In this article, we present intermediate results of the initial 5 years of building an integrated patient-centred cardiac care registry alongside the primary processes of the NHR. Although it is complex to establish its impact, several examples have shown demonstrable contributions of a cardiac care registry to quality of care [20, 21].
For most of the facilitated registries comprising over 1.5 million procedures, we showed high percentages of data completeness. The validity of the acquired data is ascertained by the embedded data quality assurance system and the audit process facilitated [13]. Extrapolating the positive trend, it is expected that in the coming years all NHR registries will attain the completeness goals of 95% or 98%. It should be noted, however, that adjustments to quality policies and related mandatory variables required by the NVVC and NVT may impact completeness rates, as centres need time to implement these changes within their electronic medical records in order to prospectively collect the data accordingly.
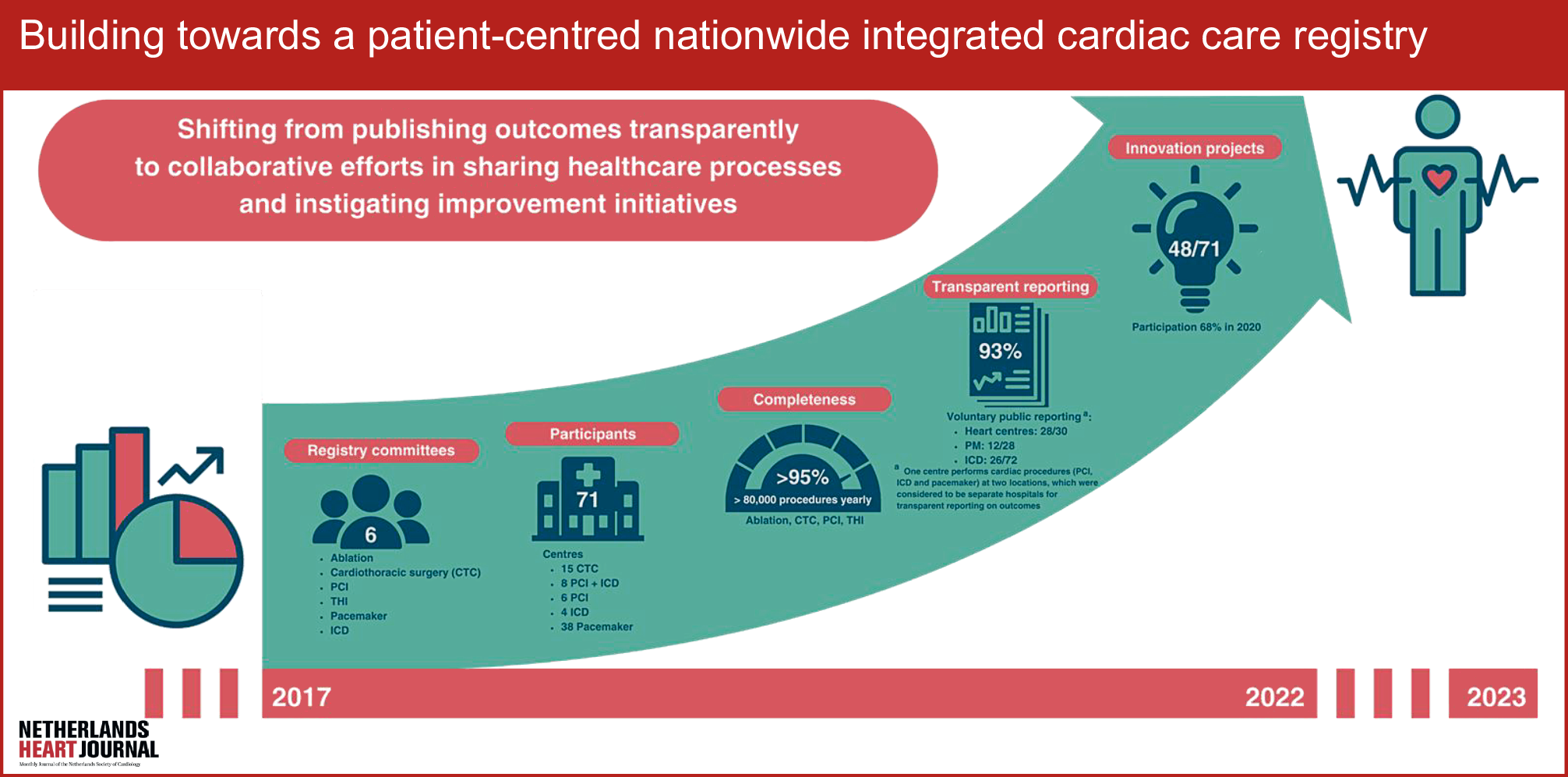
The mandated cardiologists and surgeons actively participate in registration committee meetings, contributing to improvement initiatives and the publication of scientific evaluations. Factors such as physician engagement and availability of complete and accurate data enable reliable benchmark analyses in the public reporting programme [7, 11, 12]. Public reporting may give rise to initiatives for improvement [9, 10]. In the past few years, we have observed in all registration committees a shift from publishing outcomes transparently to collaborative efforts in sharing healthcare processes with the aim of learning and generating ideas on further improving quality of care. This is supported by recent research by the NHR, showing that several centres actively use data and benchmark analyses to determine potential for improvement [22, 23]. In addition, results from several innovation projects initiated by the registration committee, addressing quality concerns such as differences in recovery from phrenic palsy, or gaining additional insights in patients with shock after PCI or in whom an extravascular device is implanted or replaced, have been published [24,25,26]. However, there is still a lot to be gained in this respect. Therefore, the NHR tries to support centres even further by organising meetings and providing a platform for exchanging content and approaches to projects.
In the past 5 years, the merging of cardiology and cardiothoracic surgery registries into the NHR has resulted in substantial progress towards one integrated patient-centred and nationwide cardiac care registry. The bundling of information on all cardiac interventions allows insight into index procedures and re-interventions by means of linking between the registries, enabling follow-up of cardiac patients while lowering the registration burden. Moreover, substantial steps towards a holistic perspective, i.e. the entire pathway of cardiac care, have been taken. The next step will include new registries focusing on medical conditions such as, but not limited to, heart failure, atrial fibrillation, endocarditis and congenital heart diseases. This enables the complete follow-up of patients, including those treated conservatively. The follow-up of these patients may provide relevant insights into guideline adherence and enable the determination of differences in outcomes between all groups of patients. Such insights may benefit physicians and their patients in shared decision-making and choosing wisely between treatment options.
Worldwide, there are several nationwide quality registries focusing on cardiovascular and cardiothoracic procedures, e.g. the GSTCVS registry, which is primarily based on voluntary unaudited survey data [5]. Other quality registries, such as the STS ACSD [27] and NICOR [4], have a multidiscplinary approach and focus on reliable national benchmarking and public reporting of patient-centred outcome measures. This aligns with the principles promoted by the non-profit International Consortium for Health Outcomes Measurement [28, 29]. Meanwhile, within the NHR, a physician-driven plan-do-check-act cycle has been established in the registration committees, initiating the necessary conditions to further build towards an integrated patient-centred cardiac care registry for disease-specific conditions. An example of a quality registry that focuses on specific medical conditions to evaluate the line of care involved is SWEDEHEART [2]. Its setup enables and successfully opens up the potential for registry-based randomised controlled trials (RBRCTs) [30, 31]. This allows SWEDEHEART to serve as an example for the ambitions of and steps taken so far by the NHR regarding the enabling of RBRCTs. Ultimately, clinical registries may become the platform for RBRCTs by utilising real-world data [32, 33].
In the Netherlands, several quality registration organisations exist that cover a variety of medical interventions and conditions. In various forms within these organisations, physicians have a central role in identifying and initiating improvement initiatives [34, 35]. However, the institution of registration committees as organised by the NHR, creating physician-driven registries, is considered unique. In this article we present medium to high participation rates of physicians at meetings of registration committees. The introduction of online meetings, in addition to vis-à-vis sessions, gained momentum due to the COVID-19 pandemic, stimulating and ensuring the continuity of the processes within the registration committee. Hence, a valuable network of involved physicians is continuously facilitated by the structure of the NHR. Physicians’ engagement and their satisfaction are correlated; when the policy and activities of the NHR are deemed relevant, reliable and of high-quality, the results are more likely to be actively discussed. The satisfaction of other stakeholders is additionally high and has shown a positive trend over time.
In conclusion, the NHR is the Dutch platform for registering validated quality data for cardiac procedures and is expanding to facilitate disease-specific quality registries. The data are essential in quality assessment for the NVVC and NVT, thereby contributing to clinical and governmental decision-making. The integration of complete and validated high-quality data, combined with active physician engagement, creates an environment where potential for improvement is identified, and new innovation projects are initiated, effectively supporting quality evaluation and improvement and creating the opportunity to move beyond evaluation of procedural quality to a comprehensive assessment of the patient pathway in cardiac care. Evaluating clinical data and processes should be dynamic and continuously updated and should therefore be one of the cornerstones of quality registries. Identification of essential outcomes is inevitable in updating registry variables and should therefore be published. Finally, the NHR enables re-use of registered data and is therefore suitable to support RBRCTs in the near future.



留言 (0)