fluctuating pain” trajectory, beginning with a baseline intensity of NRS 7.1/10, with a reduced pain intensity by week 26 but then seeing an increase by week 52.
 Figure 2.:
Figure 2.: Class-specific mean predicted acute LBP trajectories. LBP, low back pain.
 Figure 3.:
Figure 3.: Detailed description of each class.
3.2. Comparison of baseline characteristics within classesPain intensity at baseline differed between classes (P < 0.001), with higher pain intensities reported in less favorable trajectories. More participants in less favorable classes reported having at least one previous episode of LBP (P = 0.020), whereas 23% never had an episode of LBP. Participants assigned to less favorable classes reported more significant disability (P < 0.001) and significant differences were observed in baseline risk stratification for developing persistent pain, as assessed by the SBT, across the different trajectory classes (P < 0.001). There were significant differences between illness perception categories regarding the reasons for pain (P < 0.001).
3.3. Sensitivity analysisOur sensitivity analysis (see Supplementary Material S4, Table S4, https://links.lww.com/PR9/A228) highlighted significant differences between participants who completed the study and dropouts in disability (ODI) scores, work status, and avoidance/endurance behavior (AEQ).
3.4. Multinomial logistic regression analysisThe most favorable latent class, “mild/moderate fluctuating pain,” was a reference class. After testing for collinearity between independent variables, the variable stress was removed from further analyses. Table 4 shows the univariable (unadjusted) and multivariable (adjusted) multinomial logistic regression analysis results.
Table 4 - Multinomial logistic regression models. Baseline predictors Unadjusted OR (95% CI) Adjusted OR (95% CI) Sociodemographic variables Age Mild/moderate fluctuating pain 1.0 (reference) Delayed recovery by week 52 1.01 (0.96–1.06) Persistent moderate pain 0.99 (0.96–1.01) Moderate/severe fluctuating pain 1.05 (1.00–1.10) Sex (female) Mild/moderate fluctuating pain 1.0 (reference) 1.0 (reference) Delayed recovery by week 52 2.21 (0.60–8.05) 1.91 (0.53–6.85) Persistent moderate pain 1.40 (0.72–2.71) 1.81 (0.85–3.82) Moderate/severe fluctuating pain 6.31 (1.31–30.37) 5.07 (0.95–27.16) Educational level (low) Mild/moderate fluctua
留言 (0)