
記住我





Quach, Ha, Ouyang, Cb, Wang, Ab, Carrillo, Jb, Feranec, Jb, Ajewole, Cb, Lamvu, Gb
aUCF College of Medicine,bOrlando VA Healthcare System—Gynecology section
Introduction: The intrauterine device (IUD) is an efficacious, long-acting, reversible contraceptive method that can be used to treat dysmenorrhea and heavy menses. Studies have shown that women experience moderate levels of pain at the time of IUD insertion and that they may decline IUD insertion due to fears of pain. Previous investigations regarding the efficacy of oral analgesics for IUD insertion pain have conflicting results. We hypothesize that a multidose ibuprofen regimen given 24-hours before the insertion of IUD can provide pain relief.
Methods: This is a prospective, triple-blind, placebo-controlled study that assesses pain levels with a 10-point visual analog scale (VAS) during speculum insertion, tenaculum insertion, IUD insertion, and 24 hours after insertion. Pain methods used 24 hours after insertion were also assessed. We performed an interval analysis of 27 patients who have completed the trial, without breaking the randomization sequence as enrollment is still ongoing.
Results: There is a significant difference in IUD insertion pain scores between multidose ibuprofen group and a placebo group (Group A mean 6.8, SD 1.7, Group B mean 4.3, SD 2.9, P = 0.01). There was no difference in pain scores at any other time point. Despite a higher pain score at the time of insertion, more women in Group A than in Group B used no pain medications after insertion (P = 0.03).
Conclusions: There is a difference in pain scores at the time of IUD insertion; however, due to ongoing randomization, we do not know whether it is less in women who took ibuprofen or placebo.
Disclosure: Any of the authors act as a consultant, employee, or shareholder of an industry for: Yes. Dr. Lamvu serves as Chair of the Board for the International Pelvic Pain Society, research consultant for Abbvie, Chief Science Officer for SoLá Therapy, subject matter expert for Medical Learning Institute, and research advisor for SOLVD Health.
Elucidating the neural underpinnings of comorbid endometriosis and migraine: a pilot fMRI investigationSieberg, Ca, Szabo, Eb, Lunde, Cc, Kim, Ab, Missmer, Sd, Borsook, De, Holmes, Sa
aBoston Children's Hospital/Harvard Medical School,bBoston Children's Hospital,cUniversity of Oxford/Boston Children's Hospital,dMichigan State University,eHarvard Medical School
Introduction: Endometriosis and migraines are highly comorbid. Patients with endometriosis are twice as likely to experience migraines as those without; however, it is unclear as to why. Migraine may parallel disease phenotypes in endometriosis in that it is a visceral, intermittent, inflammatory pain, which can chronify. This study used MRI to investigate resting state functional connectivity (RSC) and structural data to compare patients with both conditions with those with endometriosis or migraine only.
Methods: Using the right anterior insula and left medial frontal cortex as seed regions, group differences in RSC between 14 patients with endometriosis and 11 patients with both conditions were compared. Group differences in cortical thickness were compared between the comorbid group and 14 patients with migraine only.
Results: Significantly increased functional connectivity in the left medial prefrontal cortex was observed in patients with both diseases in the left pallidum, part of the basal ganglia, compared with patients with endometriosis only (P < 0.05, FDR corrected for multiple comparisons). Decreased cortical thickness was detected in patients with both diseases in the left superior frontal gyrus compared with those with migraine only (P < 0.05, Monte Carlo corrected for multiple comparisons).
Conclusions: Patients with both diseases exhibited altered functional connectivity in the left medial prefrontal cortex and reduced cortical thickness in the left superior frontal gyrus, part of the dorsolateral prefrontal cortex, a key area for nociceptive modulation, when compared with patients with migraine only. This suggests alterations in cognitive inhibitory control processes, including descending pain modulation.
Disclosure: No.
Sexual pain in women with chronic pain and childhood sexual abuseFoxx, Aa, Whitmore, Ga, As-sanie, Sa, Till, Sa
aUniversity of Michigan
Introduction: A history of sexual abuse is associated with chronic pelvic pain. This study further investigates the pain experience with respect to sexual activity in adulthood for this unique population.
Methods: Retrospective cross-sectional study of new patients at a tertiary care hospital’s chronic pelvic pain clinic between 2019 and 2021. All patients completed validated self-report measures on their pain.
Results: Of 1112 patients, 22% (N = 241) reported childhood sexual abuse, whereas 45% (N = 500) reported no sexual, physical, or emotional trauma. There was no statistical difference in terms of age, racial demographics, marital status, or the rate of endometriosis diagnosis. Survivors reported similar “average pain” (5.4 (SD 1.8) vs 5.1 (SD 1.9); P = 0.016) and “worst pain” (7.0 (SD 1.9) vs 6.5 (SD 1.9); P = 0.007) within the last week, as compared those with no history of any type of abuse. However, specific activities were consistently more painful for survivors of sexual abuse, including urination (3.0 (SD 3.0) vs 2.4 (SD 2.9); P = 0.006), having a full bladder (4.6 (SD 3.0) vs 3.6 (SD 3.1); P < 0.001), bowel movements (5.1 (SD 3.1) vs 4.1 (SD 3.3); P < 0.001), deep intercourse (6.7 (SD 3.1) vs. 5.6 (SD 3.6); P < 0.001), and insertion during sex (5.2 (SD 3.6) vs 4.3 (SD 3.7); P = 0.004) and with tampon use (4.0 (SD 3.5) vs 3.0 (SD 3.2); P = 0.001). There was no statistical difference in the pain they reported during their menses. Survivors were more likely to avoid sex due to pain (OR = 2.2 [1.3, 3.6]) or interrupt sex due to pain (OR = 2.3 [1.5, 3.5]).
Conclusions: Despite survivors of childhood sexual abuse reporting similar overall pain to their peers, they have higher pain associated with sexual activity, as well as bladder and bowel function. There is a higher rate in this population of avoidance and interruption of sex due to pain.
Disclosure: No.
Lasers in the treatment of vulvodynia: a scoping reviewStarzec-Proserpio, Ma, Grigol Bardin, Mb, Morin, Mc
aCentre of Postgraduate Medical Education,bDepartment of Obstetrics and Gynecology, School of Medical Sciences, Campinas University,cSchool of Rehabilitation, Faculty of Medicine and Health Sciences, Université de Sherbrooke; Research Center, Centre Hospitalier Universitaire de Sherbrooke (CHUS)
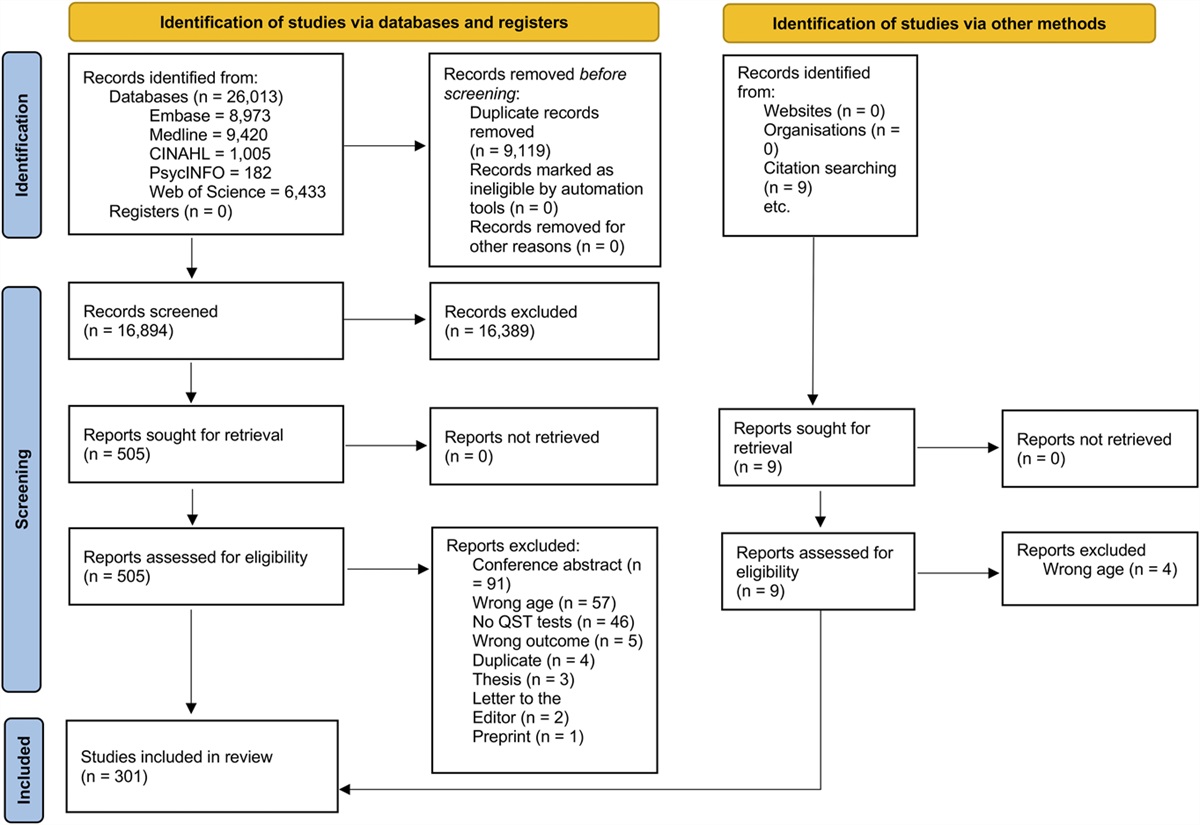
Introduction: Considering the warning statements issued by the Food and Drug Administration and leading societies, this review aimed to map the evidence on the effectiveness of lasers for vulvodynia.
Methods: A scoping review with a systematic search was conducted. Searches included terms related to vulvodynia and laser. The type of laser, effects on pain, function, participants’ perceived improvement, and adverse events were analyzed.
Results: Eight studies were included: 1 pilot randomized controlled trial, 5 before–after studies, 1 nonrandomized study, and 1 case report. The following laser applications were used: CO2 ablation, microablative CO2, microablative and nonablative photothermal treatment with Erbium:YAG, high-intensity laser therapy, and low-level laser therapy. Of the 6 studies including pain outcomes, 3 showed statistically significant improvements, and 3 reported a reduction in pain from subjectively interpreted data. The 2 studies investigating sexual function also reported an improvement (based on subjective interpretation). Of the 2 studies with a comparison group, neither one was powered to detect between-group differences. As for the patients’ perceived improvement, 57 to 78% of participants reported a significant or moderate improvement, with one study showing greater statistically significant improvement in the low-level laser therapy group compared with sham laser. The adverse events varied depending on the type of laser.
Conclusions: Although the findings obtained are promising, they should be interpreted with caution given the lack of robust and sufficiently powered studies. Further research is needed to assess the efficacy of different types of lasers for vulvodynia prior implementation into clinical practice.
Disclosure: No.
Does pudendal nerve block improve perioperative pain following onabotulinumtoxinA injection for myofascial pelvic pain?Coombs, Pa, Lewis, Gb, Chen, Ab, Carrubba, Ab
aHCA Healthcare/USF Morsani College of Medicine GME,bMayo Clinic Florida
Introduction: OnabotulinumtoxinA injections are useful for the treatment of myofascial pelvic pain. Concurrent pudendal nerve block (PNB) has been suggested to decrease postoperative pain, as OnabotulinumtoxinA does not take immediate effect. The efficacy of PNB for this purpose has not been well elucidated. We aim to determine whether PNB improves pain in the perioperative period following pelvic floor OnabotulinumtoxinA injections.
Methods: A subgroup analysis was performed from a retrospective cohort study including 202 patients encompassing 416 OnabotulinumtoxinA injections at a single academic institution. Post Anesthesia Care Unit (PACU) visual analog scale (VAS) pain score and oral morphine equivalents (OMEs) data between 2018 and 2022 were reviewed.
Results: A total of 64 patients met inclusion criteria, with 96 OnabotulinumtoxinA injection events. Thirty-three OnabotulinumtoxinA injections were done with concurrent PNB, while 63 injections were performed without PNB. Demographics of patients were similar in both groups. Mean VAS on arrival to PACU was 1.6 for OnabotulinumtoxinA alone and 2.2 for OnabotulinumtoxinA/PNB (P = 0.195). Mean VAS upon discharge from PACU was 1.7 for OnabotulinumtoxinA alone and 1.9 for OnabotulinumtoxinA /PNB (P = 0.291). Mean time (minutes) in PACU was 100.5 for OnabotulinumtoxinA alone and 101.6 for OnabotulinumtoxinA/PNB (P = 0.463). Mean OMEs given in PACU were 12.5 for OnabotulinumtoxinA alone and 14.9 for OnabotulinumtoxinA/PNB (P = 0.207).
Conclusions: This study suggests that pudendal nerve block at the time of pelvic floor OnabotulinumtoxinA injection may not have additional benefit of decreasing postoperative pain. Further larger studies are needed to determine the efficacy of pudendal nerve block at the time of pelvic floor OnabotulinumtoxinA injections.
Disclosure: No.
Heart rate variability and autonomic function of adolescents with chronic abdominal painTham, SWa, Ngai, Jb, Palermo, Ta
aUniversity of Washington School of Medicine,bSeattle Children's Research Institute
Introduction: Autonomic dysfunction has been increasingly reported in adults with chronic abdominal and pelvic pain. This is demonstrated by low heart rate variability (HRV), thought to be related to poorer pain modulation. Given the limited pediatric data, we compared subjective and objective autonomic function between adolescents with chronic abdominal pain (CAP) and pain-free adolescents and tested for group differences under stress.
Methods: This prospective study of 60 adolescents (females = 68.3%, M = 6.3 years) included 33 adolescents with CAP from the institution’s gastroenterology and pain clinics, and 27 pain-free adolescents from the community (October 2019 to April 2022). Adolescents reported on abdominal pain and autonomic function (COMPASS31) and underwent electrocardiogram monitoring for HRV parameters (RMSSD: root mean squared of successive differences, LF: proportion of low frequency) at rest and during stress induction.
Results: The groups were similar on age, race, and ethnicity, with more females in the group with CAP. Adolescents with CAP experienced moderate pain intensity (M = 5, SD = 2). Adolescents with CAP had a 22.3-point higher COMPASS31 scores compared with pain-free adolescents of the same age and sex (P < 0.001), whereas RMSSD and LF did not differ. On linear mixed models, adolescents with CAP had 1244-point increase in LF during stress compared with pain-free adolescents (P = 0.006); findings were not statistically significant for RMSSD.
Conclusions: Adolescents with CAP had greater self-reported autonomic dysfunction compared with pain-free adolescents but were similar on HRV. Having CAP was associated with changes in LF during stress but not RMSSD. Findings signal autonomic dysregulation in adolescents with CAP and need replication in larger samples.
Disclosure: No.
Is there a correlation between idiopathic scoliosis and chronic pelvic pain in females?Aklar, Aa, Mekik, Bb, Yeral, Ab, Aslan, Db, Attar, Rb, Attar, Eb
aFenerbahçe University,bYeditepe University
Introduction: Pelvic girdle symptoms associated with scoliosis can be seen rarely. Individuals with scoliosis are more likely to have adaptations in the surrounding muscles and fascia structures. It is possible that scoliosis contributes to pelvic pain by influencing pelvic joint alignment, tone of pelvic muscles, and relationship of relevant nerves to surrounding tissue. The current study aimed to investigate the relationship between idiopathic scoliosis and chronic pelvic pain among women.
Methods: A total of 52 women, with a mean age of 33.36 ± 13.69 years, were included in this study. Each participant filled out a structured questionnaire including sociodemographic characteristics and general health information. In addition to the sociodemographic characteristics of the individuals, their physical activity habits and the pelvic pain experience except during the menstrual period were questioned. The SRS-22 (Scoliosis Research Society-22) and Walter Reed Visual Scale were used to evaluate scoliosis. Also, VAS (visual analog scale) and PPIQ (Pelvic Pain Impact Questionnaire) questionnaires were used to assess the level of pelvic pain.
Results: The results of the study revealed a significant positive correlation between SRS-22, Walter Reed Visual Scale, PPIQ, and VAS levels of chronic pelvic pain (P < 0.05).
Conclusions: In conclusion, women with idiopathic scoliosis are more likely to have chronic pelvic pain. Therefore, women with idiopathic scoliosis may be also assessed in terms of pelvic girdle pain in the early stage of scoliosis.
Disclosure: No.
Transvaginal PBMT photon fluency enhanced with tissue coolingPietrafitta, Ja, Hetz, Nb, Devine, Jc
aGlobaLASEReach, LLC,bGlobaLASEReach,cNone
Introduction: Chronic pelvic pain (CPP) affects 22 million women. Treatments are frequently ineffective and painful. Transcutaneously administered photobiomodulation therapy (PBMT) has been shown to reduce musculoskeletal pain, although >90% of the photons reflect off or are absorbed into the skin. The remaining photons travel only a few centimeters deep. The vaginal cavity becomes a valuable portal to deliver photonic energy to painful pelvic floor musculature. A recent observational study suggests CPP improvement with transvaginal PBMT. Treatment power output (PO) is limited by heat generation within the vaginal cavity causing pain.
Methods: This study used a new transvaginal PBMT device that prevents excess heating of tissues using thermoregulation. This is accomplished using temperature sensors (TTS) and a cooling system; 810 nm light irradiation was administered on live human abdominal and thenar skin sites. Increasing PO was tested while maintaining the irradiated skin’s surface temperature (SST) at specific temperatures using the cooling system. Photon fluency tests through the thenar tissue were performed using 810-nm continuous mode at 10 W/sec with and without cooling. Cooling was used to maintain the SST just below 41°C or with enhanced cooling to maintain the SST between 35°C and 36°C.
Results: When skin cooling maintained STT just below 41°C, increasing PO did not cause burns or pain. Higher photon fluency readings were detected through the thenar tissues during the 35°C to 36°C tests compared with tests just below 41°C.
Conclusions: Combining skin surface cooling with 810-nm irradiation allows for higher PO to be administered, resulting in increased photon fluency without overheating tissues.
Disclosure: Yes, this is sponsored by industry/sponsor: GlobaLASEReach, LLC. Clarification: Industry initiated, executed, and funded study. Any of the authors act as a consultant, employee, or shareholder of an industry for: GlobaLASEReach.
The association of endosalpingiosis with chronic pelvic painLewis, Ga, Ghaith, Sb, Craver, Ea, Li, Za, Wasson, Mc, Burnett, Td, Carrubba, Aa
aMayo Clinic Florida,bMayo Clinic Alix School of Medicine,cMayo Clinic Arizona,dMayo Clinic Rochester
Introduction: Endosalpingiosis is a poorly understood condition of ectopic epithelium resembling the fallopian tubes. It is described as an incidental pathologic finding and similar to endometriosis. The primary objective is to determine whether endosalpingiosis (ES) has a similar association with chronic pelvic pain when compared with endometriosis (EM).
Methods: This is a retrospective case–control analysis of patients with a histologic diagnosis of endosalpingiosis or endometriosis at 3 affiliated academic hospitals between 2000 and 2020. All ES patients were included, and 1:1 matching was attempted to obtain a comparable EM cohort. Demographic and clinical data were obtained, and statistical analysis was performed.
Results: A total of 967 patients (515 ES and 452 EM) were included. ES patients were significantly older than EM patients (median age, 52 vs 48 years, P < 0.001), but other demographic variables were similar. Fewer ES patients had baseline chronic pelvic pain than EM patients (25.3% vs 47%, P < 0.001), and patients with ES were less likely to undergo surgery for the primary indication of pelvic pain (16.1% vs 35.4%, P < 0.001). Pelvic pain as the surgical indication remained lower in the ES group in multivariable analysis (OR = 0.49, P < 0.001). There were similar rates of persistent postoperative pain between ES and EM groups (10.1% vs 13.5%, P = 0.109).
Conclusions: Although endosalpingiosis can be associated with chronic pelvic pain, the incidence of pain is significantly lower than in patients who have endometriosis. These findings suggest that ES is a unique condition that differs from EM. Further research including long-term follow-up and patient-reported outcomes is imperative.
Disclosure: Any of the authors act as a consultant, employee, or shareholder of an industry for: Gynesonics (Dr. Carrubba is part of the Advisory Board). This position was not related to the current project.
“They do make you feel embarrassed or ashamed or like you're crazy”: patient–provider communication about vulvar painRowland, Ca, Cromeens, MGb, Ogbansiegbe, Jc, Mihas, Pd, Banhabbour, Re, Carey, Ef
aUNC School of Medicine,bIndiana University School of Nursing,cUniversity of North Carolina at Chapel Hill,dOdum Institute for Research in Social Science, University of North Carolina at Chapel Hill,eoint Department of Biomedical Engineering, University of North Carolina,fDepartment of Obstetrics and Gynecology, University of North Carolina
Introduction: Individuals suffering from vulvodynia can experience painful physical and psychosocial effects while navigating disconnected health services. The purpose of this study is to explore individuals’ experiences with vulvodynia and provider interactions.
Methods: This descriptive qualitative study used focus groups to interview heterosexual, adult (ages 18–51) women suffering from vulvodynia, vestibulodynia, or dyspareunia. Participants completed questionnaires and semistructured focus group discussions. We conducted 6 focus groups with 3 to 5 participants. Focus group discussions were audiorecorded, transcribed verbatim, and coded by 2 independent investigators who met to resolve differences and reach consensus. This study analyzed selected codes and subsets of codes related to feelings of frustration, isolation, and being misunderstood in provider interactions. The University of North Carolina Institutional Review Board approved this study.
Results: Twenty participants participated in the focus group discussions. The mean age for the participants was 33.3 years. Most women were educated with at least some college (93%), White (78.6%), married (75%), and had income greater than $100,000 (50%). Participants shared feelings of frustration surrounding interactions with providers, feeling dismissal, disbelief, isolation, and stigmatization, resulting in feelings of self-doubt. Patient–provider interactions left the participants dissatisfied with diagnostic experiences–feeling providers did not understand the condition and were commonly misdiagnosed.
Conclusions: Patients experiencing vulvar pain value interactions with providers that affirm their symptoms and experiences and provide them with autonomy in decision making for treatment. Provider education efforts may help to destigmatize the condition and improve the quality of care for patients experiencing vulvar pain.
Disclosure: Any of the authors act as a consultant, employee, or shareholder of an industry for: Annelleo.
Endometriosis-associated pain and adverse childhood events: is resiliency the missing puzzle piece?Lunde, Ca, Szabo, Eb, Kim, Ab, Holmes, Sc, Borsook, Dd, Sieberg, Cb
aBoston Childrens Hospital and University of Oxford,bBoston Childrens Hospital,cBoston Childnres Hospital,dMassachusetts General Hospital
Introduction: Endometriosis is one of the most common chronic gynecological diseases affecting 10 to 15% of women in their reproductive years and 70% of people with chronic pelvic pain. Approximately 62% of adults in the United States report at least one childhood trauma, which is associated with an increased risk of chronic pain and gynecological complications. Resilience is important to measure in addition to stress or trauma as the mechanisms associated with stress-related psychopathology are expected to differ significantly from those associated with resilience. This study aimed to describe the experience of childhood stress, resilience, and trauma in people with endometriosis-associated pain (EAP).
Methods: Participants with endometriosis (n = 37, mean age = 27.9 years) and pain-free controls (n = 40, mean age = 25.6 years) completed 2 questionnaires: Childhood Traumatic Events Scale (CTES) and the Connor-Davidson Resilience Scale (CD-RISC). T-tests were used to compare the groups.
Results: Although both groups endorsed an average of 2 childhood traumatic events, those with endometriosis reported a significantly higher burden score indicating a greater perceived impact, mean score of 10.2 (7.6) vs. 6.8 (5.2) (t(50) = −1.8, P = 0.03). There were no significant differences between the groups on resiliency scores; although both groups endorsed low/moderate overall resiliency scores, the mean score for controls was 21.8 (4.5) vs. EAP participants with 21.1 (5.4).
Conclusions: Further research with larger sample sizes and mixed methodologies is needed to further elucidate the relationship between EAP, trauma, and resiliency. However, these findings highlight the importance of trauma-informed care and positive psychology for those with EAP.
Disclosure: No.
Childhood pelvic pain in survivors of childhood sexual traumaFoxx, Aa, Whitmore, Ga, As-sanie, Sa, Till, Sa
aUniversity of Michigan
Introduction: A history of sexual abuse is associated with chronic pelvic pain.
Methods: Retrospective cross-sectional study of new patients at a tertiary care hospital’s chronic pelvic pain clinic between 2019 and 2021. All patients completed validated self-report measures of pain and pain outcomes.
Results: Of 1112 patients, 22% (N = 241) reported childhood sexual abuse, whereas 45% (N = 500) reported no sexual, physical, or emotional trauma. There was no statistical difference in age, racial demographics, marital status, or the rate of endometriosis diagnosis. Among survivors of sexual abuse, 52% (N = 128) had pain during their childhood. The majority (89%) of patients with childhood pain had persistent pain that never resolved. Another 7.8% of patients had childhood pain that lasted for more than a year before resolving as a child. Less than 4% had pain that resolved within a year of developing it during childhood. Survivors were more likely to have pain during their childhood (OR = 2.3[1.7, 3.1]) and were more likely to have their pain continue to persist into adulthood (OR = 2.3[1.7, 3.1]) as compared with women with chronic pelvic pain and no history of sexual abuse. Survivors of sexual abuse tended to develop pain at an earlier age than their peers (12.3 (SD 3.8) vs 13.3(SD 3.1); P = 0.018).
Conclusions: Pain starts at a younger age among survivors of childhood sexual trauma, and it is more likely to persist into adulthood (instead of resolve) as compared with women with no trauma history. This highlights the importance of treating childhood pain in survivors of sexual abuse because it is unlikely to spontaneously resolve.
Disclosure: No.
Dysmenorrhea catastrophizing and functional impairment in female pelvic painLi, Ra, Kreher, Db, Gubbels, Ac, Palermo, Td, Benjamin, Ae, Irvine, Ce, Hart, Ae, Jusko, Tb, Seplaki, Cb
aSeattle Children's Research Institute,bUniversity of Rochester School of Medicine & Dentistry,cCreighton University School of Medicine-Phoenix,dUniversity of Washington School of Medicine,eDepartment of Obstetrics and Gynecology
Introduction: Dysmenorrhea is suggested to increase the risk of chronic pain by enhancing central sensitization. However, little is known about whether emotional and cognitive responses induced by dysmenorrhea contribute to chronic pain-associated functional impairment. We examined the association between catastrophizing specific to dysmenorrhea and disability associated with both dysmenorrhea and chronic pelvic pain (CPP).
Methods: Women (N = 104) receiving care for CPP through a tertiary gynecological pain clinic between 2017 and 2020 were recruited. They completed the pain catastrophizing scale, the brief pain inventory–pain interference, and a newly developed questionnaire assessing dysmenorrhea symptoms and treatment preceding the development of CPP. Dysmenorrhea catastrophizing and dysmenorrhea interference measures were developed and tested for internal consistency and construct validity. Multiple linear regression models examined dysmenorrhea catastrophizing in association with dysmenorrhea interference and CPP interference.
Results: Dysmenorrhea catastrophizing and interference measures demonstrated excellent internal consistency (Cronbach alpha 0.93 and 0.92, respectively) and evidence of construct validity (correlated with dysmenorrhea severity and treatment, Ps < 0.01). Dysmenorrhea catastrophizing moderately correlated with pain catastrophizing (ρ = 0.30) and was associated with greater dysmenorrhea interference (P < 0.001) and CPP interference (P = 0.009) accounting for general pain catastrophizing and other confounders. Exploratory analysis identified dysmenorrhea intensity as the most important predictor of dysmenorrhea catastrophizing.
Conclusions: Among treatment-seeking women with CPP, dysmenorrhea-specific catastrophizing is associated with disability related to both previous dysmenorrhea and current CPP. Dysmenorrhea catastrophizing could be an important pathway to amplified pelvic pain–related functional impairment and thus constitute a target for early intervention.
Disclosure: No.
Experience with treatments as reported by persons with chronic pelvic pain in the general populationLewis, Ha, Manko, Kb, Ajewole, Cc, Lamvu, Gc
aUCF HCA GME Consortium of Greater Orlando,bUniversity of Central Florida College of Medicine,cOrlando Veterans Affairs
Introduction: Current guidelines for management of chronic pelvic pain (CPP) emphasize a multimodal approach including holistic treatments and pelvic physical therapy (PT). Treatment research focuses primarily on use of surgical and medical therapies among patients seen in specialty or tertiary care centers. Our objective was to determine what treatments are used by patients with CPP in the general population.
Methods: We conducted a cross-sectional survey of US persons ≥ 18 years old. To adequately represent women with CPP, within a 5% margin of error and 95% confidence level, the calculated sample size was 385 respondents. The survey contained questions about interactions with health care professionals and treatments used.
Results: Of 1221 respondents 63.8% (n = 780) reported abdominal/pelvic pain and a pain level ≥2 on a 0 to 10 scale; 122 had pain <6 months and 658 had pain ≥6 months (CPP). Of 658, 42.6% (n = 280) were diagnosed with a CPP condition by their PCP and 24.5% (n = 337) by a gynecologist. Of those with pain <6 months, 41.0% (n = 50) reported receiving no treatment vs. 51.2% (n = 337) of the group with CPP. Those with CPP were more likely to use opioids (12.5% vs. 3.3%, P = 0.002) and less likely to report having pelvic PT (16.4% vs. 32.8%, P = <0.00). Alternative treatments, including acupuncture, nutrition, and cognitive behavioral therapy, were used by 41.5% of CPP patients (n = 273).
Conclusions: Nearly half of patients with pelvic pain did not receive treatment. Alternative treatments and pelvic PT are largely unused, confirming a gap between current treatment guidelines and actual practice.
Disclosure: Dr. Lamvu is a consultant for SOLVD Health, Abbvie and Myovant.
The use of telemedicine in pelvic floor physical therapy: is it effective?Coad, Ba, Ramani, Sa, Michel, La, Morgan, Ja, Peled, Aa, Chudnoff, Sa, Andikyan, Va
aStamford Hospital
Introduction: The study objective was to examine whether there are differences in meeting treatment goals between pelvic floor physical therapy (PFPT) patients who participated in telehealth visits versus those who participated in traditional office visits at a community hospital.
Methods: Retrospective chart review was performed among women >18 years old who received PFPT at a 305-bed community teaching hospital from April 2019 to February 2021. Cohorts were defined as “Mostly Office Visits” (>50% office visits) and “Mostly Telehealth” (>/= 50% telehealth visits). Primary outcome measures included demographic data, number/type of visit for each patient, number of no-show/cancellation appointments, and number of patients discharged meeting PFPT goals. Statistical significance was defined as P < 0.05.
Results: Two hundred thirty-four subjects met criteria for the “Mostly Office Visit” cohort and 48 subjects met criteria for the “Mostly Telehealth” cohort. There were no significant differences observed in age (P = 0.919), BMI (P = 0.817), race/ethnicity (P = 0.170), or insurance type (P = 0.426) between the cohorts. There was no statistically significant difference in meeting PFPT goals between the “Mostly Office Visit” cohort (24.4%) and the “Mostly Telehealth” cohort (35.4%) (P = 0.113). There was no difference in the number of cancelled visits per patient (mean cancellations “Office visit” 1.98; “Telehealth” 1.63; P = 0.246) and the number of no-show visits per patient (mean no-show’s “Office visit” 0.23; “Telehealth” 0.31; P = 0.297) between the cohorts.
Conclusions: There was no statistically significant difference in meeting discharge goals regardless of whether a patient participated in majority telehealth visits versus traditional office visits. Therefore, we can conclude that provider-led telehealth visits may be equally efficacious at providing competent PFPT care.
Disclosure: No.
External myofascial mobilization improves both short and long-term outcomes in males with chronic pelvic painSharafudeen, Aa, Shenoy, Pa, Ismail, La, Al-mudahka, Na, Majzoub, Aa
aHamad Medical Corporation
Introduction: CPS (chronic pelvic pain syndrome) is a debilitating medical condition that affects males of all ages. The study objective was to assess the short-term and long-term benefits of an external myofascial mobilization (EMM) in the treatment of males with chronic pelvic pain syndrome (CPPS).
Methods: This study includes a retrospective chart review of patients who underwent EMM therapy for CPPS at the Pelvic Pain clinic between January 2019 and April 2021. As outcome measures, the National Institutes of Health-Chronic Prostatitis Symptom Index (NIH-CPSI) scale and the numerical rating scale (NRS) were used.
Results: A total of 29 patients completed the standard 4-session EMM therapy and the follow-up evaluation. Patients ranged in age from 24 to 61 years, with a mean of 38. The mean (SD) NIH-CPSI score was 28.41 (9.3) at the baseline and dropped to 7.14 (3.15) after the treatment. At 12 months, the NIH-CPSI score was 10.63 (4.95). The majority of the trial group's patients demonstrated a decline in NIH-CPSI score of >6 points post therapy, and this improvement was well sustained at follow-up at 12 months, showing a robust short-term and long-term response to EMM therapy. The NRS measurement also demonstrated a substantial improvement in pain (P 0.001).
Conclusions: An EMM strategy based on fascial connectivity resulted in considerable symptom improvement in all of the individuals investigated, with longer-lasting symptom alleviation. EMM is proven to be a successful therapy option for CPPS. To validate the conclusions presented here, more high-quality studies with control groups are required.
Disclosure: No.
Hypnotherapy use and acceptance in patients with chronic pelvic painFadadu, Pa, Fenske, Ba, Mara, Ka, Song, Ja, Gibbens, Ya, Philpot, La, Wang, XJa, Green, Ia
aMayo Clinic
Introduction: An increased number of patients with chronic pelvic pain (CPP) are seeking complementary and alternative medicine (CAM) therapies either as a primary treatment or as an adjunct to the traditional therapies of surgery or pharmaceuticals. Hypnotherapy can create a safe altered state of consciousness with the potential to alleviate pain. We aim to assess the current usage and acceptance of hypnotherapy among patients with CPP in a tertiary care practice.
Methods: We prospectively surveyed patients being evaluated for CPP from October 2021 to January 2022. The survey assessed prior experience and attitudes towards hypnosis and other CAM therapies. A favorability score was calculated based on responses for each CAM therapy.
Results: A total of 92 patients participated, 2.4% of which previously had tried hypnotherapy. Of patients who had not tried hypnotherapy, 65.3% were willing to try, with an average age of 35 years and 3 comorbid pain conditions. Those most willing to try hypnotherapy were patients who would also consider trialing massage therapy (P = 0.024), physical therapy (P = 0.003), psychotherapy (P < 0.001), dietary supplements (P = 0.037), and suppositories/enemas (P = 0.008). Hypnotherapy was more favorable to over-the-counter medications and suppositories/enemas and less favorable than heating/cooling pads, physical therapy, and wellness coaching. However, overall hypnotherapy had low favorability when compared with other CAM therapies.
Conclusions: Despite evidence of efficacy, hypnotherapy is not being used by patients with CPP and not viewed favorably. Future studies should focus on increasing provider knowledge of acceptable CAM therapies including hypnotherapy and patient selection as well as understanding limiting factors for efficacious but poorly used treatments.
Disclosure: No.
The impact of mind–body medicine on patient-reported outcomes in management of chronic pelvic painCarrubba, Aa, Lothman, Kb, Ball, Cb, Mongan, Ab, Perlman, Ab, Chen, Ab
aMayo Clinic Florida,bMayo Clinic
Introduction: Mindfulness therapy is beneficial for patients with chronic medical conditions, but there is limited data in pelvic pain. Our objectives are to determine whether mindfulness training improves quality of life outcomes in pelvic pain and to determine feasibility of implementation of this program.
Methods: This is a pilot feasibility trial for women with chronic pelvic pain at a single academic tertiary referral clinic. A convenience sample of 15 subjects was enrolled based on available funding. Subjects were scheduled for three 60-minute virtual mind–body sessions (1 individual and 2 group) with a mind–body counselor. Patient-Reported Outcomes Measurement Information System-Computer Adaptive Testing (PROMIS-CAT) scores were obtained at baseline, and they were repeated at 3 months and 6 months after enrollment. Minimal clinically important difference (MCID) cutoff values of 5 points were assigned to each category to assess for effectiveness of the intervention. Descriptive statistics were performed.
Results: Fifteen patients enrolled in the study, 14 attended the individual baseline mind–body counseling visit, 12 attended the first group visit, and 9 attended the second group visit. Among the 13 patients who completed the 3-month PROMIS-CAT scores, 7 had a significant MCID improvement in “sleep disturbance” T scores. At least a 5-point MCID improvement in the “fatigue,” “pain interference,” and “ability to participate in social roles” was observed in 6 patients each. There was a 40% dropout rate.
Conclusions: A formal mind–body counseling program can feasibly be implemented to support concurrent pelvic pain treatments. Our pilot trial demonstrated modest improvement in patient-reported quality of life.
Disclosure: Any of the authors act as a consultant, employee, or shareholder of an industry for: Gynesonics (Dr. Carrubba is part of the Advisory Board). This position was not related to the current project.
Acceptability of transvaginal photobiomodulation among women with chronic pelvic painAjewole, Ca, Manko, Kb, Lewis, Hc, Carrillo, Ja, Lamvu, Ga
aOrlando VA Medical Center,bUniversity of Central Florida School of Medicine,cOsceola Regional Medical Center Obstetrics and Gynecology Residency Progr
留言 (0)