
記住我

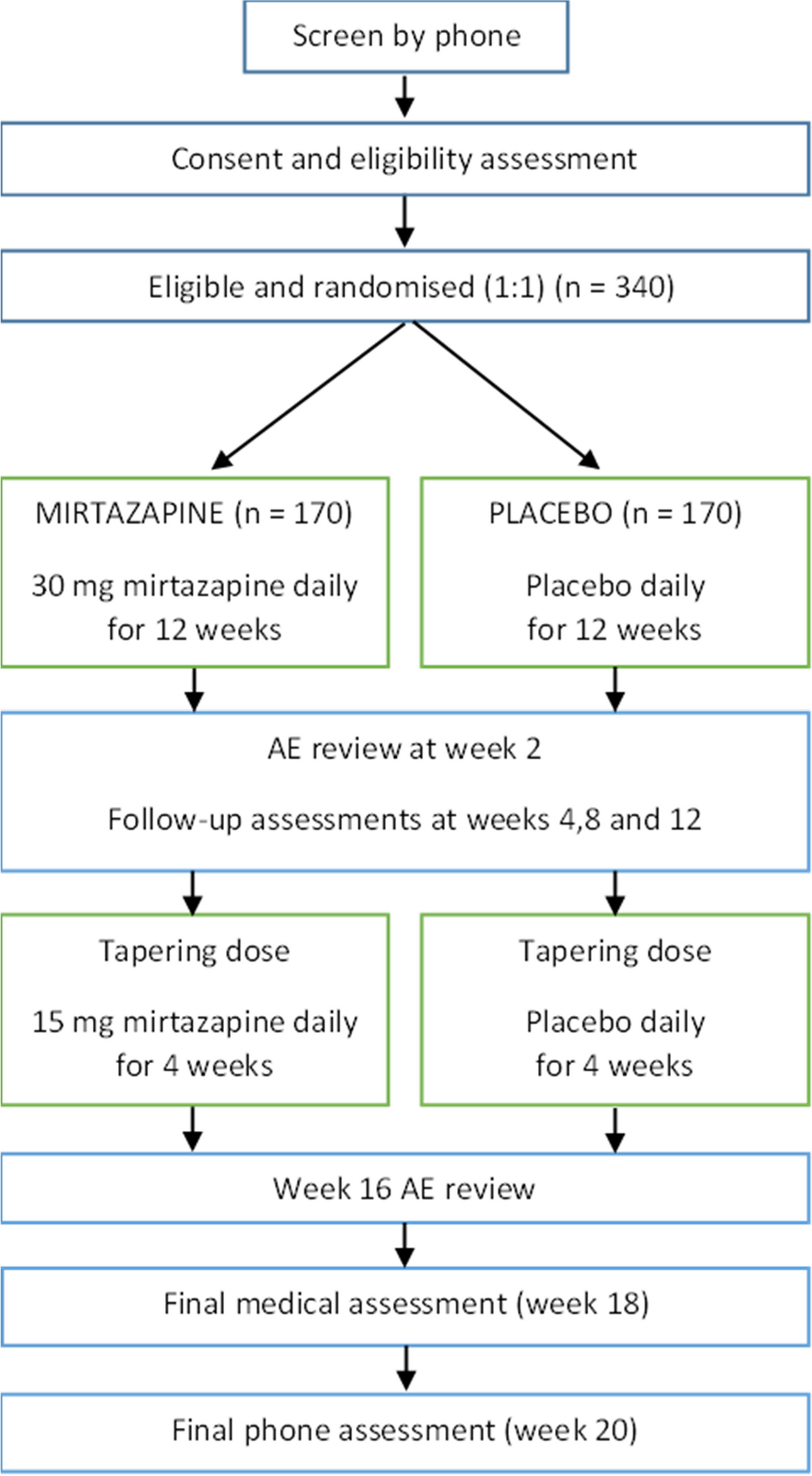




The study will be conducted as a two parallel-group exploratory randomized controlled trial (RCT) with an active control group. Participants will be randomized into either VR training or a control group, after baseline assessment, with an allocation ratio at 1:1 (Fig. 1). During the intervention period, participants in both groups will be followed up with a ten-minute phone call once per week, with standardized questions to each of the study conditions. This aims to increase fidelity and adherence to protocol, and adverse events will be monitored. For the participants in the intervention group, the phone call will also include technical issues if needed, and assessment of sense of presence (Multi-Modal Presence Scale [32]) during the intervention. Participants in both groups will answer weekly questionnaires regarding motivation (Situational Motivation Scale [33]) and fatigue (Fatigue Severity Scale [34]).
Fig. 1
The primary and secondary outcome measures will be re-administered at the end of the 5-week intervention period (T2) and 16 weeks (T3) after baseline. After T3, the first ten participants from the VR group will be asked to take part in individual qualitative interviews to gain in-depth understanding of their experience with the use of VR as a training method and participation in the intervention.
The RCT will follow the CONSORT statement [35] and is registered in ClinicalTrials.gov (NCT05443542) and Open Science Framework (osf.io/6gphy). When preparing this protocol, we used the SPIRIT reporting guidelines and the SPIRIT checklist is available as an additional file (Additional file 1).
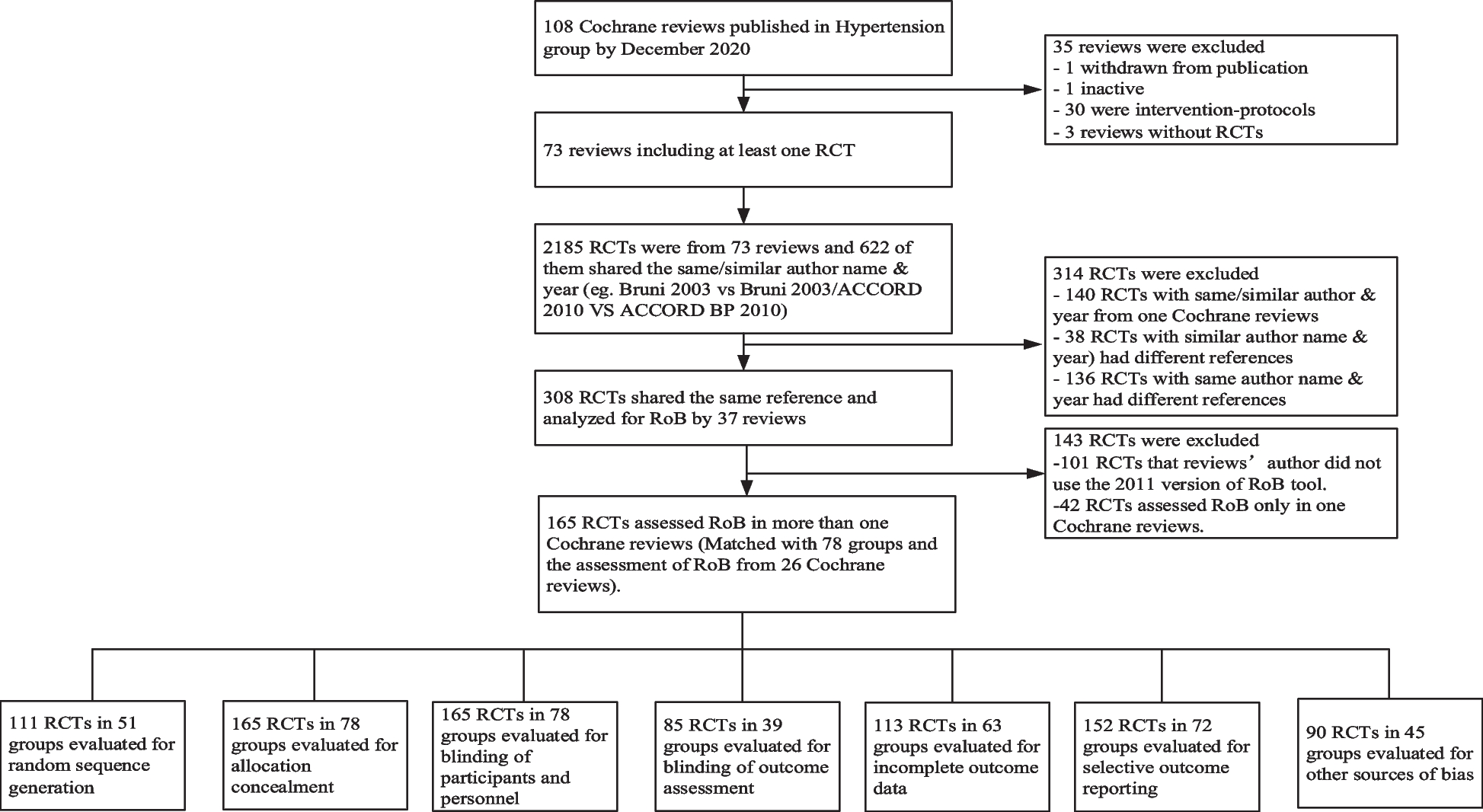
Study settingT1 (week 0), T2 (week 5), and T3 (week 16) assessments will be performed at Sunnaas Rehabilitation Hospital, the largest rehabilitation hospital in Norway and the owner of the study. Participants will receive tutorials on the use of the VR technology at baseline, and the interventions will be carried out in the participant’s homes (Fig. 2).
Fig. 2
Standard protocol items: recommendations for intervention trials (SPIRIT)
ParticipantsPatients with ABI who have been admitted to Sunnaas Rehabilitation Hospital will be considered for inclusion, and screened for eligibility. Eligible participants will receive a letter with an invitation to participate in the study. If participants have not responded to the letter within fourteen days, the project members will call them and ask whether they are interested in participating. A next of kin nominated by the patient will be included to obtain comparative information on the participants’ everyday functioning.
Eligibility criteriaInclusion criteria:
Patients with ABI (traumatic brain injury, cerebrovascular incidents, anoxia, encephalitis, and non-progressive brain tumors)
At least 12 months post injury
Aged 18–65 years
Objective or subjective impairments of processing speed, working memory, or sustained attention
◦Objectively determined via neuropsychological assessments of processing speed, working memory, and sustained attention documented in medical journal
◦Subjectively determined through a screening interview that include open-ended questions about perceived everyday processing speed, attention and working memory. The interview also contains the two items for attention and processing speed in the Rivermead Concussion Symptoms Questionnaire.
Participants need to:
◦Be physically able to operate VR equipment
◦Understand instructions in Norwegian or English
◦Be able to provide informed consent
Exclusion criteria:
Aphasia affecting the ability to understand instructions
Apraxia affecting the ability to operate the VR equipment
Visual neglect
Photosensitive epilepsy
Severe mental illness or active substance use disorder
Comorbid neurological disorders
Descriptive and outcome measuresAll outcome measures will be administered at T1, T2, and T3. The primary outcome is sustained attention and will be measured by the coefficient of variation (CoV) on the Conners Continuous Performance Test 3rd (CPT 3) [36]. Secondary outcomes are CPT 3, Mean hit Reaction time, Weschler Adult Intelligence Scale IV, Backwards Digit Span and Digit Sequencing [37], and patient competency rating scale [38]. Psychometric properties for each measure are acceptable. See Table 1 for an overview of all primary and secondary outcome measures, citations for psychometric properties, respondents, and time points.
Table 1 Outcome measures, respondents and time pointsAt baseline (T1), neuropsychological test measures and questionnaires will be used for descriptive purposes. The following neuropsychological test battery will be applied: the Trail Making Test 4 (shifting) and subtest 3 of the Color Word Interference Test (inhibition) from the Delis-Kaplan Executive Function System test battery [42]. Abstract reasoning will be measured with Similarities and Matrices from WAIS IV [37]. Furthermore, we will include Coding from the WAIS IV as a measure of processing speed [37]. Immersive tendencies questionnaire will be administered at baseline to assess personality traits that may impact the level of experienced immersion [43].
Demographic data such as marital status, length and type of education and work status, will be gathered. In addition, injury-related data such as type and localization of injury will be collected.
Randomization and allocation concealmentAfter the baseline assessment, the participants will be randomized into either the intervention or the control group. The randomization sequence will be generated electronically by an independent statistician, using block randomization [44] with a 1:1 ratio. Participants will be randomized after baseline assessment. The allocation sequence will be stored in a database that can only be accessed by the study’s principal investigator. Allocation will not be modified if the participant do not tolerate the intervention.
Blinding of participants and the researchers carrying out the intervention is impossible, but outcomes will be assessed by blinded assessors. Participants will be instructed to not reveal their group allocation to the outcome assessors. Data analysis will also be blinded as fake ID numbers will be assigned in the final database.
The personnel conducting the blinded assessments of the participants, will be trained by the research team to ensure data quality.
Study interventionsVirtual realityThe experimental intervention is playing a commercially available VR game 30 min per day, for 5 weeks. The game selected is BeatSaber [45], which is a rhythm-based VR game that requires the player to react to colored blocks presented at the rhythm beats. As the game progresses the requirements of the game increases as the blocks are presented faster thus taxing both processing speed, sustained attention, and working memory. In addition to its cognitive requirements, the game was chosen due to availability on different platforms, which may ease implementation. It also has many users globally, securing the availability of the game in the future. The participants will be provided with a VR headset in order to conduct the VR training sessions at home. Throughout the intervention period they will have access to support, either by phone or video conference. Each 30-min session will be scheduled individually, with the instruction to use an alarm system to keep track of time. There are no existing clinical guidelines regarding recommended dosage and intensity of VR training; thus, the session length is based on clinical experience at SRH.
The VR game tracks the actual time each participant has spent playing the game during the intervention period. The amount of time spent playing will be recorded and used as a measure of intervention adherence.
Control groupAn information booklet has been developed based on best practice evidence with information regarding compensatory strategies that participants can easily practice in their everyday lives. In addition to strategies, the booklet includes general information on topics that can affect cognitive functioning; national recommendation of physical exercise and physical activity, leisure activities (crossword puzzles, Sudoku, games and reading), sleep and nutrition. The control group will not be given a specific dosage; however, they will be encouraged to choose one or two topics to focus on during the intervention period. The control group will receive the same amount of therapist follow-up as the intervention group. The intervention group will not receive the information booklet.
At the end of the data collection period, the participants allocated to the control group will be offered to utilize VR as a method of training for a 5-week period. They will be given the possibility of the same amount of training and tutoring as the intervention group.
Qualitative data collectionTo investigate the participant’s experiences with VR as a method of cognitive training, semi-structured interviews will be conducted. An interview guide has been developed as recommended by Creswell [46], based on the acceptability framework developed by Sekhon and colleagues [47]. This includes questions regarding how participants feel about the intervention, the perceived amount of effort required to partake in the intervention, to what extent the participants understood the intervention, whether the participants perceived the intervention to result in its intended purpose, and the participant’s own belief that they can participate in the intervention. Interviews will be transcribed verbatim after each interview.
A pilot interview with one participant with previous experience with utilizing VR will be performed. After this an evaluation of the interview guide will be performed to assess whether amendments to the interview guide is needed.
Technical solutions and data managementThe intervention will be provided using the Oculus Quest 2 (Facebook Technologies, LLC). The Oculus Quest 2 is a wireless standalone VR headset that delivers the commercial VR game to the participants, creating the virtual environment through visual and auditory stimuli. The VR headset utilizes two motion-controlled hand controls that detect the hand movements of the participants in the virtual environment and provide haptic stimuli to the user. Oculus Quest 2 requires Meta accounts to set up the headset and to download and play the VR games. We will set up 20 Meta accounts, one for each headset.
Questionnaire data will be gathered using the University of Oslo’s solution for managing data, Services for Sensitive Data [48]. The TSD is an IT platform with a secure server that is approved for storing sensitive data for research purposes [48]. Questionnaires will be set up electronically using Nettskjema, which is a tool for designing and conducting online surveys [49].
All physical forms and test results will be kept in a locked cabinet. All data material will be recorded with the participant ID and will be de-identified. Only the researchers working on the project will have access to the list that connects participant IDs with names. Data will be stored electronically on a secure research server at SRH and will be deleted 5 years after the project period has ended. Only the research team will have access to the final trial dataset. Access to data is regulated by Norwegian laws regarding data protection and research ethics, and distribution of data is prohibited.
Statistical analysesDescriptive statistics will be performed to describe demographics, cognitive functioning and injury severity. Effect analysis of primary and secondary outcomes will be performed according to intention-to-treat analysis using data from all randomized participants, regardless of whether they complete the intervention. To determine changes in continuous outcome measures over time (T1, T2, and T3) between the groups, linear mixed-effects models will be used. Time and time-by-group interaction will be used as fixed effects and their interactions as indicators of the intervention effect. The main effect of group will be removed from the models to adjust for potential baseline differences [50]. In the same manner, we aim to explore associations between motivation, cybersickness, fatigue and sense of presence and interaction with time within the mixed-model framework. Estimated mean between group changes from baseline to T2 and T3 with 95% confidence intervals will be provided. For all outcomes, an alpha level of p = 0.05 will be applied.
Sub-group analyses of i.e. differences in duration since injury, age, and educational levels will be performed. Differences in continuous variables between groups will be tested using an independent sample t-test for normally distributed data, or by the Mann–Whitney U test for very skewed data. Linear regression analysis will be performed with registered adherence data as a possible predictor of treatment efficacy.
Sample size and power calculationComparable studies to guide a potential anticipated effect for power calculation are lacking. However, similar studies investigating the outcome of attention utilizing computerized gaming interventions report within-group improvement scaling from one to two standard deviations [51]. In addition, a cross-sectional study investigating a similar population at two time points with the same outcome measures was also utilized [52]. The sample size was calculated based on the coefficient of variation (CoV) of CPT as the primary outcome. A mean difference in change in CoV of CPT of 3% between baseline and follow up between the groups was defined as a clinically important difference. With equal allocation to both treatment groups and with an SD of 5%, power of 80%, and a significance level of 5%, the sample size was calculated to be 45 patients in each group. Allowing for 10% drop out, we aim to include a total of 100 patients.
The sample for qualitative interviews will be selected using selective sampling, meaning selecting individuals who are knowledgeable about the intervention or phenomenon being studied [53]. In this study, the sample will be the first ten participants that finish the VR intervention period.
Qualitative analysesAfter all the interviews have been conducted, thematic analysis will be applied, following these six steps: (1) Organizing and preparing data, including transcribing and sorting field notes. (2) Reading through all the data, to obtain a general sense of what the information given by the participants. (3) Coding the data and organizing the material into segments of texts to start bring meaning to the information. (4) Separate the information into “descriptions” and “themes”. (5) Check for interrelating themes and descriptions. (6) Interpret the meaning of the themes and descriptions [54].
Dissemination planThe study plans for at least three publications in international peer-reviewed journals. We expect the novelty and innovative aspects of the study to allow for publication in high-impact journals within the field of neurology/rehabilitation and health innovation. Results will be disseminated in relevant expert forums, national meetings, conferences, and popular scientific journals and reports. Members of the local research group all have central positions within research, clinical management, and innovation at SRH. Implementation of study findings into clinical practice will thus be highly feasible. SRH plays a major role in spreading knowledge and contributing to the implementation of new knowledge throughout the rehabilitation sector, i.e., through hosting the South Eastern Regional Competency Centre for Rehabilitation. This will provide ample opportunity for national dissemination of results. The international collaborators will help to improve international dissemination of the results. We also expect study findings to be of interest for the general public.
留言 (0)