
記住我

Retinal detachment (RD) in pathologic myopia (PM) is commonly caused by a macular hole (MH); it is occasionally associated with posterior paravascular retinal breaks (PRBs).1–3 Treating MHs or PRBs is challenging especially when they are located over the regions of macular atrophy (MA) or patchy chorioretinal atrophy (PCRA). First, it is difficult to identify these MHs or PRBs because there is a lack of contrast due to the underlying chorioretinal atrophy.4 Second, it is difficult to perform laser retinopexy during pars plana vitrectomy (PPV) because the melanin is deficient in the areas of PCRA.4–6 Third, it is difficult to close myopia MH, especially when it is located in the area of MA with a long axial length.7,8
In recent years, a variety of surgical techniques have been used to treat RD associated with MHs and/or posterior PRBs in highly myopic eyes, including PPV combined with an inverted or inserted internal limiting membrane (ILM) technique,9–11 autologous neurosensory retinal transplantation,12,13 and human amniotic membrane transplantation.14–16
For eyes with RD related to MHs situated over MA or posterior PRBs situated over the areas with PCRA, although the autologous neurosensory retinal transplantation is effective, the procedure is complicated and traumatic. The inverted or inserted ILM technique has been shown to improve the closure of MHs or posterior PRBs; however, it is difficult to harvest the ILM flap and ILM plugs in the areas of chorioretinal atrophy. In addition, there is a high risk of ILM fragment dislocation during the gas–perfluorocarbon liquid (PFCL) exchange procedure.
In our previous study, we showed that the autologous blood-assisted lyophilized human amniotic membrane (LhAM) graft covering was simple and effective in treating eyes with MHs in high myopia.17 However, when we used this technique to treat RD eyes with MHs situated over MA or posterior PRBs situated over the area of PCRA, we found that the LhAM was difficult to be placed accurately on the MHs or posterior PRBs in the area of chorioretinal atrophy under gas, and complications such as graft dislocation often occurred postoperatively. Therefore, we modified this surgical technique by using PFCL-assisted pretreated LhAM graft covering to treat these eyes. The grafts were pretreated with indocyanine green (ICG) and hypertonic glucose solution.
In this study, we compared the surgical outcomes of two surgical techniques: autologous blood-assisted LhAM graft covering and PFCL-assisted pretreated LhAM graft covering in treating eyes with RD related to MHs situated over the area of MA and/or posterior PRBs situated over the area of PCRA.
MethodsNineteen consecutive patients with RD related to MHs located above MA or PRBs located above a region of PCRA in PM were included in this study. The patients underwent vitrectomy with LhAM covering between May 2019 and July 2022. The inclusion criteria were as follows: 1) Patients had pathological myopia (>6° diopter (d) or axial length ≥ 26.5 mm) accompanied by posterior staphyloma and myopic maculopathy (Category 3 and Category 4),18 2) patients had RD with MH and/or posterior PRBs situated over the areas of CRA, and 3) patients had proliferative vitreoretinopathy (PVR) A or B. The exclusion criteria were as follows: 1) Patients had RD with MHs or posterior PRBs situated over the areas without CRA; 2) patients had PVR C; or 3) patients had a history of retinal surgery, diabetic retinopathy, vitreous hemorrhage, retinal vascular occlusion, uveitis, trauma, optic atrophy, ocular tumors, or corneal opacity. This study adhered to the tenets of the Declaration of Helsinki. All the patients signed an informed consent. The study protocol was approved by the ethics committee of the Eye Hospital of Wenzhou Medical University (2019-009-K-09).
All patients had standard ophthalmologic examinations including best-corrected visual acuity (BCVA) measurement, slit-lamp examinations, fundus examinations, and spectral domain optical coherence tomography (SPECTRALIS HRA OCT; Heidelberg Engineering, Heidelberg, Germany) before the surgery and during the follow-up period. Axial lengths were measured using intraocular lens Master (Carl Zeiss Meditec AG, Jena, Germany). Briefly, the classification of myopic maculopathy was as follows based on the International Photographic Classification and Grading System: PCRA (Category 3) and MA (Category 4).18 Primary staphylomas were classified as follows according to the area involved: the posterior pole of the eye (Type I), the macular area (Type II), the peripapillary area (Type III), the area nasal to the disk (Type IV), and the area below the disk (Type V).19 The RD was classified as follows based on the extension of RD: type 1 indicated RD within the macula, type 2 indicated RD beyond the macula, and type 3 indicated total RD.9 MH closure was defined as the absence of the neurosensory defect over the fovea on spectral domain optical coherence tomography.20
Information collected from each patient included the patient's age, sex, ocular history, initial BCVA, preoperative and postoperative clinical manifestations, extent of RD, location of retinal breaks, extent of PVR, postoperative complications, and final visual outcomes.
Surgical TechniquePars plana vitrectomy: All eyes underwent 23/25-gauge PPV using the Constellation Vision System (Alcon Laboratories, Inc., Fort Worth, TX). Phacoemulsification was performed before PPV if the fundus was obscured due to the opacity of the lens. The vitreous core was removed by vitrectomy, and the residual vitreous was visualized by injection of 0.05 mL of triamcinolone acetonide aqueous suspension (40 mg/mL suspension, Zhejiang Xianju Pharmaceutical Co, Ltd, China) into the posterior pole. The solution was subsequently removed using a 0.2-µm micropore filter (Millex-GS 0.22 µg, Millipore). If the thin premacular vitreous membrane was adhered to the retina, it was then excised using a vitreous cutter (with controlled suction up to 150 mmHg) or surgical forceps. The ILM was stained with 0.125% ICG for 20 seconds. The ILM was removed completely if ILM was sparse in the macular area and did not fill the MHs or PRBs.
After the MHs or posterior PRBs were identified, the subretinal fluid was extracted using a soft silicone-tipped Flynn needle and gas–fluid exchange. The LhAM graft was cut from the LhAM patch (JiXi RuiJi Bio Technology Co., JiangXi, China) using micro scissors.
The untreated lyophilized human amniotic membrane graft coveringThe LhAM graft was cut approximately 750 to 1,000 µm larger than the size of the MH. During the fluid–air exchange, a small amount of fluid was left in the area of MHs or posterior PRBs (the area of posterior pole). The graft was placed into the vitreous cavity through the trocar using the end-gripping forceps. The sticky stromal side of LhAM needed to face the MH. The fluid left in the posterior pole made the graft unfold and float on the surface of the fluid. The fluid between the graft and the retina was carefully evacuated using a flute needle. The graft was gently adjusted using a flute needle or intraocular forceps to cover the MH or posterior PRB completely. Once the graft was attached to the MH or posterior PRB, one drop of autologous blood was injected to cover the LhAM graft.17
The PFCL-assisted pretreated LhAM graft coveringThe LhAM graft was cut into a size slightly larger than the size of the MH or posterior PRB and then soaked in 0.125% ICG/50% hypertonic glucose solution for 15 to 20 minutes. The graft was rinsed with a balanced saline solution. After the removal of subretinal fluid, PFCL was gently applied over the macula to cover the MH or posterior PRB, and then, the fluid–gas exchange was performed. The vitreous on the periphery was trimmed in all quadrants using scleral indentation. The pretreated graft was implanted into the eye through a 23/25-gauge cannula. The graft sunk into the PFCL and adhered to the surface of the retina, covering the MH or posterior PRB completely. The gas–fluid exchange was performed again, the PFCL was then completely aspirated, and the graft was covered with a drop of autologous blood (see Video, Supplemental Digital Content 1, https://links.lww.com/IAE/C188).
At the end of the surgery, 12% C3F8 or silicone oil (5,700 centistokes) tamponade was performed based on the degree of PVR. The 12% C3F8 tamponade was performed in the eyes with PVR A, and silicone oil tamponade was performed in the eyes with PVR B and the presence of posterior polar retinal proliferative membrane. All patients were asked to remain in the prone position for 2 weeks after the surgery.
The patients were divided into two groups based on the different LhAM graft covering techniques: the untreated group (n = 10, PPV and untreated LhAM graft covering) and the pretreated group (n = 9, PPV and PFCL-assisted pretreated LhAM graft covering).
All statistical analyses were performed using SPSS statistical software (version 20; Chicago, IL). The preoperative and postoperative BCVA values were converted to the logarithm of the minimal angle of resolution (logMAR), as previously described and were analyzed using the Wilcoxon test. Best-corrected visual acuity values of counting fingers, hand movement, and light perception were converted to logMAR values of 1.85, 2.3, and 2.6, respectively.21 Continuous variables are expressed as mean ± SD. The categorical variables are expressed as individual counts and percentages. Univariate analyses were performed using a paired-samples t-test. Statistical significance was considered at a level of P < 0.05.
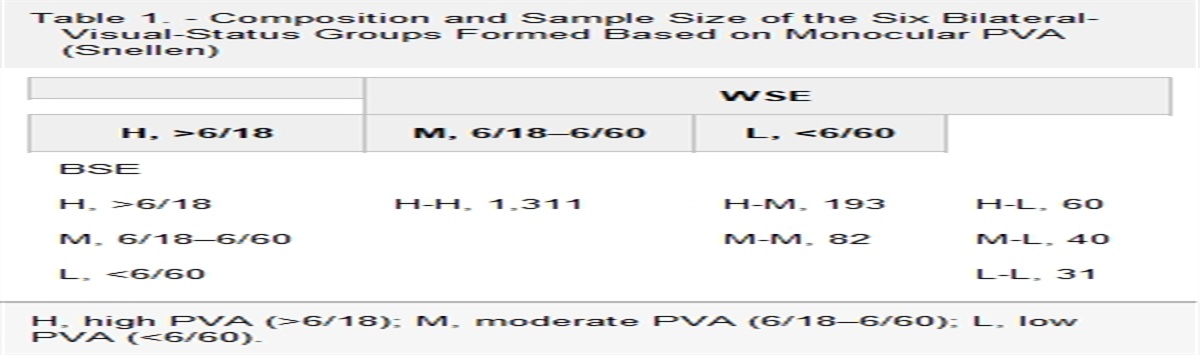
ResultsPreoperative demographic characteristics and postoperative outcomes of patients (14 female patients and 5 male patients) are presented in Tables 1 and 2, respectively. The age was 61.5 ± 11.9 years (mean ± SD, range: 48–84 years) and 62.3 ± 5.5 (range: 54–70 years) in the untreated group and the pretreated group, respectively (P = 0.851). The axial length was 29.7 ± 0.9 mm (range: 28.7–30.9 mm) and 30.8 ± 2.3 mm (range: 26.7–33.5 mm) in the untreated group and the pretreated group, respectively (P = 0.195). Type 1 staphyloma of the posterior pole was present in all eyes in both groups. Macular atrophy was present in 80.0% (8/10) and 77.8% (7/9) of the eyes in the untreated group and the pretreated group, respectively (P = 1.000). Macular holes were found in 90.0% (9/10) and 66.7% (6/9) of the eyes in the untreated group and the pretreated group, respectively (P = 0.303). Paravascular retinal breaks were found in 20.0% (2/10) and 44.4% (4/9) of the eyes in the untreated group and the pretreated group, respectively (P = 0.350). Paravascular retinal breaks and MHs coexisted in one eye and two eyes in the untreated group and the pretreated group, respectively. Patchy chorioretinal atrophy was present in 20.0% (2/10) and 22.2% (2/9) of the eyes in the untreated group and the pretreated group, respectively. The epiretinal membrane was only present in the posterior pole of PVT B. There was no statistical difference in the degree of RD (P = 1.000) or PVR (P = 1.000) between the two groups. Choroidal detachment was only present in one eye in the pretreated group. Suprachoroidal hemorrhage was only found in one eye in the pretreated group.
Table 1. - Preoperative Demographic Characteristics and Postoperative Outcomes of Patients With RD in a PM Eye Case No. Age (y)/Sex/Eye Pathologic Myopic Stats Lens Status Funds Status Retinal Breaks Intervention BCVACat-, cataract; CD, choroidal detachment; CF, counting fingers; Cry-, crystalline lens; EG, excessive gliosis; ERM, epiretinal membrane; F, female; FC, counting fingers; HM, hand motion; IT, inferior temporal to optic nerve; L, left; LP, light perception; M, male; Phaco, phacoemulsification; Pre-op, preoperative; Pse-, pseudophakic; R, right; SCF, suprachoroidal fluid; SCH, suprachoroidal hemorrhage; SiO, silicon oil; ST, superior temporal to optic nerve.
Silicone oil removal was performed 3 to 6 months postoperatively. At the final follow-up (6–24 months), the retinal reattachment rate was 100% in both groups (Table 2).
Postoperatively, the graft covered the retinal surface of MHs and PRBs well in all eyes in the pretreated group. The graft dislocation was found in one eye in the untreated group; the graft shift was found in another eye in the untreated group. No postoperative inflammation was observed in either group. At the final visit, the PRBs were closed in all eyes in both groups. The MH closure rate was 77.8% (7/9) and 100% (7/7) in the untreated group and the pretreated group, respectively (Table 2, Figure 1). Four eyes (40.0%, 4/10) in the untreated group and one eye (11.1%, 1/9) in the pretreated group developed excessive gliosis in the area of MH 6 to 18 weeks postoperatively. The gliosis increased slowly with time and appeared to be stable at the final follow-up (Table 2, Figure 2).
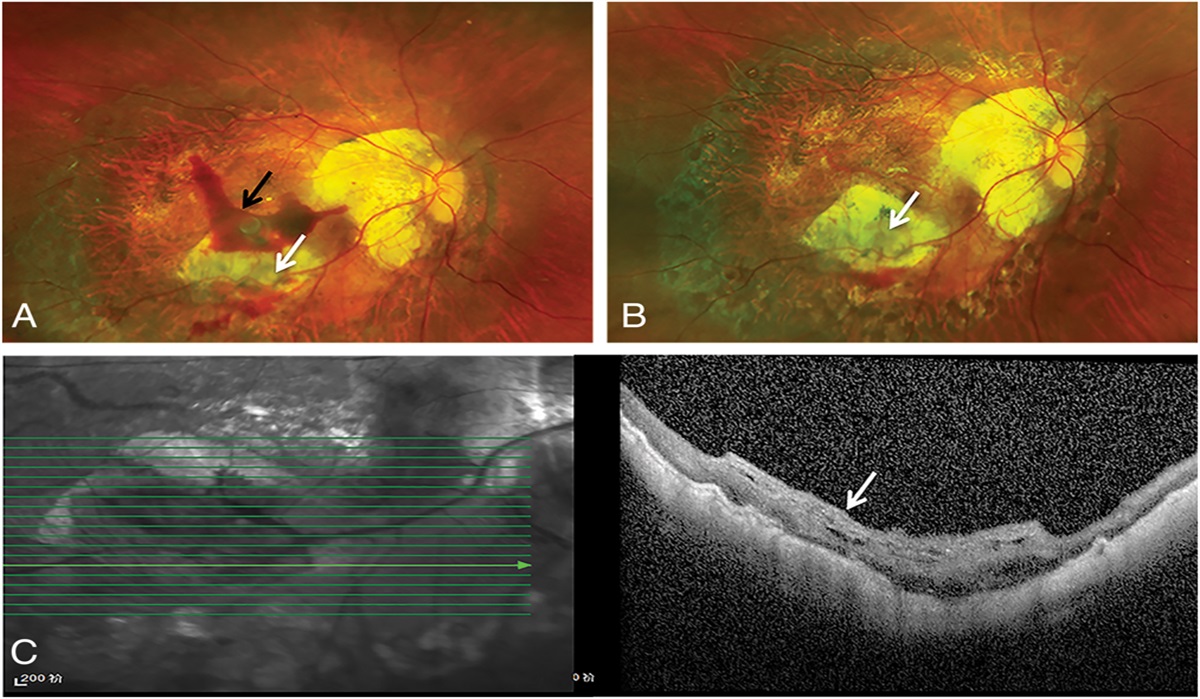
 Fig. 1.:
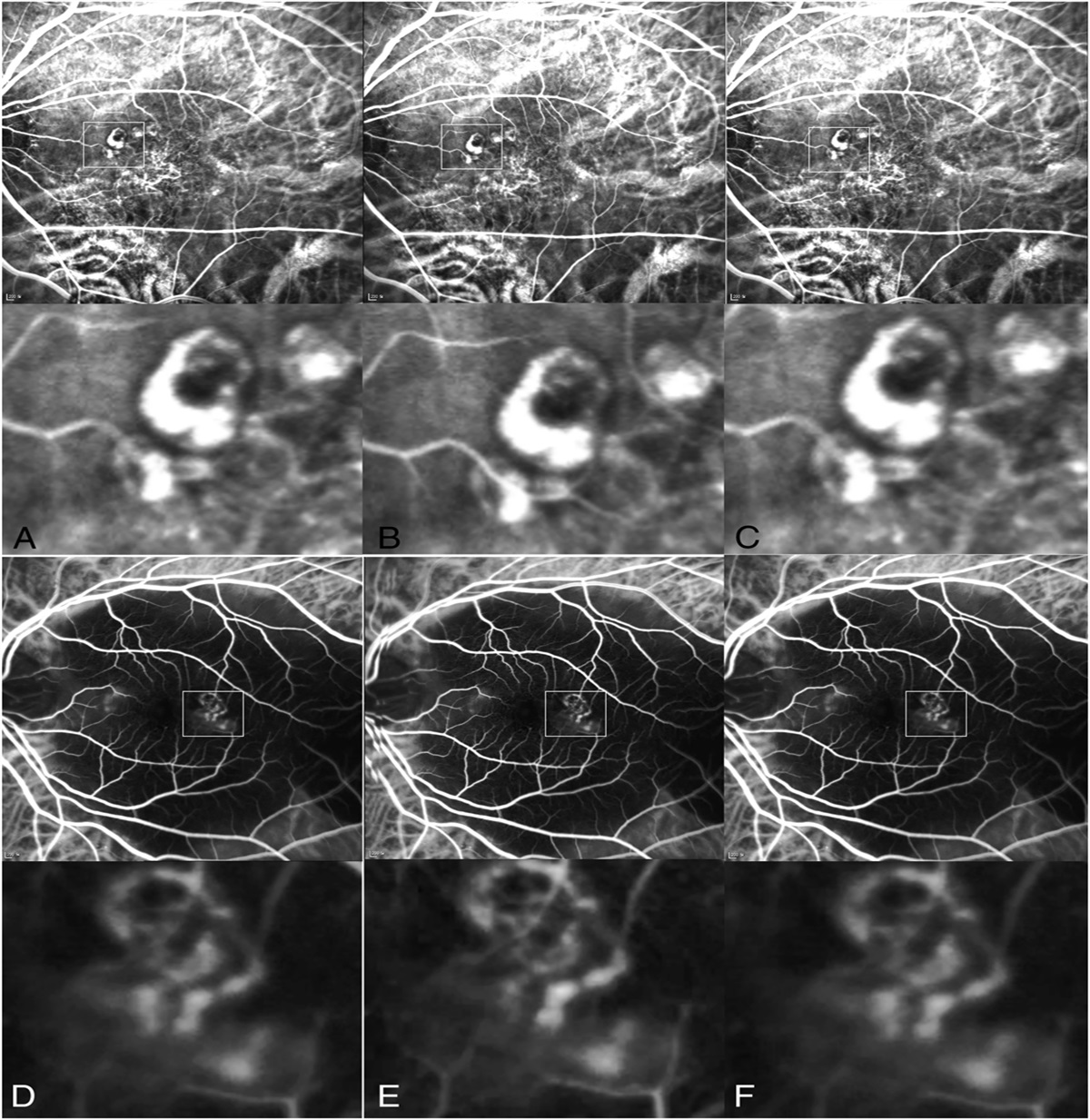
Fig. 1.: The patient (case 12) with RD related to posterior PRBs situated above PCRA in PM underwent a vitrectomy and pretreated LhAM graft covering. A. One week after surgery, the LhAM graft was positioned over the PRBs (white arrow), with a few blood clots visible over the graft (black arrow). B. Three months after surgery, the LhAM graft was attached to the retina (white arrow), and the blood clots have disappeared. C. Three months after surgery, optical coherence tomography showed that the LhAM graft was tightly attached to the retina and the retinal break closed (white arrow).
 Fig. 2.:
Fig. 2.: The patient (case 6) with RD related to MHs situated above MA in PM underwent a vitrectomy and untreated LhAM covering. A. Preoperative optical coherence tomography images showed MH RD (type 1). B. At the 4-week follow-up, optical coherence tomography showed closed MH and uneven LhAM graft. C and D. At the 6-week and 3-month follow-ups, excessive gliosis developed in the macular areas. G and H. At the 13-month and 18-month follow-ups, excessive gliosis remained stable.
Postoperatively, BCVA was improved by more than 0.3 logMAR units in four eyes (40.0%) and seven eyes (77.8%) in the untreated group and the pretreated group, respectively. Best-corrected visual acuity remained unchanged in 60.0% (6/10) and 22.2% (2/9) in the untreated group and untreated group, respectively. At the final visit, the BCVA was improved from 1.8 ± 0.4 logMAR (preoperatively) to 1.6 ± 0.4 logMAR (postoperatively) in the untreated group (P = 0.06). The BCVA was improved from 2.0 ± 0.4 logMAR (preoperatively) to 1.5 ± 0.5 logMAR (postoperatively) in the pretreated group (P = 0.004). There was no statistical difference in the postoperative BCVA between the two groups (P = 0.17, Table 2).
Postoperatively, recurrent suprachoroidal hemorrhage occurred in the eye with preoperative suprachoroidal hemorrhage in the pretreated group; the suprachoroidal hemorrhage was absorbed 1 month postoperatively. Increased intraocular pressure was observed in one eye (10.0%, 1/10) and two eyes (22.2%, 2/9) in the untreated group and the pretreated group, respectively. Multiple anti–glaucomatous medications (1–3) were given to these eyes for the first 2 weeks of the postoperative period.
DiscussionIn this study, we used the PFCL-assisted pretreated LhAM graft (treated with ICG and hypertonic glucose solution) to treat the eyes with RD related to MHs and/or PRBs situated above MA or PCRA in PM. This surgical technique appeared to reduce the dislocation or shift of LHAM graft, promote closures of MHs/PRBs, and reduce gliosis in MH.
The human amniotic membrane plug was first used to promote the closure of recurrent MH17,22 and was later used for treating myopic MHs with RD.14,15 It was also used for repairing RD with PRBs located above PCRA in PM.16 We used the technique to treat myopic MHs with or without RD, and we found that transplanting the LhAM graft through the MH into the subretinal space might lead to enlargement of MH and damage to the photoreceptors and retinal pigment epithelium. This has also been confirmed by other investigators.23 We also found that the LhAM plug might hinder the repair of the outer structure of the retina because it might stay between the retina and the retinal pigment epithelium for a long time.17
In our previous study, we used autologous blood-assisted LhAM graft covering to treat eyes with MH in high myopia and showed that the MH closure rate was 83.3% postoperatively, and the surgical trauma was minimal. This was because the LhAM graft was placed right on the surface of the retina.17 However, when we used this technique to treat RD eyes with MHs situated over MA or posterior PRBs situated over the areas with PCRA, we encountered a lot of problems. First, it was difficult to cover these holes with LhAM graft accurately because the PRBs were often located on the steep slope of the posterior scleral staphyloma. Second, it was hard to tell if the graft was shifted or dislocated at the end of surgery because the contrast between the white LhAM graft and the area of chorioretinal atrophy was low. Third, since the LhAM graft was folded under the air, a small amount of balanced salt solution was required to be left in the posterior pole to open the folded graft.17 The balanced salt solution in the posterior pole may flow into the submacula through MHs or posterior PRBs, making the graft difficult to unfold.
Later, we improved the technique above by using PFCL. Under the PFCL, the location of the MH or PRBs could be clearly identified; however, the untreated LhAM graft tended to float on the surface of PFCL because of its lightweight. Therefore, we pretreated the LhAM graft with a hypertonic sugar solution to increase its gravity, allowing it to sink easily into the PFCL. Once the LhAM grafts touched the retina surface around the MH or PRBs, the basement membrane of the graft could adhere to the surface of the retina under the pressure of PFCL. We also stained the grafts with ICG to make it obviously seen when covering MHs or PRBs. Although ICG is potentially toxic to the retinal pigment epithelium,24 the ICG staining did not affect our patients because their MHs were located in the areas of MA and their PRBs were located over the areas of PCRA.
Recently, postoperative excessive gliosis has been reported in the inverted ILM flap technique.25,26 In this study, higher incidence of excessive gliosis was observed in the untreated group (40%) compared with the pretreated group (11%). Because it is difficult to identify the exact location of the graft under gas, the diameter of the graft in the untreated group is usually larger than the one in the pretreated group. When placing a large graft on the uneven bottom and the steep edge of the posterior scleral staphyloma, it is hard to ensure the smoothness of the graft. Since the pretreated LhAM graft is placed under PFCL, it is easy to identify the exact location of the graft. The pretreated graft is cut into the exact size of the MH or PRB; therefore, it is easy to ensure the flatness of the graft. In addition, there is usually more residual subretinal fluid when placing the untreated graft under the gas. For the pretreated graft, there is almost no residual subretinal fluid under PFCL. The excess residual subretinal fluid may lead to local hyperplasia and excessive gliosis.
Our study has several limitations. First, this is a retrospective study, and the sample size was relatively small. Second, the follow-up period was short, and there was a lack of evaluation of long-term effect.
In summary, PFCL-assisted pretreated LhAM graft (treated with ICG and hypertonic glucose solution) was effective in treating RD related to MHs and/or PRBs situated above MA or PCRA in PM. This surgical technique appeared to reduce the dislocation or shift of LHAM graft, promote closures of MHs/PRBs, and reduce gliosis in MH.
References 1. Morita H, Ideta H, Ito K, et al. Causative factors of retinal detachment in macular holes. Retina 1991;11:281–284. 2. Stirpe M, Michels RG. Retinal detachment in highly myopic eyes due to macular holes and epiretinal traction. Retina 1990;10:113–114. 3. Chen L, Wang K, Esmaili DD, Xu G. Rhegmatogenous retinal detachment due to paravascular linear retinal breaks over patchy chorioretinal atrophy in pathologic myopia. Arch Ophthalmol 2010;128:1551–1554. 4. Hsieh YT, Yang CM. Retinal detachment due to paravascular abnormalities-associated breaks in highly myopic eyes. Eye (Lond) 2019;33:572–579. 5. Lim LS, Tsai A, Wong D, et al. Prognostic factor analysis of vitrectomy for retinal detachment associated with myopic macular holes. Ophthalmology 2014;121:305–310. 6. Lam RF, Lai WW, Cheung BT, et al. Pars plana vitrectomy and perfluoropropane (C3F8) tamponade for retinal detachment due to myopic macular hole: a prognostic factor analysis. Am J Ophthalmol 2006;142:938–944. 7. Wei Y, Wang N, Zu Z, et al. Efficacy of vitrectomy with triamcinolone assistance versus internal limiting membrane peeling for highly myopic macular hole retinal detachment. Retina 2013;33:1151–1157. 8. Suda K, Hangai M, Yoshimura N. Axial length and outcomes of macular hole surgery assessed by spectral-domain optical coherence tomography. Am J Ophthalmol 2011;151:118–127.e1. 9. Lai CC, Chen YP, Wang NK, et al. Vitrectomy with internal limiting membrane repositioning and autologous blood for macular hole retinal detachment in highly myopic eyes. Ophthalmology 2015;122:1889–1898. 10. Baba R, Wakabayashi Y, Umazume K, et al. Efficacy of the inverted internal limiting membrane flap technique with vitrectomy for retinal detachment associated with myopic macular holes. Retina 2017;37:466–471. 11. Rizzo S, Tartaro R, Barca F, et al. Autologous internal limiting membrane fragment transplantation for rhegmatogenous retinal detachment due to paravascular or juxtapapillary retinal breaks over patchy chorioretinal atrophy in pathologic myopia. Retina 2018;38:198–202. 12. Li Y, Li Z, Xu C, et al. Autologous neurosensory retinal transplantation for recurrent macular hole retinal detachment in highly myopic eyes. Acta Ophthalmol 2020;98:e983–e990. 13. Moysidis SN, Koulisis N, Adrean SD, et al. Autologous retinal transplantation for primary and refractory macular holes and macular hole retinal detachments: the global consortium. Ophthalmology 2021;128:672–685. 14. Caporossi T, De Angelis L, Pacini B, et al. A human amniotic membrane plug to manage high myopic macular hole associated with retinal detachment. Acta Ophthalmol 2020;98:e252–e256. 15. Caporossi T, Governatori L, Gambini G, et al. Treatment of recurrent high myopic macular hole associated with retinal detachment using a human amniotic membrane. Jpn J Ophthalmol 2022;66:518–526. 16. Caporossi T, De Angelis L, Pacini B, Rizzo S. Amniotic membrane for retinal detachment due to paravascular retinal breaks over patchy chorioretinal atrophy in pathologic myopia. Eur J Ophthalmol 2020;30:392–395. 17. Chen H, Lin W, Tang Y, Wei Y. The long-term follow-up of autologous blood clot-assisted lyophilized human amniotic membrane covering treatment unclosed macular hole. Retina 2023;43:1340–1347. 18. Ohno-Matsui K, Kawasaki R, Jonas JB, et al. International photographic classification and grading system for myopic maculopathy. Am J Ophthalmol 2015;159:877–883.e7. 19. Curtin BJ. The posterior staphyloma of pathologic myopia. Trans Am Ophthalmol Soc 1977;75:67–86. 20. Chen YP, Chen TL, Yang KR, et al. Treatment of retinal detachment resulting from posterior staphyloma-associated macular hole in highly myopic eyes. Retina 2006;26:25–31. 21. Schulze-Bonsel K, Feltgen N, Burau H, et al. Visual acuities “hand motion” and “counting fingers” can be quantified with the Freiburg visual acuity test. Invest Ophthalmol Vis Sci 2006;47:1236–1240. 22. Rizzo S, Caporossi T, Tartaro R, et al. A human amniotic membrane plug to promote retinal breaks repair and recurrent macular hole closure. Retina 2019;39:S95–S103. 23. Tsai D-C, Huang Y-H, Chen S-J. Parafoveal atrophy after human amniotic membrane graft for macular hole in patients with high myopia. Br J Ophthalmol 2021;105:1002–1010. 24. Stanescu-Segall D, Jackson TL. Vital staining with indocyanine green: a review of the clinical and experimental studies relating to safety. Eye (Lond) 2009;23:504–518. 25. Wu AL, Ling KP, Chuang LH, et al. Treatment of macular hole retinal detachment with macular plug in highly myopic eyes: three-year results. Acta Ophthalmol 2020;98:e839–e847. 26. Chen Y, Wang J, Ye X, et al. The role of internal limiting membrane flap for highly myopic macular hole retinal detachment: improving the closure rate but leading to excessive gliosis. Front Med (Lausanne) 2021;8:812693.
留言 (0)