
記住我





Lipedema, also known as lipohyperplasia dolorosa (LiDo), is a widespread bilateral subcutaneous deposition of adipose tissue in limbs and arms but not affecting feet or hands.1,2,11,13,16,19,30,39,44,45,49,51 Depositions are unresponsive to dietary restrictions and physical activity.19,39,50 Lipedema affects almost exclusively women and typically manifests concomitant with hormonal changes, such as puberty, childbirth, or menopause.3,17
Pain or heaviness in affected extremities is considered a lipedema-defining characteristic8,12,21,24,26,43,45 and differentiates lipedema from nonpainful phenotypes such as obesity or lymphedema.8 The etiology of lipedema pain is currently unknown. Patients are mostly unresponsive to analgesics, and this lasting pain greatly aggravates the burden of the disease.21,43
Pain is defined as a physiological sensory and psychological emotional experience.38 The emotional experience of lipedema pain is routinely recorded by pain questionnaires such as “Deutsche Schmerzfragebogen” or “painDETECT.”11,20,33 By contrast, it has not been attempted to characterize, which physiological sensory sensitivities, such as detection of warmth, cold, heat pain, cold pain, and pressure pain, may be changed and to quantify such changes in lipedema patients. Lipedema pain is ill described. It has been described as sensitivity against touch but also as continuous pain. It is described as “if legs would burst from the inside,” “painful weakness,” “piercing, stabbing.”43 It remains unclear which of the clinical pain categories, such as nociceptive, inflammatory, neuropathic, neuroplastic, or psychosomatic pain, may be at the heart of this debilitating condition. An objectifiable characterization of lipedema pain beyond patient self-reporting is currently missing.
Accordingly, we aimed to characterize the somatosensory phenotype in lipedema patients using the standardized approach of quantitative sensory testing (QST) as developed by the German Research Network on Neuropathic Pain (DFNS).32,37,40,41 Conducting 7 tests, 13 different sensory thresholds are determined. Objectivity was assured by standardized training of the measuring personal, averaging over repetitive tests, comparing lipedema patients with unaffected matched controls, as well as measuring the unaffected hands in addition to the affected thigh, which served as patient-specific internal control, and by comparison to DFNS database controls. Finally, yet importantly, we investigated young non-obese patients, which remain largely undiagnosed for decades. The study was accompanied by a standard pain questionnaire to investigate patients' psychometry and pain descriptions to provide a comprehensive analysis of the hallmarks of lipedema pain. The potential of the results for differentiating lipedema from controls was tested by receiver operating characteristic (ROC) analysis and corroborated by Bayesian inference analysis.
2. Materials and methods 2.1. PatientsThis project was conducted in accordance with the Declaration of Helsinki and the ICH E6 Good Clinical Practice (GCP) guidelines, approved by the ethical committees (University of Cologne [20-1594], Aerztekammer Nordrhein [2021239]), and registered at the German Clinical Trials Register (DRKS00030509). All participants provided signed informed consent before their inclusion.
Á priori sample size calculation was based on QST measurements of 9 lipedema patients performed during the clinical routine for diagnostic purposes indicating a difference of z-scores larger than 1 between lipedema patients and controls. Using G*Power Version 3.1.9.6 for windows, we estimated a sample size of 17 plus 3 potential dropouts (effect size d=1, σ=1, α=0.05, and a power of 80%).
Patients were recruited from the CG-Lympha clinic for surgical lymphology (inclusion criteria: female, 18–40 years, body mass index (BMI) below 30 kg/m2; exclusion criteria: diseases affecting the sensory system, use of topical analgesics, diagnosis of independent pain etiologies). Lipedema was diagnosed by a trained physician based on symmetric volume increase of the legs, unresponsiveness to dietary measures, caliper jump at the ankle and/or wrist, unaffected hands and feet, and absence of signs of lymphedema. Healthy controls were addressed through flyer and email within the University Hospital Cologne and the University of Cologne.
2.2. Quantitative sensory testingQuantitative sensory testing was performed according to the protocol of the German Research Network on Neuropathic Pain (DFNS)32,37,40,41 by DFNS-trained scientists. Seven different tests were conducted to assess 13 different parameters in a standardized manner using the official DFNS test instructions and recommended testing devices (Thermal Sensory Analyser II (TSA-II; 9 cm2 thermode contact area), AlgoMed digital algometer, Medoc Main Station Version 6.4.0.22 (Medoc Ltd, Ramat Yishay, Israel); standardized von Frey hairs (Optihair2-Set, MRC Systems GmbH, Heidelberg, Germany); Pin-Prick stimulators (MRC Systems GmbH); and Rydel-Seiffert 64 Hz tuning fork (AESCULAP OF 33, AESCULAP Surgical Instruments, B. Braun, Melsungen, Germany). Individuals were measured at the lateral thigh, which is experienced as painful in lipedema patients and the dorsum of the hand as an intraindividual unaffected control area. Vibration detection thresholds (VDT) were assessed at the patella and the processus styloideus ulnae, respectively, and pressure pain thresholds (PPT) at the quadriceps femoris muscle and the thenar eminence, respectively.
Thresholds and age-, gender-, and area-normalized z-scores were calculated using Microsoft Excel 2010 for windows using the respective DFNS-reference values.
2.3. Assessment of pain intensities, psychometry, and medical historyPain psychometry was determined by the German Pain Questionnaire (DSF) of the German Pain Association,11,33 which combines several validated scores such as “The German depression-anxiety-and-stress scale (DASS),”35 the habitual well-being (FW7), and general health (Veterans RAND 12; VR-12) scores.25 In addition, it contains a comprehensive section of pain descriptions, such as rating of perceived pain intensities (numerical rating scale [NRS], 0 = no pain, 10 = worst pain imaginable) under resting or stress conditions, location, pain courses, duration, pain description list (Schmerzbeschreibungsliste [SBL]),27 and grades of severity according to von Korff,48 among others.
2.4. StatisticsStatistics were tested using GraphPad Prism 6 for windows. Statistical significance was assumed for α<0.05. Biometrical and psychometric data with continuous variables were compared using independent t-tests. Ordinal data were compared using the Mann–Whitney U test. Categorical data were tested through contingency tables by χ2. Z-scores of QST measurements were tested with 2-way repeated-measures design analysis of variances (ANOVA), followed by Sidak post hoc tests to correct for multiple comparisons. Quantitative sensory testing data of one patient were excluded from statistical analysis due to thermode failure but kept in the graphical representations because thermal thresholds did not seem to be affected in lipedema patients.
Receiver operating characteristic curves6 were calculated for PPT, VDT, and PPT-VDT measurements to gauge their potential diagnostic value. To estimate the certainty of our results under the premise of the sample size, we performed Bayesian inference analysis31 using the Turing package (v0.24.1) and the AdvancedMH package (v0.7.4) for Julia 1.8.5. To evaluate the posterior densities, a Hamiltonian Monte Carlo (HMC) algorithm with No-U-Turn Sampler (NUTS) were used to obtain 106 samples for each posterior density except for PHS and DMA. Because of the singular data, numeric differentiation fails, and hence, a standard Metropolis-Hastings algorithm was used. Modelling assumptions are described in the respective results sections.
All data are available upon request from the corresponding author.
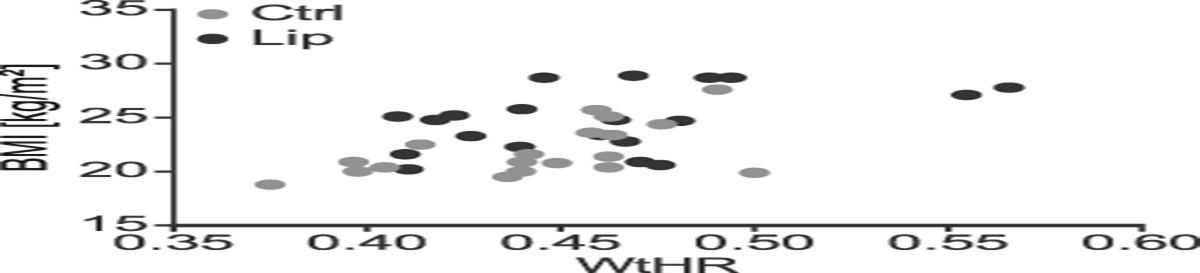
3. Results 3.1. Study population consisted of non-obese age-matched and waist-to-height ratio–matched women with only minor comorbiditiesWe recruited 40 women, 20 per group. The study was conducted in German with all participants speaking German on native speaker level (cohort characteristics, see Table 1). There was no statistically significant difference of age (ctrl: 27.15 ± 4.2 years, lipedema: 27.35 ± 4.4 years; P = n.s), height (ctrl: 169.3 ± 6.0 cm, lipedema: 165.7 ± 7.3 cm; P = n.s.), weight (ctrl: 63.4 ± 7.7 kg, lipedema: 68.3 ± 11.1 kg; P = n.s.), waist (75.2 ± 5.1 cm, lipedema: 76.3 ± 7.8 cm; P = n.s), and waist to height ratio (WtHR, waist [cm]/height[cm], ctrl: 0.44 ± 0.03, lipedema: 0.46 ± 0.04; P = n.s.). Lipedema patients showed a slight but statistically significant higher body mass index (BMI, weight [kg]/(height [m])2) compared with the controls (ctrl: 22.1 ± 2.4 kg/m2, lipedema: 24.8 ± 2.9 kg/m2, P < 0.05). Body mass indexes and WtHR of both groups were within the normal or slightly overweight range28 (Fig. 1).
Table 1 - Biometrical data. Ctrl Lipedema P Mean ± SD range Mean ± SD range Age [y] 27.15 ± 4.2 20–37 27.35 ± 4.4 23–40 n.s. Height [cm] 169.3 ± 6.0 157–179 165.7 ± 7.3 152–175 n.s. Weight [kg] 63.4 ± 7.7 48–76 68.3 ± 11.1 54–88 n.s. Waist [cm] 75.2 ± 5.1 60–80 76.3 ± 7.8 66–99 n.s. WtHR 0.44 ± 0.03 0.38–0.5 0.46 ± 0.04 0.41–0.57 n.s. BMI [kg/cm2] 22.1 ± 2.4 18.8–27.6 24.8 ± 2.9 20.2–28.9 <0.05BMI, body mass index; WtHR, waist to height ratio.
 Figure 1.:
Figure 1.: Distribution of body mass index (BMI) and waist-to-height ratio (WtHR) of our study population. Lipedema (Lip) patients showed a slight but statistically significant higher BMI compared with the controls. WtHR of both groups were not significantly different. BMIs and WtHR of both groups were within the normal or slightly overweight range.
Psychometric parameters and comorbidities were assessed using the DSF questionnaire. Fourteen lipedema patients and all controls provided full information.
All lipedema patients were diagnosed as stage I or II39 at least 6 months before recruitment (11.2 ± 6.6 years, range 0.5–27 years). All associated the manifestation of the disease with phases of hormonal changes, such as puberty. Fourteen reported a familial history of lipedema. All lipedema patients reported perceived chronic pain in the affected legs, and in 85.7% of patients, the pain was present for 1 year or longer. All reported only minor comorbidities (Table 2).
Comorbidities Ctrl (n) Lipedema (n) Mental/emotional strain 2 2 Hypothyreosis 3 2 Asthma 1 0 Migraine 0 1 Chronic sinusitis 0 1 Reflux, gastritis 2 1 Focal nodular hyperplasia 1 0 Endometriosis 0 2 Orthopedical entities (scoliosis, backpain, ligament rupture) 1 3 Peripheral nerve injury (area out of interest) 1 0The DSF questionnaire includes the “Depression, Anxiety, Stress Scale (DASS).” All scores for both groups were in an asymptomatic range, ie, below threshold of clinical significance (dashed red lines) (Fig. 2A). Nevertheless, all scores were significantly higher in lipedema patients compared with controls with respect to depression (controls 2.4 ± 3.66 vs lipedema 5.57 ± 4.26, t(32) = 2.33, P < 0.05), anxiety (controls 1 ± 1,3 vs lipedema 2.86 ± 3.03, t(32) = 2.45, P < 0.05), and stress (controls 3.1 ± 2.47 vs lipedema 7.29 ± 4.34, t(32) = 3.58, P < 0.01).
 Figure 2.:
Figure 2.: Psychometry of the participants as measured by the DSF. Dashed lines indicate cutoff values separating scores considered as normal or abnormal, respectively. (A) All scores of the depression–anxiety–stress scale (DASS) remained below the cutoff values and thus are considered as normal. (B) Results for the general health condition (veterans RAND-12 [VR12]) questionnaire with respect to the “physical compartment summary (PCS)” and “mental compartment summary (MCS).” Scores above dashed lines are considered as normal values. We found normal scores for both groups in the PCS; MCS scores slightly below the threshold value in lipedema (Lip) patients indicate the presence of minor mental burden. (C) Results for the habitual well-being (FW7 questionnaire) with higher scores indicating more well-being. We found a reduced score in lipedema patients; however, still in the mid range of the scale, indicating normal habitual well-being values for patients with chronic pain (all values are displayed as mean + standard deviation. Ctrl n = 20, lipedema n = 14). DSF, German pain questionnaire.
The DSF questionnaire includes the VR12 to assess the general health condition. The score is subdivided into a “physical compartment summary (PCS)” and a “mental compartment summary (MCS).” PCS-Scores of both groups were asymptomatic (values above dashed red line, Fig. 2B). Although nonpathological, the lipedema group showed reduced scores (43.78 ± 8.69) compared with controls (54.25 ± 7.69), t(30) = 3.59, P < 0.01. For MCS, the lipedema group showed slightly symptomatic values being below the cutoff value of 43. Nevertheless, we did not find a significant difference between the groups (Ctrl: 48.38 ± 14.56, lipedema: 40.99 ± 15.46), t(30) = 1.38, P > 0.05).
Furthermore, the DSF questionnaire assesses the habitual well-being using FW7 (Fig. 2C). Higher scores indicate higher well-being. Without a clear cutoff value, scores from the midrange and up can be considered as normal. The lipedema group scored midrange (17.64 ± 7.84) and controls higher-range (29.94 ± 5.81), t(30) = 5.1, P < 0.0001). Both scores indicate normal habitual well-being in both cohorts.
3.3. Lipedema patients report severe persistent pain with circadian fluctuations described with somatic termsAll participants rated their pain intensity on a numerical rating scale (NRS) during resting and during stress such as mild exercise (Fig. 3A). Control participants did not report noticeable pain with the exception of 2 participants with very mild stress-induced pain perceptions due to occasional nonchronic posture-induced back pain. By contrast, lipedema patients reported pronounced pain at resting conditions (control median 0, lipedema median 7, U = 0, P < 0.0001) and increased stress-induced pain intensities (control median 0, lipedema median 8), U = 3.5, P < 0.0001.
 Figure 3.: Characterization of lipedema (Lip) pain as measured by the DSF. (A) Pain intensity ratings on numerical rating scale (NRS; 0 = no pain, 10 = worst imaginable pain) under resting conditions and stress induced, eg, during mild exercise. Lipedema pain ratings were significantly increased compared with the control group, where pain was virtually absent (Ctrl n = 20; lipedema n = 20; independent t test; PRef. 10) as described by lipedema patients with circadian fluctuations. (C) Results for the German version of the Pain Description List (SBL), subdivided into an affective (SBL-A) and somatic (SBL-S) part. Values above the dashed line indicate a pathologic SBL-A of increased affective pain perception. This was not the case in our population of lipedema patients (n = 14). Furthermore, the higher SBL-S score indicated a rather somatic nature of lipedema pain. (D) Grades of severity according to von Korff (0: no pain; 1: low pain intensity; low disability; 2: high pain intensity; low disability; 3: high pain-related disability; moderately limiting; 4: high pain-related disability; severely limiting) (Ctrl n = 20; lipedema n = 14; χ2 test; P
Figure 3.: Characterization of lipedema (Lip) pain as measured by the DSF. (A) Pain intensity ratings on numerical rating scale (NRS; 0 = no pain, 10 = worst imaginable pain) under resting conditions and stress induced, eg, during mild exercise. Lipedema pain ratings were significantly increased compared with the control group, where pain was virtually absent (Ctrl n = 20; lipedema n = 20; independent t test; PRef. 10) as described by lipedema patients with circadian fluctuations. (C) Results for the German version of the Pain Description List (SBL), subdivided into an affective (SBL-A) and somatic (SBL-S) part. Values above the dashed line indicate a pathologic SBL-A of increased affective pain perception. This was not the case in our population of lipedema patients (n = 14). Furthermore, the higher SBL-S score indicated a rather somatic nature of lipedema pain. (D) Grades of severity according to von Korff (0: no pain; 1: low pain intensity; low disability; 2: high pain intensity; low disability; 3: high pain-related disability; moderately limiting; 4: high pain-related disability; severely limiting) (Ctrl n = 20; lipedema n = 14; χ2 test; PLipedema patients reported a distinct circadian pattern with increasing pain in the early afternoon and culminating in the evening (Fig. 3B). Pain was experienced with varying degrees of oscillation. All but 4 reported continuous pain.
The emotional or affective (SBL-A) and somatic (SBL-S) pain, respectively, was captured using the pain description list (SBL)27 (Fig. 3C). Schmerzbeschreibungsliste-affective values remained considerably below threshold values. Schmerzbeschreibungsliste-somatic presented higher values. This indicated a subordinated role for the affective emotional component, while pointing to a rather somatic nature of lipedema pain.
Von Korff grading captures the severity of pain as a function of intensity and disability48 (Fig. 3D). Grades are defined as 0: no pain, 1: low pain intensity and low disability, 2: high pain intensity with low disability, 3: high pain-related disability that is moderately limiting, and grade 4: high pain-related disability that is severely limiting. Corroborating others, lipedema pain appears mostly as moderately in few cases as severely limiting.
3.4. Normal sensitivity thresholds for all lipedema-patients and controls measured at the dorsum of the handBeyond questionnaire-based psychometry, we performed QST according to the protocol of the DFNS32,37,40,41 to objectify evoked response thresholds of sensory inputs.
Sensory thresholds were assessed at the notaffected dorsum of the hand. Comparison with DFNS control data showed z-scores for all parameters to remain in the normal range within the 95% confidence interval (CI) (−1.96 to 1.96). A repeated-measures ANOVA followed by Sidak post hoc test showed no significant difference between both groups in any of the parameters assessed at the dorsum of the hand (Fig. 3A, F(1, 418) = 0.0002, P > 0.05). This indicates experimenter-proficiency using the QST methodology and absence of generalized pain (Fig. 4A).
 Figure 4.:
Figure 4.: Mean QST sensory profiles. (A) Mean QST sensory profiles of control and lipedema (Lip) participants measured at the dorsum of the hand. Values between −1.96 and 1.96 are considered normal. (B) Mean QST sensory profiles of control and lipedema participants measured at the lateral thigh. We found significantly increased PPT and decreased VDT values, respectively, in lipedema patients. (C) Display of single participant data of controls and lipedema patients measured at the lateral thigh for PPT and VDT (Ctrl n = 20, lipedema n = 20, except thermal thresholds at the lateral thigh: n = 19 (see results section for explanation)), 2-way repeated-measures ANOVA, ****P < 0.0001). CDT, cold detection threshold; CPT, cold pain threshold; DMA, dynamical mechanical allodynia; HPT, heat pain threshold; MDT, mechanical detection threshold; MPS, mechanical pain sensitivity; MPT, mechanical pain threshold; PHS, paradoxical heat sensations; PPT, pressure pain threshold; TSL, thermal sensory limen; VDT, vibration detection threshold; WDT, warmth detection threshold; WUR, windup phenomenon.
3.5. Selectively decreased threshold for pressure pain and increased threshold for vibration detection at the lateral thigh of lipedema patientsNext, measurements were conducted at the lateral thigh, which is reported as painful by patients (Fig. 4B). Z-scores of the control group remained within the normal 95% CI range, with exception of a slightly increased value for the pressure pain threshold if compared with DFNS controls measured at the dorsum of the foot. Also lipedema patients showed normal QST measurements for most test stimuli with 2 exceptions: (1) values for the PPT were strongly increased (4.51 ± 1.26, see Fig. 4C), indicating pain hyperresponsiveness; and (2) values for the VDT were strongly decreased (−3.67 ± −1.41, Fig. 4C), suggesting reduced sensitivity to vibration. Repeated-measures ANOVA followed by Sidak multiple comparison post hoc test revealed a significant difference between lipedema patients and controls (F(37, 370) = 2.485, P < 0.0001) for PPT (P < 0.0001, 95% CI = −3.442, −1.371) and VDT ((P < 0.0001, 95% CI = 1.203, 3.274).
3.6. Pressure pain threshold and vibration detection threshold shows high sensitivity and selectivity to identify participants as lipedema patientsNext, we investigated whether only considering PPT and VDT identifies lipedema patients in the set of all 40 measured women. We performed a ROC analysis for sensitivity and specificity of such assignments. First, we tested whether using either the values for PPT or alternatively for VDT would correctly identify participants as either lipedema patient or control. Each parameter alone showed promising diagnostic ability assigning in the best case 90.75% (PPT) and 86.38% (VDT), respectively, of the measured women correctly as lipedema or control (PPT: AUC = 0.9075, P < 0.0001; VDT: AUC = 0.8638, P < 0.0001, Fig. 5A).
 Figure 5.:
Figure 5.: ROC analyses for diagnostic ability investigation of assessed QST z-scores. (A) ROC analyses of PPT and VDT measured at the lateral thigh in control participants and lipedema (Lip) patients. Each parameter alone showed promising diagnostic ability to distinguish both groups of our study population. (B) ROC analysis of the combined values of both parameters on single patient level. Assessment of both parameters increased the diagnostic ability. (C) Intraindividual control measurements are considered by value subtraction of hand measurements from measurements of the thigh for each parameter. Again, both parameters showed promising diagnostic ability. (D) Subtraction of both values calculated in (C) showed the highest diagnostic potential in terms of sensitivity and specificity. PPT, pressure pain threshold; QST, quantitative sensory testing; ROC, receiver operating characteristic; VDT, vibration detection threshold.
3.7. Combination of pressure pain threshold and vibration detection threshold values shows higher sensitivity and selectivity to assign participants as lipedema patientsNext, we asked whether combining PPT and VDT potentially allows a better identification of single individuals as either lipedema patient or control. We subtracted the values of the z-scores of PPT and VDT measured at the lateral thigh and performed another ROC analysis. Combining both parameters increased the diagnostic ability to 93.00% correct assignment as lipedema or control (AUC: 0.93, P < 0.0001, Fig. 5B).
Because we measured all QST parameters at the hand as an intra-individual control site, we tested whether a combination of the QST measurements taken at the thigh with the ones taken at the hand allows an even more sensitive and selective group assignment. For this, we subtracted the z-score hand values from the respective thigh values of the same individual for PPT and separately for VDT, respectively (∆(parameter) = z-score(thigh) – z-score(hand), d-score). This did not further increase the sensitivity and selectivity to assign measured women as lipedema or control (Fig. 5C, PPT: AUC 0.888, P < 0.0001; VDT: 0.900, P < 0.0001).
3.8. Integration of pressure pain threshold of thigh, pressure pain threshold of hand, vibration detection threshold of thigh, and vibration detection threshold of hand into one PVTH score shows best sensitivity and selectivity to identify participants as lipedema-patients or controlsFinally, we combined all 4 measurements into a score (PPT, VDT, thigh, hand–score) and tested for sensitivity and selectivity of such a “PVTH-score” to identify the measured women as lipedema or control. We defined the score as PVTH score = (z-score(PPT-thigh) – z-score(PPT-hand)) – (z-score(VDT-thigh) – z-score(VDT-hand)). Of all ROC analyses this, resulted in best sensitivity and best specificity, identifying 95.8% of the measured individuals correctly as lipedema patient or control (AUC = 0.958, P < 0.0001, Fig. 5D, see also Table 3 for sensitivity-specificity values).
Table 3 - Exemplary sensitivity–specificity threshold value pairs. Threshold value Sensitivity [%] 95% CI Specificity [%] 95% CI Likelihood ratio >1734 95 75.13%–99.87% 40 19.12%–63.95% 1.583 >2013 95 75.13%–99.87% 45 23.06%–68.47% 1.727 >3302 95 75.13%–99.87% 85 62.11%–96.79% 6.333 >3340 95 75.13%–99.87% 90 68.30%–98.77% 9.500 >4378 80 56.34%–94.27% 95 75.13%–99.87% 16.000 >4551 80 56.34%–94.27% 100 83.16%–100.0%Combinatory measurements of PPT and VDT at the hand dorsum and the lateral thigh.
PPT, pressure pain threshold; VDT, vibration detection threshold.
This suggests that one may reduce the full QST protocol of 7 measurements at 2 different sites to just these PPT and VDT measurements, thereby reducing the time from approximately 1 to 1.5 hours for a full QST to approximately 10 minutes for such a 2 measurement protocol while maintaining a high sensitivity and selectivity for the identification of lipedema patients on single patient basis.
3.9. Bayesian inference corroborates promising diagnostic ability of 4 combined measurements (pressure pain threshold of hand, pressure pain threshold of thigh, vibration detection threshold of hand, and vibration detection threshold of thigh) irrespective the cohort size of the study at handEspecially for small sample sizes, classical statistics does not provide reliable estimates about generalization potential of results. By contrast, Bayesian statistics can estimate how well a proposed diagnostic test would perform in the medical practice based on the limited study group size.
For the Bayesian analysis, we considered the d-scores from 19 lipedema patients and 20 nonlipedema participants (Fig. 6A). How the d-scores for the whole population are distributed is not known. For the general population estimate, we assumed a location scale t-distribution t(μ,σ,ν) for the d-scores of the general population. The parameters μ, σ, and ν had to be inferred from our data set . For this, the following posterior probability distribution is used:p(μ,σ,ν∣)∼pdfNormal(0,100)(μ)⋅pdfExp(10000)(σ)⋅pdfExp(10000)(ν)⋅∏i=1npdft(μ,σ,ν)(di) .
 Figure 6.: Bayesian inference about the general population from small sample size. (A) Difference of z-scores from lateral thigh and hand, named “d-scores,” for the different measurements of control and lipedema (Lip) women. (B–D) Inferred parameters for both groups for all QST aspects. The combined PPT-VDT
Figure 6.: Bayesian inference about the general population from small sample size. (A) Difference of z-scores from lateral thigh and hand, named “d-scores,” for the different measurements of control and lipedema (Lip) women. (B–D) Inferred parameters for both groups for all QST aspects. The combined PPT-VDT d
-scores difference between lipedema and nonlipedema is more pronounced than PPT or VDT alone (μ
:mean of a normal distribution,σ
:standard deviation andν
:outlier tendency). (E) ROC curve for PPT-VDT calculated from the inferred population distributions. Color shades display range of possible ROC curves for different highest density interval (hdi) levels. The darker the shade, the lower the corresponding hdi level. The combinedd
-score PPT-VDT promises to be a valid diagnostic tool with reasonable sensitivity and specificity for the detection of lipedema. PPT, pressure pain threshold; QST, quantitative sensory testing; ROC, receiver operating characteristic; VDT, vibration detection threshold.(See supplement for detailed explanation and derivation). In short, on the basis of the limited data collected, the posterior distribution allows calculation of the probability that a parameter is the true but unknown population parameter. Figures 6B–D shows these probability distributions for location μ, scale σ, and outlier tendency ν. Table 4 lists the 99% highest density intervals, ie, the smallest intervals in which the true parameters lie with 99% probability, given our data. In addition, the posterior probability allows to plot different credibility regions for ROC curves that are to be expected if our study was repeated with other and potentially more participants (Fig. 6E).
Table 4 - 99% highest density intervals for the quantitative sensory testing parameters of interest. Parameter VDT PPT PPT − VDTμ
nonlipedema −1.71, −0.31 0.21, 1.75 1.09, 2.90μ
lipedema −3.96, −2.16 2.40, 4.45 5.02, 7.91σ
nonlipedema 0.72, 1.76 0.80, 1.95 0.93, 2.28σ
lipedema 0.88, 2.22 1.02, 2.56 1.43, 3.60ν
nonlipedema 1.21, 46213.70 1.21, 46089.20 1.83, 45991.70ν
lip 0.96, 46113.61 0.97, 45980.46 0.97, 46159.00PPT, pressure pain threshold; VDT, vibration detection threshold.
These analyses corroborate our results: The PVTH score appears as a promising diagnostic test also for the general population. The credibility regions of the ROC analysis suggest that our sample ROC analysis (Fig. 5) can be in principle generalized to the general population. The 99% credibility levels contain as best case a sensitivity above 95% and as worst case a sensitivity of at least 50%, both for negligible false-positive probabilities (100% - specificity). The most probable sensitivity (0.1% hdi region) is approximately 75%.
4. DiscussionPain is a hallmark reported by most lipedema patients. We aimed to objectify lipedema pain for its physiological sensory vs psychosocial content. This may guide hypothesis building about the etiology and treatment of lipedema pain and may help developing novel diagnostic tools.
Our sample size estimation resulted in a surprise. Anecdotal QST data of clinical routine patients indicated a pronounced effect size detectable with a cohort of mere 17 patients. Indeed, our cohort of 20 non-obese lipedema patients and 20 matched controls corroborated the existence of a clear twofold increased PPT-z-score for lipedema patients over our matched controls. The difference to the over 1200 QST-DFNS database controls was even larger. Our study-groups are well matched by weight, height, waist, and WtHR, respectively.1,9,10,16,23,28,44,51 They represented the general population with comorbidities, such as orthopedic problems, hypothyreosis,5,53 occasional back pain, and migraine. Participants were only excluded if diagnosed as chronic pain patients but not with only anecdotal pain. We even kept 2 participants with endometriosis because their QST profiles did not systematically differ.
There is speculation about the psychological burden of lipedema patients.7,15 We do not have indications of clinically relevant psychometric abnormalities. All participants reported normal scores for depression, anxiety, and stress (DASS questionnaire) showed no significant influence of stress on pain experiences, normal PCS score (VR-12 questionnaire), and a normal general well-being, except for a marginally reduced VR-12 MCS score for lipedema patients. In contrast to reports by others,12 self-reported pain of stage I and II patients was severe. Corroborating others,21,43 verbal pain description pointed to a somatic rather than psychosomatic aversive experienced pain. Although psychologically asymptomatic, nevertheless, lipedema patients were considerably more burdened with lower quality of life with respect to social, mental, and physical functioning.42
留言 (0)