
記住我

Traumatic brain injuries (TBIs) are responsible for more than 2.5 million emergency department visits and 214,000 admissions annually,1 with the majority not requiring neurosurgical (NSG) intervention. Traumatic brain injuries also contribute substantially to national health care costs, more than $40.6 billion annually according to a Centers for Disease Control and Prevention estimate2 for nonfatal TBI alone. It is in this setting that the Brain Injury Guidelines (BIG)3 and, subsequently, the modified Brain Injury Guidelines (mBIG)4,5 were developed to stratify and guide management of TBI with intracranial hemorrhage (ICH). The algorithms aim at optimizing health care resource utilization by selectively requiring intensive care unit (ICU) admission, repeat imaging to rule out progression of the injury, and NSG consultation. These guidelines challenged the traditional standard protocols for traumatic ICH adopted by a majority of trauma centers, which require routine ICU admission, repeat imaging, and NSG consult. Traditionally, protocol would mandate transfer to a tertiary hospital or trauma center for evaluation regardless of size of bleed or neurological stability when specialty resources are not available.
From a resource utilization perspective, a consequential application for mBIG is in the potential for reducing unnecessary, “low-value” interhospital transfers for mild TBI. In recent years, several validation studies5–9 have assessed the safety and reproducibility of BIG and its adaptations. However, the clinical and financial impact of these guidelines on interhospital patient transfer protocols remains poorly defined, especially in large metropolitan areas, where transport time between healthcare facilities may be rapid.
Our institution, an urban Level 1 trauma center, routinely receives transfers of patients with TBI and ICH from community and affiliate hospital emergency departments. The injury severity is not taken into account when the decision to transfer is made, given the lack of NSG availability at the transferring facilities. However, patients with mild TBIs who are at low risk for progression of their ICH and requiring NSG intervention could potentially be safely observed and managed at the affiliate institution without admission or transfer for higher level of care, with the application of the BIG or mBIG criteria. Thus, the purpose of this retrospective study is to validate the safety of mBIG for patients with TBI transferred for higher level of care and evaluate the potential resource savings associated with the reduction of low-value interhospital transfers. We further hypothesized that a large proportion of patients transferred for the management of their TBI could potentially remain at the transferring facility for observation, hence minimizing secondary overtriage.
PATIENTS AND METHODSThis retrospective observational study was approved by the institutional review board and adhered to the STrengthening the Reporting of OBservational studies in Epidemiology guidelines for proper reporting of methods, results, and discussion (Supplemental Digital Content, Supplementary Data 1, https://links.lww.com/TA/D589). The trauma registry of our Level I trauma center was queried for consecutive patients transferred to our facility from other hospitals for higher level and specialty care between January 1, 2017, and December 31, 2022, and who met all of the criteria for inclusion in mBIG. More specifically, the inclusion criteria were as follows:
18 years or older Blunt mechanism of injury Diagnosis of a TBI and/or a skull fracture Glasgow Coma Scale (GCS) score of 13 to 15 Absence of focal neurological deficitsTracked variables included transferring facility, demographics, mechanism of injury, admission GCS, history of anticoagulation or antiplatelet therapy, Injury Severity Score, Abbreviated Injury Scale (AIS) scores for all body regions, ICU admission, hospital length of stay (LOS), ICU LOS, NSG consult, and NSG interventions performed.
Transfer Request and Accepting ProcessAll requests for patient transfer from other facilities are fielded by our transfer center staff. Experienced registered nurses triage these requests and facilitate direct communication between requesting and accepting physicians. The covering trauma surgeon is the primary accepting physician. During the study period, accepting physicians had no access to imaging studies obtained at other facilities at the time of transfer acceptance. Patients with isolated TBI are routinely admitted to the neurocritical care ICU, while nonisolated TBI patients are admitted to the surgical ICU, and the covering neuro-intensivist is consulted for all patients admitted to an ICU. In addition, per institutional guideline, all TBI patients received NSG consultation, irrespective of TBI severity. Imaging studies obtained at transferring institutions were reviewed and uploaded into our picture archiving and communication system. Repeat head computed tomography (CT) scan (CTH) was routinely obtained on all TBI patients within a 6-hour interval from the initial CTH or earlier if medically justified. Nonadherence to this guideline was at the discretion of the covering trauma surgeon and based on patient factors and/or clinical circumstances. An example for justified nonadherence would be a patient with a misread CTH at the transferring facility demonstrating a TBI that was not confirmed on review by our own radiologists or on repeat imaging obtained at our institution. Institutional implementation and compliance toward mBIG did not occur until December, 2022, and did not impact the transfer process during the study period.
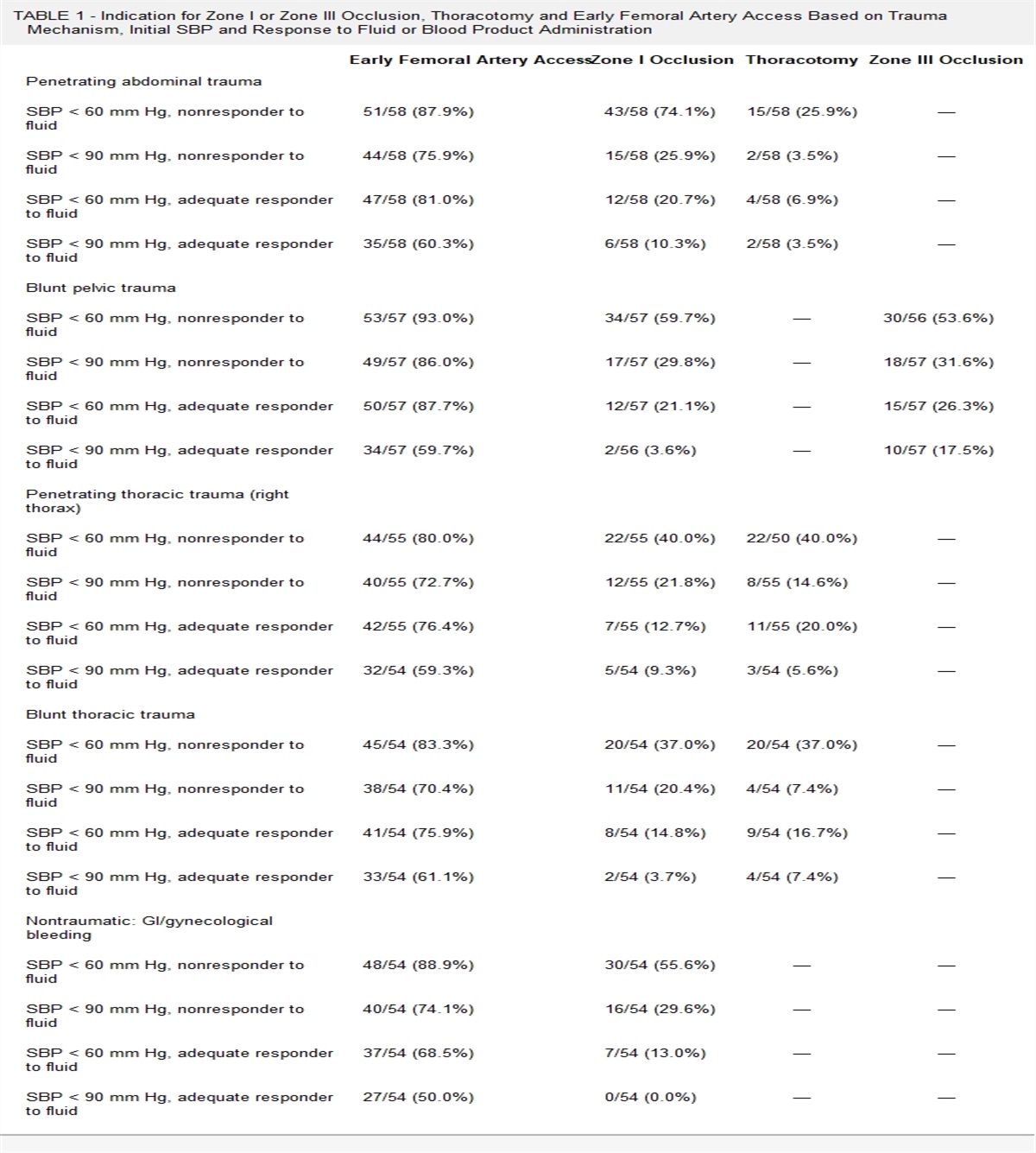
Classification Into mBIG CategoriesAll CTH of included patients were reviewed. Patients were stratified into mBIG1, mBIG2, or mBIG3 based on their initial CTH obtained at the transferring facility, using the clinical and radiologic criteria set by Khan et al.5 (Table 1). Measurements were performed in millimeters. Epidural hematomas and subdural hematomas (SDHs) were measured by maximum width, intraparenchymal hemorrhage was measured by maximum diameter along the largest axis, and traumatic subarachnoid hemorrhage was measured by maximum diameter and distribution. Classification was based on the most severe injury pattern in patients with more than one type of intracranial injury. All patients on anticoagulation or antiplatelet therapy (excluding aspirin, independent of dose) were categorized as mBIG3. All subsequent CTHs were also reviewed to determine radiographic progression of ICH. In addition, the electronic medical records were reviewed to abstract changes in neurological examination.
TABLE 1 - Modified Brain Injury Guidelines Radiologic Stratification, as per Kahn et al.5 mBIG 1 mBIG 2 mBIG 3 Skull fracture No Non-displaced Displaced SDH ≤4 mm 4–7.9 mm ≥8 mm EDH No No Yes SAH ≤3 sulci and <1 mm Single hemisphere or 1–3 mm Bihemisphere or >3 mm IVH No No Yes IPH ≤4 mm 4–7.9 mm ≥8 mm or multipleEDH, epidural hematoma; IPH, intraparenchymal hemorrhage; IVH, intraventricular hemorrhage; SAH, subarachnoid hemorrhage.
The primary outcome was progression of ICH on repeat imaging and/or requirement for NSG intervention. Secondary outcomes included ICU and hospital LOS, requirement for am NSG consultation, and total hospitalization charges. A subgroup analysis was performed for patients with isolated TBI, defined as TBI without (1) requirement for a specialty consult (spine, vascular, otorhinolaryngology, oromaxillofacial surgery, etc.), (2) high risk for complications or deterioration (prior brain surgery, non–drug-related coagulopathy), and (3) a significant concurrent extracranial injury (multiple rib fractures, complex pelvic fractures, etc.). This definition was more clinically relevant as compared with a definition based on AIS scores, especially in the setting of a request for transfer for higher level and subspecialty care, when injury scores are largely irrelevant.
Statistical analysis was performed using IBM SPSS for Windows, version 28.0 (IBM Corp., Armonk, NY). Continuous variables were presented as median with interquartile ranges (IQRs), and categorical variables as proportions and percentages. Proportions were compared using χ2 test or Fisher's exact test where appropriate. Statistical significance was set at p < 0.05.
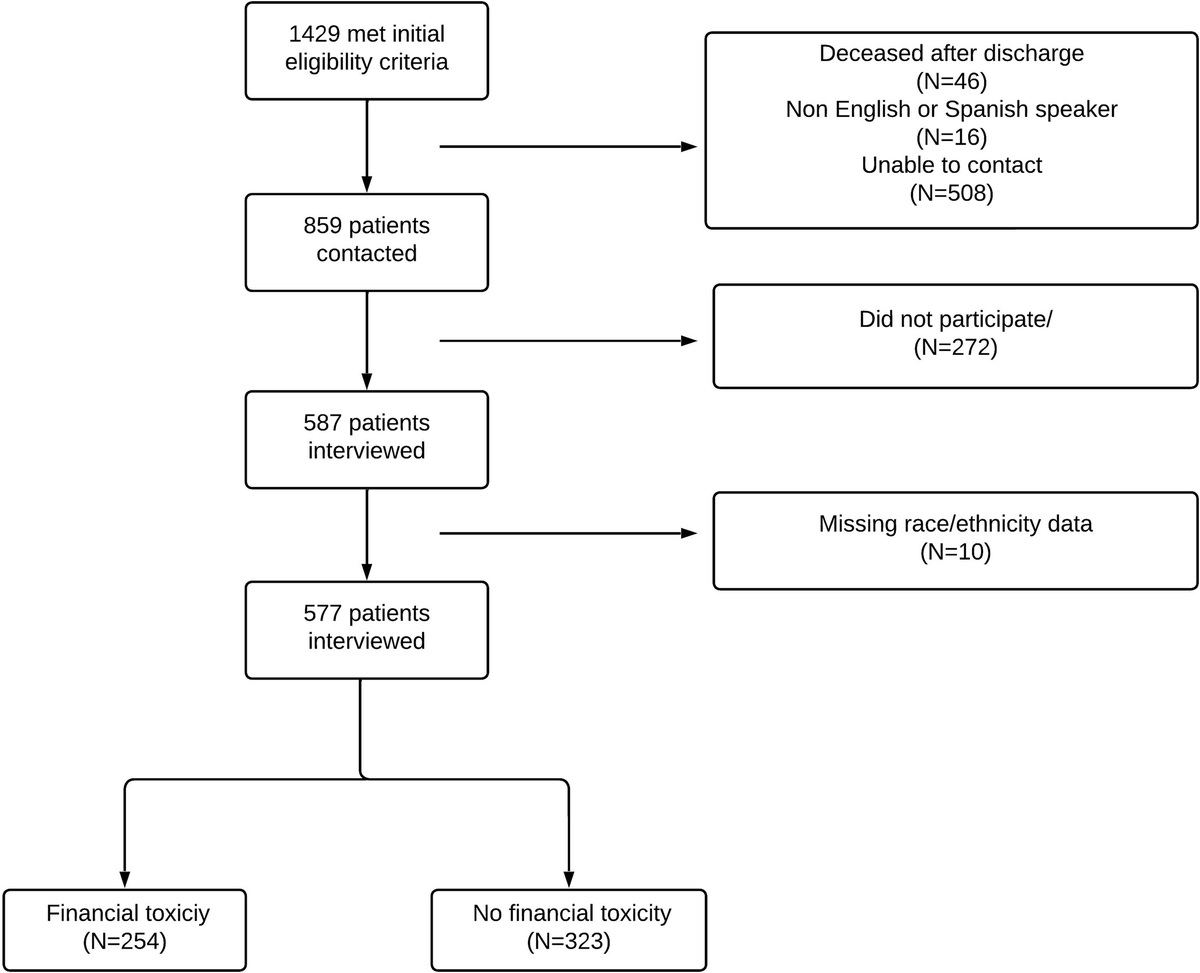
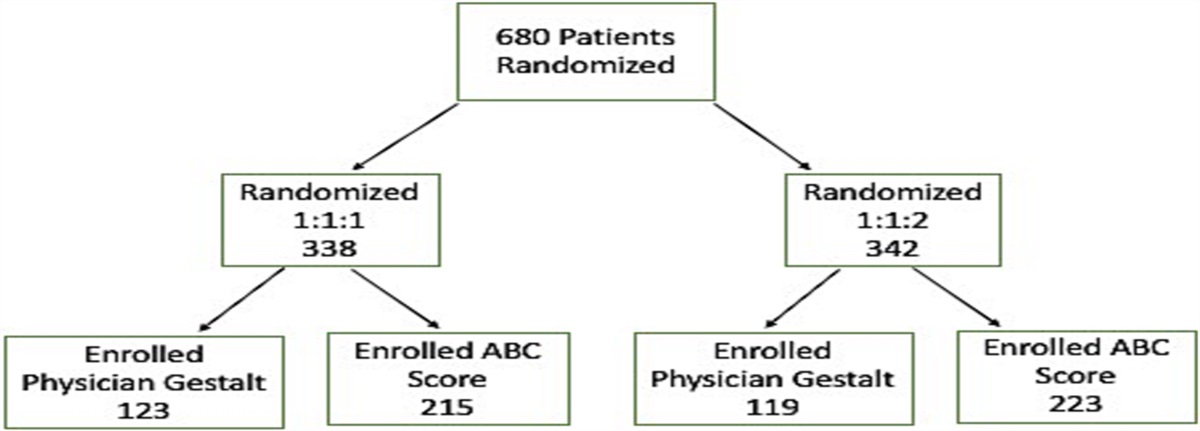
RESULTSOver the 6-year study period, 289 trauma patients meeting the inclusion criteria were transferred to our trauma center. The median age was 67 years (IQR, 46–79 years), and the majority were male (60.9%). The median Injury Severity Score was 10 (IQR, 9–17), and the median AIS head was 3 (IQR, 3–4). The primary injury mechanism was fall (70.6%), followed by assault (15.6%). Almost half (n = 139, 48.1%) of the patients were transferred from a single facility, an affiliate to our hospital. Overall, 69 patients (23.9%) were classified as mBIG1, 61 (21.1%) as mBIG2, and 159 (55.0%) as mBIG3 (Fig. 1). Table 2 outlines the demographics and clinical characteristics of patients based on mBIG classification.
 Figure 1:
Figure 1: Study flow chart.
TABLE 2 - Patient Demographics and Clinical Characteristics mBIG 1ISS, Injury Severity Score; ASA, aspirin.
Within the mBIG1 cohort (n = 69), 92.8% (n = 64) demonstrated radiographic stability or improvement of their ICH on their first repeat CTH. Three patients (n = 3, 4.3%) exhibited a slight increase in the size of the SDH on their repeat CTH not exceeding 4 mm, and they remained in the mBIG1 category. Two patients (n = 2, 2.9%) exhibited increase in the size of their SDH to 7 mm, radiologically progressing to mBIG2. No patient progressed to mBIG3, and none demonstrated clinical decline or required an NSG intervention (Table 3).
TABLE 3 - Patient Outcomes mBIG 1The vast majority of mBIG2 patients (n = 57, 93.4%) also demonstrated radiographic stability on their first repeat CTH. Two patients (n = 2, 3.3%) exhibited minor size increases in radiological features although remained in the mBIG2 category without clinical decline, and subsequent imaging showed stability. However, two additional patients (n = 2, 3.3%) in this cohort progressed from mBIG2 to mBIG3 and demonstrated acute neurological decline, representing 1.5% of patients with mBIG1 and mBIG2 injuries. The first patient initially presented with a 5-mm SDH, which was stable on repeat scan; however, at 48 hours from injury, the patient had worsening mental status, prompting further imaging demonstrating evolution of the SDH and interval development of an adjacent 4-cm intraparenchymal hemorrhage with uncal herniation. The second patient had blossoming of their subarachnoid hemorrhage, notably following vascular surgery initiation of baby aspirin for a focal common iliac artery dissection. Neurosurgical intervened with placement of a bolt for intracranial pressure monitoring on both patients; however, in both instances, because of advanced age, other traumatic injuries, and poor baseline function, per family decision, no further procedures were performed, and both patients expired.
Secondary OutcomesThe median hospital LOS for mBIG1 patients was 4 (IQR, 3–7), with 94.2% (n = 65) admitted to the ICU and 91.3% (n = 63) evaluated by NSG. Of those ICU admissions, most (n = 45, 65.2%) were downgraded in less than 48 hours. For mBIG2 patients, the median hospital LOS was 5 (IQR, 4–9) with the majority initially admitted to the ICU (n = 54, 88.5%). Again, most (n = 38, 62.3%) were in the ICU for less than 48 hours (Table 3). The median hospital charges per patient for mBIG1 and mBIG2 were $152,296 and $149,550, respectively. The aggregate hospital charges for mBIG1 and mBIG2 patients amounted to US $34.3 million over the 6-year study period.
Isolated TBIA subgroup analysis was performed for patients with isolated TBI (Table 4). These accounted for 78.3% (n = 54 of 69) of mBIG1 and 83.6% (n = 51 of 61) of mBIG2 patients. The total accounted for 80.8% of all mBIG1 and mBIG2 patients and for 36.3% of all transfers. Less than 1% (n = 1 of 105) required NSG intervention. The aggregate hospital charges for this subgroup of mBIG1 and mBIG2 patients amounted to US $19.8 million.
TABLE 4 - Subgroup Analysis of Patients With Isolated TBI mBIG 1In this study evaluating patients with TBI transferred to our Level I trauma center for higher level and subspecialty care, we found that almost half had mBIG1 or 2 injuries, amenable to observation without the need for repeat imaging, NSG consultation, and/or ICU admission. Moreover, more than 35% of transferred patients had minor isolated TBI, amenable for observation at the transferring facilities. No mBIG1 patient had a clinically significant progression of their TBI requiring NSG intervention. Overall, clinically significant progression of ICH occurred infrequently in 1.5% of patients with mBIG1 and mBIG2 injuries, and less than 1% required NSG intervention on subgroup analysis of isolated TBI. Implementation of the mBIG algorithm for patients presenting at low-level trauma centers with no subspecialty care and at nontrauma centers may be safe and substantially decrease secondary overtriage and resource utilization. In addition, classification of these patients based on mBIG before transfer (when transfer is required for associated injuries) may decrease ICU bed utilization and NSG consultation.
Direct admission and secondary triage of severely injured trauma patients to a trauma center is associated with higher survival.10,11 Often, however, trauma patients with minor injuries that do not require any intervention are transferred to higher level trauma centers because of lack of specialty and subspecialty care. In fact, up to 40% of these patients may be secondarily overtriaged, resulting in overutilization of valuable resources and in patient dissatisfaction.12–14 To mitigate secondary overtriage, nonspecialized providers at lower level trauma centers and nontrauma centers should be equipped with the necessary tools and evidence-based practices to appropriately triage patients and maximize the benefits of transferring a trauma patient with non–life-threatening injuries to higher level trauma centers. This may prove challenging, however, given the wide range of injuries that these patients present with. With this work, we focus on a specific group of trauma patients with TBI at low risk for progression who account for a large proportion of secondary overtriage.15,16
Missed injury with ICH can have devastating consequences, and patient care should be allocated with safety as the priority. This study demonstrates that the mBIG algorithm5 provides a safe framework to assess patient risk for progression of TBI in this patient population, and therefore, resources can, and should, be assigned accordingly. Several validation studies6–9 support this. In their prospective analysis using a slight algorithmic variation of the original BIG,3 Ross et al.7 found that no BIG 1 or BIG 2 patients demonstrated a clinical decline or required any further NSG intervention. Similarly, Tourigny et al.6 reported a sensitivity for predicting the need for a transfer of 100% (95% confidence interval, 93.2–100%) and a specificity of 9.4% (95% confidence interval, 6.8–12.6%) using a different variation of the BIG guidelines by Martin et al.8 and posited that they could reduce the number of transfers to their level 1 trauma centers by 6% to 25%. Capron et al.17 found that more than 30% of transfers of TBI patients to a Level I trauma center can be prevented with the application of the BIG criteria. Yun et al.18 reported that only warfarin use and an SDH 1 cm or larger were independent predictors for admission of TBI patients to a Level I trauma center. Our work indicates that implementing the mBIG algorithm for patients who present with a TBI to transferring facilities that are nontrauma centers may result in a substantial decrease in low-value transfers and secondary overtriage. In fact, we found that more than 35% of these patients with isolated TBI that meet mBIG1 and 2 criteria can be observed without the need for repeat imaging and/or NSG consultation. For the remaining nonisolated TBI patients who require transfer for associated injuries, there is opportunity to prevent low-value ICU admissions and NSG consultation by classifying these patients into mBIG before transfer and determining their disposition using the framework that the guideline provides.
It is important to interpret the results of this study in the context of seemingly similar, previously published, work. The BIG criteria have been repeatedly validated in various settings, even for use at a Level III trauma center.8 Martin et al.8 modified the validated BIG criteria to create a more conservative classification to allow for their application at their Level III trauma center. Moreover, in their revised classification, they included patients with a GCS score of <13. Similarly, Capron et al.17 suggested another revision to the BIG classification, with all patients with a GCS score of <15 be classified as BIG3. We included patients with a GCS score of 13 to 15, as per the inclusion criteria for mBIG, without incorporating any additional modifications, either related or not to the admission GCS. Based on our findings, the mBIG would not require any modifications if to be applied at transferring facilities, given its reliability. In addition, Capron et al.17 reported on transfers from a catchment area encompassing 75 miles with several rural and semirural communities. In contrast, our institution is located in a major metropolitan city with our referring hospitals (nontrauma centers) embedded within the community and a relatively close proximity. Therefore, the application of mBIG in this type of urban setting differs substantially and comes with a different set of transport challenges and implications. Pragmatically, we may be able to rely more heavily on our referring hospitals with improved partnerships and communication, given the safety net of a relatively rapid transfer between hospitals if a patient were to decline and require higher level of care.
Interhospital transfers are resource heavy and expensive. They require ambulance and transport staff and essentially create a double workload at both the origin and receiving facility — at minimum from the emergency or trauma teams, radiologist, and imaging technicians to the hospital registrars and support staff. Less tangible factors, such as time and potential delay in care due to transport, must be taken into consideration. Even if a transfer was preferred because of resource limitations at the origin facility, or insurance reasons, certain patients may be more appropriately served on a monitored floor or step-down unit, rather than with a brief and costly ICU stay. There may even be a role in leveraging ICU telemedicine to reduce low-value interhospital transfers.19,20 Selective repeat CTH and NSG consultations should be implemented over a blanket approach. Pragmatically, policy changes and interhospital agreements can be made to identify these low-value transfers, minimize unnecessary consults, and optimize ICU and hospital bed allocation.
CONCLUSIONThis is a retrospective single-institution study and has several limitations. In contrast to the original mBIG studies,4,5 intoxication, which can adversely limit neurological examinations, were not factored into analysis because records were difficult to consistently obtain from outside facilities. We recognize that, while the referring nontrauma hospitals in our study have on- or off-site radiologists available, we are unable to fully take into account the referring hospital's capabilities for prompt radiology reads of CTHs or personnel availability for serial neurological monitoring.
Furthermore, cost analysis was based on total hospital charges and not the direct and indirect costs of hospitalization, as they were not adequately captured in our trauma registry. Transport times were not accounted for, although, given the close proximity of the vast majority of transferring facilities to our institution and the prioritization of these transfers by our transfer center, transport times are typically short. Despite these limitations, this study illustrates the vast consumption of resources that may be saved with minimization of low-value transfers for low-risk TBI. More than 35% of interfacility transfers for minor isolated TBI are low value and may potentially be safely deferred in an urban health care setting. Higher level trauma centers may develop interhospital processes and agreements to optimize resources and avoid secondary overtriage and unnecessary admissions without impacting outcomes.
AUTHORSHIPA.S. and G.B. contributed in the literature review. A.S. and G.B. contributed in the study conception and design. A.S., N.M., M.M., and G.B. contributed in the data collection. A.S., N.M., M.M., and G.B. contributed in the analysis and interpretation of data. A.S. and G.B. contributed in the drafting of manuscript. M.M., S.T., S.L., R.C., and D.M. contributed in the critical revision.
DISCLOSUREConflicts of Interest: Author Disclosure forms have been supplied and are provided as Supplemental Digital Content (https://links.lww.com/TA/D590).
REFERENCES 1. National Center for Injury Prevention and Control. Traumatic Brain Injury. Centers for Disease Control and Prevention. Atlanta, GA. Available at: https://www.cdc.gov/traumaticbraininjury/data/index.html. Accessed September 7, 2023. 2. Miller GF, DePadilla L, Xu L. Costs of nonfatal traumatic brain injury in the United States, 2016. Med Care. 2021;59(5):451–455. 3. Joseph B, Friese RS, Sadoun M, Aziz H, Kulvatunyou N, Pandit V, et al. The BIG (brain injury guidelines) project: defining the management of traumatic brain injury by acute care surgeons. J Trauma Acute Care Surg. 2014;76(4):965–969. 4. Khan AD, Elseth AJ, Brosius JA, Moskowitz E, Liebscher SC, Anstadt MJ, et al. Multicenter assessment of the brain injury guidelines and a proposal of guideline modifications. Trauma Surg Acute Care Open. 2020;5(1):e000483. 5. Khan AD, Lee J, Galicia K, Billings JD, Dobaria V, Patel PP, et al. A multicenter validation of the modified Brain Injury Guidelines: are they safe and effective? J Trauma Acute Care Surg. 2022;93(1):106–112. 6. Tourigny JN, Boucher V, Paquet V, Fortier É, Malo C, Mercier É, et al. External validation of the updated brain injury guidelines for complicated mild traumatic brain injuries: a retrospective cohort study. J Neurosurg. 2022;137(3):782–788. 7. Ross M, Pang PS, Raslan AM, Selden NR, Cetas JS. External retrospective validation of brain injury guidelines criteria and modified guidelines for improved care value in the management of patients with low-risk neurotrauma. J Neurosurg. 2019;1–6. 8. Martin GE, Carroll CP, Plummer ZJ, Millar DA, Pritts TA, Makley AT, et al. Safety and efficacy of brain injury guidelines at a level III trauma center. J Trauma Acute Care Surg. 2018;84(3):483–489. 9. Joseph B, Aziz H, Pandit V, Kulvatunyou N, Sadoun M, Tang A, et al. Prospective validation of the brain injury guidelines: managing traumatic brain injury without neurosurgical consultation. J Trauma Acute Care Surg. 2014;77(6):984–988. 10. Newgard CD, McConnell KJ, Hedges JR, Mullins RJ. The benefit of higher level of care transfer of injured patients from nontertiary hospital emergency departments. J Trauma. 2007;63(5):965–971. 11. MacKenzie EJ, Rivara FP, Jurkovich GJ, Nathens AB, Frey KP, Egleston BL, et al. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354(4):366–378. 12. Ciesla DJ, Sava JA, Street JH, Jordan MH. Secondary overtriage: a consequence of an immature trauma system. J Am Coll Surg. 2008;206(1):131–137. 13. Crowley BM, Griffin RL, Andrew Smedley W, Moore D, McCarthy S, Hendershot K, et al. Secondary overtriage of trauma patients: analysis of clinical and geographic patterns. J Surg Res. 2020;254:286–293. 14. Sorensen MJ, Von Recklinghausen FM, Fulton G, Burchard KW. Secondary overtriage: the burden of unnecessary interfacility transfers in a rural trauma system. JAMA Surg. 2013;148(8):763–768. 15. Dengler BA, Plaza-Wüthrich S, Chick RC, Muir MT, Bartanusz V. Secondary overtriage in patients with complicated mild traumatic brain injury: an observational study and socioeconomic analysis of 1447 hospitalizations. Neurosurgery. 2020;86(3):374–382. 16. Moslehi S, Haghdoust Z, Masoumi G, Rad EH, Nouri F, Kouchakinejad-Eramsadati L, et al. Secondary overtriage of trauma patients in a trauma center: frequency and associated factors. J Inj Violence Res. 2023;15(1):45–54. 17. Capron GK, Voights MB, Moore HR 3rd, Wall DB. Not every trauma patient with a radiographic head injury requires transfer for neurosurgical evaluation: application of the brain injury guidelines to patients transferred to a level 1 trauma center. Am J Surg. 2017;214(6):1182–1185. 18. Yun BJ, White BA, Benjamin Harvey H, Prabhakar AM, Sonis JD, Glover M, et al. Opportunity to reduce transfer of patients with mild traumatic brain injury and intracranial hemorrhage to a level 1 trauma center. Am J Emerg Med. 2017;35(9):1281–1284. 19. Fortis S, Sarrazin MV, Beck BF, Panos RJ, Reisinger HS. ICU telemedicine reduces interhospital ICU transfers in the Veterans Health Administration. Chest. 2018;154(1):69–76. 20. Fortis S, Weinert C, Bushinski R, Koehler AG, Beilman G. A health system-based critical care program with a novel tele-ICU: implementation, cost, and structure details. J Am Coll Surg. 2014;219(4):676–683.
留言 (0)