
記住我

The peeling of the internal limiting membrane (ILM) and injection of endotamponade agents are part of the pars plana vitrectomy (PPV) procedure, which is the primary surgical method used to treat macular hole retinal detachment (MHRD). Internal limiting membrane peeling reduces traction, creates greater retinal redundancy to facilitate anatomical closure, and removes scaffolds for cellular proliferation.1 In 2010, Michalewska et al2 introduced a novel technique to improve surgical outcomes in individuals with MHRD by using an inverted ILM flap. However, the method may be limited by the following reasons: 1) eyes with MHRD have a longer axial length than that of eyes without MHRD, and during the insertion–removal of instruments, the ILM flap flutters easily because of balanced salt solution (BSS) flow; 2) the ILM flap curls after removal from the retina, making it difficult to tilt the entire macular area; 3) the ILM flap detaches easily and gets aspirated during fluid–air exchange (FAX)3; and 4) when endotamponade agents are filled, the position of the ILM flap is likely to change. Therefore, with this technique, MH closure is not achieved in some patients with MHRD. MHs in certain individuals were unclosed which may affect postoperative vision recovery and result in the retinal detachment recurrence.4 To address these issues, in this study, we describe a “viscoelastic agent pool” technique for improving inverted ILM flap stability in patients with MHRD. In this novel technique, we aim to form a “no-flow” pool in the posterior pole using diluted intraoperative viscoelastic agents. In this stationary liquid, the ILM flap is relatively easy to operate and remains stable during the entire operation. We also evaluated the functional and anatomical outcomes and complications associated with the technique.
Methods PatientsThe procedures of this investigation were performed in compliance with the Declaration of Helsinki. All patients provided a signed informed consent form. In this study, we included patients who had been clinically diagnosed with MHRD at The Eye Hospital at Wenzhou Medical University (Hangzhou) between June 2022 and December 2022. The inclusion criteria were clinical presentation of MHRD and axial length equal to or greater than 26.5 mm. The diagnostic criteria for MHRD were as follows: B-scan in spectral domain-optical coherence tomography showed that there was retinal detachment at the edge of MH, and MH was the initial retinal break (rhegmatogenous retinal detachment combined with MH was not included). The study excluded individuals who had a history of retinal surgery, uveitis, retinal vessel disorders (such as retinal vascular occlusion), or had experienced trauma.
Patient ExaminationAll patients underwent best-corrected visual acuity (BCVA) assessment, dilated fundus examination by slitlamp, ultra-widefield retinal imaging, IOL master, and spectral domain-optical coherence tomography (Spectralis OCT; Heidelberg Engineering, Heidelberg, Germany), both preoperatively and postoperatively. Visual acuity before and after surgery was transformed into logarithm of minimal angle of resolution (logMAR) equivalents. The minimum MH diameters were measured by the onboard software of Heidelberg Spectralis OCT. To minimize the error caused by axial length, we corrected the MH diameter using the formula mentioned in the literature.5
Surgical outcomes included the MH closure rate (closed MHs were categorized into two patterns by SD-OCT: Type 1 was MH closed without a neurosensory retinal defect at the fovea and Type 2 was MH closed with a foveal neurosensory retinal defect at the fovea)6 and retinal reattachment rate. Postoperative complications included excessive gliosis7 and endophthalmitis. The correlation among parameters was assessed using linear regression. The SPSS software package V.26.0 (SPSS, Inc, Chicago, IL) was used for all statistical analyses, and the significance level was set at P < 0.05.
Preparation of Diluted Sodium Hyaluronate Solution for “Viscoelastic Agent Pool”We used Pe-Ha-Luron F 1.6 NaHa containing 16 mg of sodium hyaluronate (Albomed GmbH, Schwarzenbruck, Germany). The solution was diluted with BSS in a 2.5-mL syringe to increase the volume from 0.3 mL to 1.5 mL. After adding BSS into the sodium hyaluronate solution, to ensure that the concentration within the syringe is uniform, we leave some space in the syringe to shake it up and down. The purpose of this method is to allow for thorough mixing of the BSS and the sodium hyaluronate solution. During this process, air is also incorporated into the solution, resulting in the formation of evenly dispersed microbubbles. At this point, we consider that the sodium hyaluronate solution has been homogeneously diluted (Figure 1).
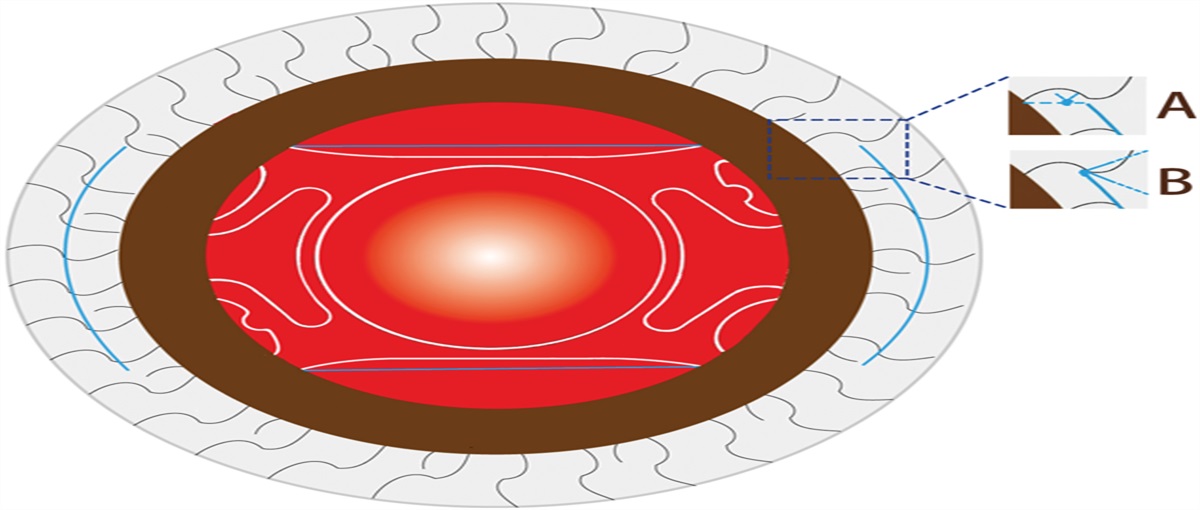
 Fig. 1.:
Fig. 1.: Schematic representation of diluted sodium hyaluronate solution preparation. A. Correct method for sodium hyaluronate injection is through the tail of the syringe; incorrect method is through the head of the syringe. B. Syringe head is blocked with a finger and the BSS is injected through the tail of the syringe. C. After loading BSS (1.2 mL) into an inverted syringe, it is gently shaken vertically to ensure adequate mixing. D. When microbubbles are visible, the dilution of the sodium hyaluronate solution is considered complete.
Surgical TechniqueFigure 2 and Supplemental Digital Contents 1 and 2 (see videos, https://links.lww.com/IAE/C161 and https://links.lww.com/IAE/C162) provide a description of the procedure known as the “viscoelastic agent pool” technique.
 Fig. 2.:
Fig. 2.: Surgical procedure of diluted sodium hyaluronate solution–assisted inverted ILM flap technique in MHRD. A. ILM is peeled, sparing the temporal ILM flap. B. Diluted sodium hyaluronate solution is injected to form the “viscoelastic agent pool.” C. Temporal ILM flap is inverted in the “viscoelastic agent pool.” D. Autologous whole blood is injected onto the ILM flap in the “viscoelastic agent pool.” E. FAX is performed through the optic disk by a backflush needle. F. Silicon oil flow is directed perpendicular to the macula.
In brief, under retrobulbar anesthesia, a standard three-port PPV was performed using the Constellation sutureless 23-G or 25-G vitrectomy system (Alcon Laboratories, Inc., Fort Worth, TX) under a contact lens by a single surgeon (B.B.Z.). The primary surgical procedure was as follows:
Posterior hyaloid detachment was manually induced, and peripheral hyaloid was carefully and completely trimmed. Indocyanine green (ICG, 5 mg/mL; Dandong Yichuang, Inc, Dandong, China) was applied to stain the ILM, followed by immediate lavage. The ILM was firmly grasped and carefully removed from the edge of the MH; the remaining temporal-quarter ILM was trimmed into a rectangular flap using a vitreous cutter. The subretinal fluid was drained with a backflush needle from the macular hole in all cases to reduce the height of retinal detachment. Diluted sodium hyaluronate solution was gently introduced over the macula to form a “viscoelastic agent pool.” Using the ILM forceps, the ILM flap cover of the MH was inverted inside the “viscoelastic agent pool.” The flap was brought in contact with the flat surface to adhere to the edge of the MH by the closed ILM forceps tip. The autologous whole blood was collected from the elbow vein of the patient by the operating room nurse during the surgery. After collection, one to two drops of autologous whole blood were injected into the viscoelastic agent pool immediately with a 27-G needle mounted on a 1-mL syringe. The injected autologous blood needs to rest for more than 30 seconds before the FAX. During FAX, a backflush needle was used to drain the vitreous cavity fluid through the surface of the optic disk. Moreover, it was important to avoid touching the edge of the blood clot to prevent it from wrapping around the ILM. All patients underwent endotamponade with silicone oil or 18% perfluoropropane (C3F8) gas. When silicone oil was injected, the surface of the blood clot was covered with silicone oil from top to bottom to prevent the blood clot from being laterally pushed away by the silicone oil flow. The patients were advised to keep their face down for at least 1 week. Results Patient CharacteristicsThis study recruited 10 patients with MHRD (two men and eight women). The mean age of the patients was 66.70 ± 8.75 (range, 55–84) years. The average follow-up duration was 6.01 ± 1.71 (range, 3.10–8.40) months. The mean preoperative BCVA was 1.38 ± 0.48 (range, 0.8–2.3) logMAR (20/125 to 20/2000). The mean axial length was 29.34 ± 1.53 (range, 27.10–30.93) mm, the mean MH diameter was 562.90 ± 277.63 (range, 137–1,029) µm, and the mean corrected MH diameter was 685.30± 345.65 (range, 172–1,325) µm. The three-channel PPV was performed in five eyes, whereas vitrectomy combined with phacoemulsification and intraocular lens implantation was performed in the remaining five eyes with coexisting cataract. In our study, Patient 1 received endotamponade with 18% C3F8 gas, whereas the others received it with silicone oil.
OutcomesAt the final follow-up, the silicone oil was completely removed in all eyes. The mean postoperative BCVA was 1.15 ± 0.50 (range, 0.5–1.7) logMAR (20/63 to 20/1000). The postoperative BCVA showed improvement (improved ≥5 letter in the Early Treatment Diabetic Retinopathy Study8) in six eyes (60%) and no improvement in four eyes (40%). All eyes (100%) exhibited MH closure after the surgery, with Type 1 closure observed in all 10 eyes (100%; Figure 3). The retinal reattachment rate was 100%. No severe postoperative complications, including excessive gliosis or endophthalmitis, were observed (Table 1). The results of simple and multiple linear regression analyses showed that postoperative BCVA improvement was not correlated with sex (P = 0.39), age (P = 0.10), axial length (P = 0.30), and corrected MH diameter (P = 0.20).
 Fig. 3.:
Fig. 3.: Preoperative and postoperative spectral domain-optical coherence tomography scans in patients (1–10) showing anatomical macular hole closure.
Table 1. - Demographic Data of Patients Number Age (Years) Sex Eye Axial Length (mm) Tamponade Surgical Procedure Maculer Hole Diameter (μm) Adjusted Maculer Hole Diameter (μm) Follow-up month Types of Macular Hole Closure Retinal Reattachment Remnant SRF Excessive Gliosis Endophthalmitis BCVA, Snellen (logMAR) Pre BCVA, Snellen (logMAR) Post BCVA Improvement in ETDRS Letter Scores 1 65 F OS 30.9 C3F8 23GPPV+P+I 1,029 1,325 7.03 1 Yes No No No 1.0 (20/200) 1.7 (20/1,000) −35 2 56 F OD 29.1 Silicone oil 25GPPV 691 838 7.17 1 Yes No No No 1.0 (20/200) 0.7 (20/100) 15 3 55 F OD 27.3 Silicone oil 25GPPV 694 789 7.27 1 Yes No No No 1.6 (20/800) 0.8 (20/125) 40 4 65 F OD 30.7 Silicone oil 23GPPV+P+I 741 948 6.03 1 Yes No No No 1.0 (20/200) 0.7 (20/100) 15 5 77 M OS 30.3 Silicone oil 23GPPV+P+I 159 201 7.17 1 Yes No No No 1.7 (20/1,000) 1.7 (20/1,000) 0 6 63 F OD 27.1 Silicone oil 25GPPV 639 722 3.1 1 Yes No No No 0.8 (20/125) 0.8 (20/125) 0 7 67 F OS 30.1 Silicone oil 25GPPV 137 172 4.63 1 Yes No No No 1.0 (20/200) 0.5 (20/63) 25 8 70 F OD 30.2 Silicone oil 23GPPV+P+I 481 605 5.33 1 Yes Yes No No 1.7 (20/1,000) 1.6 (20/800) 5 9 84 F OD 27.3 Silicone oil 25GPPV 690 785 8.4 1 Yes No No No 2.3 (20/2000) 1.7 (20/1,000) 0 10 65 M OS 30.5 Silicone oil 25GPPV 368 468 3.93 1 Yes No No No 1.7 (20/1,000) 1.3 (20/400) 20Type 1 closure: closed without foveal neurosensory retinal defect; Type 2 closure: closed with foveal neurosensory retinal defect.
P+I, phacoemulsification and intraocular lens implant.
In the standard inverted ILM flap technique, preventing the floating and displacement of the ILM flap in the detached retina could be challenging. To improve the stability of ILM flaps, surgeons have attempted different techniques. Lai et al9 used a viscoelastic agent to block the MH and then applied the perfluoro-n-octane required for stabilizing inverted ILM flaps. Yang and Kim10 manipulated the intravitreal fluid flow direction and released the negative pressure to handle the ILM flaps. Using a multilayer ILM flap covering the MH, Xu et al11 obtained better anatomical outcomes than those with single ILM peeling. Finn and Mahmoud12 stabilized the ILM by using perfluorocarbon liquid in myopic hole associated with rhegmatogenous retinal detachment. The technique involves creating a hinged ILM door, which relieves traction contributing to the macular holes. This technique preserves more ILM and provides the advantage of confirmed placement of the ILM back in place draped over the MH to close it. Because of the medical costs for patients and the learning curve of different levels and ranks of surgeons, an easy and effective technique is needed to address this dilemma.
The “viscoelastic agent pool” technique is a different method from the above techniques. First, a diluted sodium hyaluronate solution was used instead of a pure solution. Sodium hyaluronate is an ophthalmic intraoperative viscoelastic agent. The high molecular weight and long chains of this material create back pressure, a strong surface tension, and a high pseudoplasticity.13 Therefore, if the sodium hyaluronate solution is injected directly into the BSS, a mass of transparent strips will be formed. These viscoelastic agent strips could slip on the retinal surface and would not provide a gripping force to the ILM flap. To overcome this phenomenon, we diluted the sodium hyaluronate solution to reduce its surface tension and shook it multiple times to obtain a homogenized puddle solution. Subsequently, when we injected this solution above the MH, it formed a relatively stable “pool.” The “viscoelastic agent pool” resembles a space isolated from the BSS where the inverted ILM flap flutter is significantly reduced and maneuverability is increased. At the same time, owing to the viscosity of viscoelastic agents, the ILM flap is easily reattached to the retinal surface at the edge of the MH. On reviewing the literature, researchers have used perfluoron to stabilize the ILM flap. The surface tension of the diluted sodium hyaluronate solution is much lower than that of perfluoron, which is not enough to flatten the macular and provide a stable state for peeling the ILM. It nonetheless has a few favorable points. First, we should inject the diluted sodium hyaluronate solution before the ILM flap is inverted in the design of the surgical plan, rather than when peeling off the ILM. When the ILM flap is inverted in the viscoelastic agent pool, the flap remains stretched, unlike in perfluoron where it tends to curl and form a strip, thus it is easier to flatten. Second, viscoelastic agents have lower medical costs compared with perfluoron. Thirdly, the viscosity of the sodium hyaluronate solution was diminished due to its dilution, resulting in effortless discharge. However, the residual solution poses no harm to the patient and does not necessitate further removal. These are precisely the reasons we opt for viscoelastic agents.
The second advantage of this technique is the use of a temporal ILM flap. The inverted ILM flap brings Müller cell remnants to stimulate glial cell proliferation and acts as a scaffold for MH healing.14 We used a single-layer temporal inverted flap to construct the roof for the MH. The advantage of the temporal ILM flap is as follows: During FAX, the flute needle is placed on the surface of the optic disk, and the direction of flow coincides with the edge of the temporal ILM flap. The aspiration force can increase the ILM flap flatness; moreover, the temporal ILM flap resembles a door, allowing the subretinal fluid to be easily removed from the optic disk.
Third, autologous blood was used as the top layer of the roof for MH. When autologous blood was injected into the viscoelastic agent pool, it slowly falls to the surface of the ILM flap and covers it and the surrounding retinal surface, forming a slight diffusion. When blood clot form, it could provide stable adhesion to the retinal surface and prevent the ILM flap displacement caused by flow during FAX and act a mechanical fixation, and after FAX, the blood clot serves as a distinct marker for the ILM flap. We found that there were no cases of blood clot displacement caused by FAX and silicone oil flow. Postoperatively, the autologous blood on the surface of the ILM flap may also contain components that could potentially help in the wound healing process and improve the MH closure rate to a certain extent.15 Therefore, we believe that autologous blood serves as an adjunctive technique in the use of viscoelastic agent pool technique.
In this study, nine patients received tamponade with silicone oil and one patient with gas (C3F8). It should be clarified that the use of silicone oil is not necessary for the viscoelastic agent pool technique. Primarily associated with the patient's medical condition, such as a restricted ability to sustain face-down position for a prolonged duration or impaired visual capacity in the non-operated eye impacting daily activities. Moreover, silicone oil makes it easier to observe the absorption of blood, the morphologic changes of retinal reattachment, and the early healing of macular holes, which cannot be observed with gas tamponade alone.
Surgery for MHRD aims to close the MH and achieve successful retinal reattachment. In previous research, the closure rate of MH in MHRD ranges from 10% to 100%, whereas the rate of retinal reattachment ranges from 43% to 92%.8 Our anatomical outcomes were better than those of previous studies. Regarding the viscoelastic agent pool technique, we are concerned about potential adverse factors that could affect retinal reattachment. For example, during surgeries for proliferative vitreoretinopathy or proliferative diabetic retinopathy, excessive residual blood may lead to postoperative proliferation of epiretinal membranes. Therefore, in our surgical procedures, we introduce only 1 to 2 drops of autologous blood to cover the area of the macular hole. This is considered sufficient to achieve the desired outcome without contributing to the postoperative complications. Fortunately, during the follow-up period, no recurrent retinal detachment nor any membranous proliferation in the macular region was observed in our patients. It is important to recognize, however, that we did not enroll the patients who already had proliferative vitreoretinopathy, extensive pigment dispersion in the vitreous cavity, or associated choroidal detachment, and who showed a significant tendency for membrane proliferation. Our case series is relatively small, and the duration of follow-up is brief, and thus, we did not present long-term results. Indeed, the introduction of autologous blood does add an additional step to the surgical procedure. Consequently, the necessity of incorporating autologous blood into the viscoelastic agent pool technique remains a point of interest and will continue to be a focus in our ongoing research. Another factor is when measuring the diameter of MH using the built-in software of OCT, it is necessary to consider the error caused by the axial length.16 Axial length affects the magnification of OCT images. For longer axial length, the actual size of the macular hole may be underestimated. Owing to this potential error, surgeons might underestimate the difficulty of the operation. The purpose of this correction is to ensure the accuracy of the surgical plan and prognosis evaluation.
However, postoperative BCVA recovery was limited in patients with MHRD. Our surgical approach includes meticulous attention to detail to minimize the impact of surgical steps on postoperative vision: Specifically, to reduce direct contact of indocyanine green with the retinal pigment epithelium exposed at the site of the macular hole, we do not aspirate the subretinal fluid before performing the staining, but instead, we perform it after staining. Similarly, to decrease the harm to the outer retinal cells from breakdown products of blood, autologous blood is restricted to covering only the surface of the ILM flap and is not in direct contact with the retinal pigment epithelium. Some studies have reported that BCVA with MHRD after surgery was related to preoperative visual acuity.17,18 We found that BCVA improvement after MH sealing was not associated with corrected MH diameter, axial length, age, or sex. We attributed our results to the following point: patients with MHRD had atrophic myopic maculopathy in different scales, retinal choroidal and outer retinal layer atrophy should be considered when evaluating the postoperative vision recovery.
In our view, viscoelastic agent pool technology can provide a stable environment, which makes the manipulation of inverted ILM flap more precise and safer. Our preliminary research indicates that no adverse reactions were found, and we believe that viscoelastic agent pool technology is a good complement to the technique of inverted ILM flap in MHRD.
LimitationsThe limitations of this study consist of the lack of a control group and the relatively limited sample size. Future studies should focus on comparing outcomes of this new technique with those of the traditional inverted ILM flap technique. Our research lacks inclusion of patients with macular hole related to rhegmatogenous retinal detachment, a condition that necessitates the use of perfluoron. This requires certain modifications to the viscoelastic agent pool technique. We will also focus on this aspect in our next phase of research. Validation of this technique should be conducted in subsequent research involving bigger sample sizes and extended follow-up durations. Anatomical characterization, including preoperative retinal choroidal atrophy and postoperative outer retinal layer integrity, was not incorporated in the study. In future studies, we aim to consider these parameters and objective indicators (multifocal electroretinography and microperimetry) for assessing macular function posttreatment.
ConclusionWe used the “viscoelastic agent pool” technique to enhance the inverted ILM flap's stability and to reconstruct the roof of the MH. The technique serves as an excellent adjunctive strategy for the inverted ILM flap. The “viscoelastic agent pool” technique was found to be effective in treating MHRD.
AcknowledgmentsThe authors greatly appreciate all the participants and our staff for this study.
References 1. Gao X, Guo J, Meng X, et al. A meta-analysis of vitrectomy with or without internal limiting membrane peeling for macular hole retinal detachment in the highly myopic eyes. BMC Ophthalmol 2016;16:87. 2. Michalewska Z, Michalewski J, Adelman RA, Nawrocki J. Inverted internal limiting membrane flap technique for large macular holes. Ophthalmology 2010;117:2018–2025. 3. Chatziralli I, Machairoudia G, Kazantzis D, et al. Inverted internal limiting membrane flap technique for myopic macular hole: a meta-analysis. Surv Ophthalmol 2021;66:771–780. 4. Lim LS, Tsai A, Wong D, et al. Prognostic factor analysis of vitrectomy for retinal detachment associated with myopic macular holes. Ophthalmology 2014;121:305–310. 5. Huang D, Chopra V, Lu ATH, et al. Does optic nerve head size variation affect circumpapillary retinal nerve fiber layer thickness measurement by optical coherence tomography? Invest Ophthalmol Vis Sci 2012;53:4990–4997. 6. Kang SW, Ahn K, Ham DI. Types of macular hole closure and their clinical implications. The Br J Ophthalmol 2003;87:1015–1019. 7. Wu AL, Ling KP, Lai CC. Management of macular hole retinal detachment. In: Chang A, Mieler WF, Ohji M, eds. Macular Surgery. Singapore: Springer; 2020:271–281. 8. Kaiser PK. Prospective evaluation of visual acuity assessment: a comparison of snellen versus ETDRS charts in clinical practice (an AOS Thesis). Trans Am Ophthalmol Soc 2009;107:311–324. 9. Lai CC, Wu AL, Chou HD, et al. Sub-perfluoro-n-octane injection of ocular viscoelastic device assisted inverted internal limiting membrane flap for macular hole retinal detachment surgery: a novel technique. BMC Ophthalmol 2020;20:116. 10. Yang JM, Kim JG. Internal limiting membrane handling in macular hole surgery: the infusion direction manipulation and infusion off techniques. Eur Rev Med Pharmacol Sci 2022;26:2395–2398. 11. Wang X, Zhu Y, Xu H. Inverted multi-layer internal limiting membrane flap for macular hole retinal detachment in high myopia. Sci Rep 2022;12:10593. 12. Finn AP, Mahmoud TH. Internal limiting membrane retracting door for myopic macular holes. Retina 2019;39:S92–S94. 13. Borkenstein AF, Borkenstein EM, Malyugin B. Ophthalmic viscosurgical devices (OVDs) in challenging cases: a review. Ophthalmol Ther 2021;10:831–843. 14. Grewal DS, Mahmoud TH. Autologous neurosensory retinal free flap for closure of refractory myopic macular holes. JAMA Ophthalmol 2016;134:229–230. 15. Lai CC, Chen YP, Wang NK, et al. Vitrectomy with internal limiting membrane repositioning and autologous blood for macular hole retinal detachment in highly myopic eyes. Ophthalmology 2015;122:1889–1898. 16. Scoles D, Mahmoud TH. Inaccurate measurements confound the study of myopic macular hole. Ophthalmol Retina 2022;6:95–96. 17. Kim SH, Kim HK, Yang JY, et al. Visual recovery after macular hole surgery and related prognostic factors. Korean J Ophthalmol 2018;32:140–146. 18. Lorenzi U, Mehech J, Caporossi T, et al. A retrospective, multicenter study on the management of macular holes without residual internal limiting membrane: the refractory macular hole (ReMaHo) study. Graefes Arch Clin Exp Ophthalmol 2022;260:3837–3845.
留言 (0)