Study population
This study was performed at the Medisch Spectrum Twente, Enschede, the Netherlands. Patients were identified by screening the weekly electrophysiology meetings between 1 January 2018 and 1 October 2021. Fourteen patients > 18 years of age with structural heart disease who had PSGB performed for refractory VA were identified. In two patients follow-up was incomplete, as they were transported to a transplantation centre following PSGB, so they were excluded.
Definitions
Sustained VT was defined as having a cycle length < 600 ms with a duration of ≥ 30 s or resulting in either antitachycardia pacing (ATP) or (intracardiac) defibrillation. ES was defined as a cluster of three or more episodes of either sustained VT, ventricular fibrillation or delivery of ATP or an electrical shock by a defibrillator in ≤ 24 h [17, 18]. Structural heart disease was considered to be either a left ventricular ejection fraction of ≤ 50% or the presence of late gadolinium enhancement on cardiac MRI.
Patient selection
Ventricular arrhythmia was treated according to the European Society of Cardiology Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death guideline and the judgement of the treating physician [3]. This generally consisted of antiarrhythmic drugs, sedation and CA when possible. PSGB was considered when VA was refractory to, or not amenable to, the aforementioned treatments. Cases in which PSGB was considered were discussed at our multidisciplinary electrophysiology meeting beforehand. In the case of ES an emergency meeting was scheduled. Only when other options such as CA were not feasible, for example a known inability to approach the substrate or severe comorbidities, was PSGB considered.
Ultrasound-guided PSGB
Percutaneous stellate ganglion block was performed by one of three anaesthesiologists with extensive experience with PSGB for chronic pain syndromes. We decided to perform a left-sided block in all cases. This decision was based on previous studies on LCSD in channelopathies as well as animal research, which suggests that the left stellate ganglion generally innervates a larger portion of the left ventricular myocardium [11, 19,20,21,22,23].
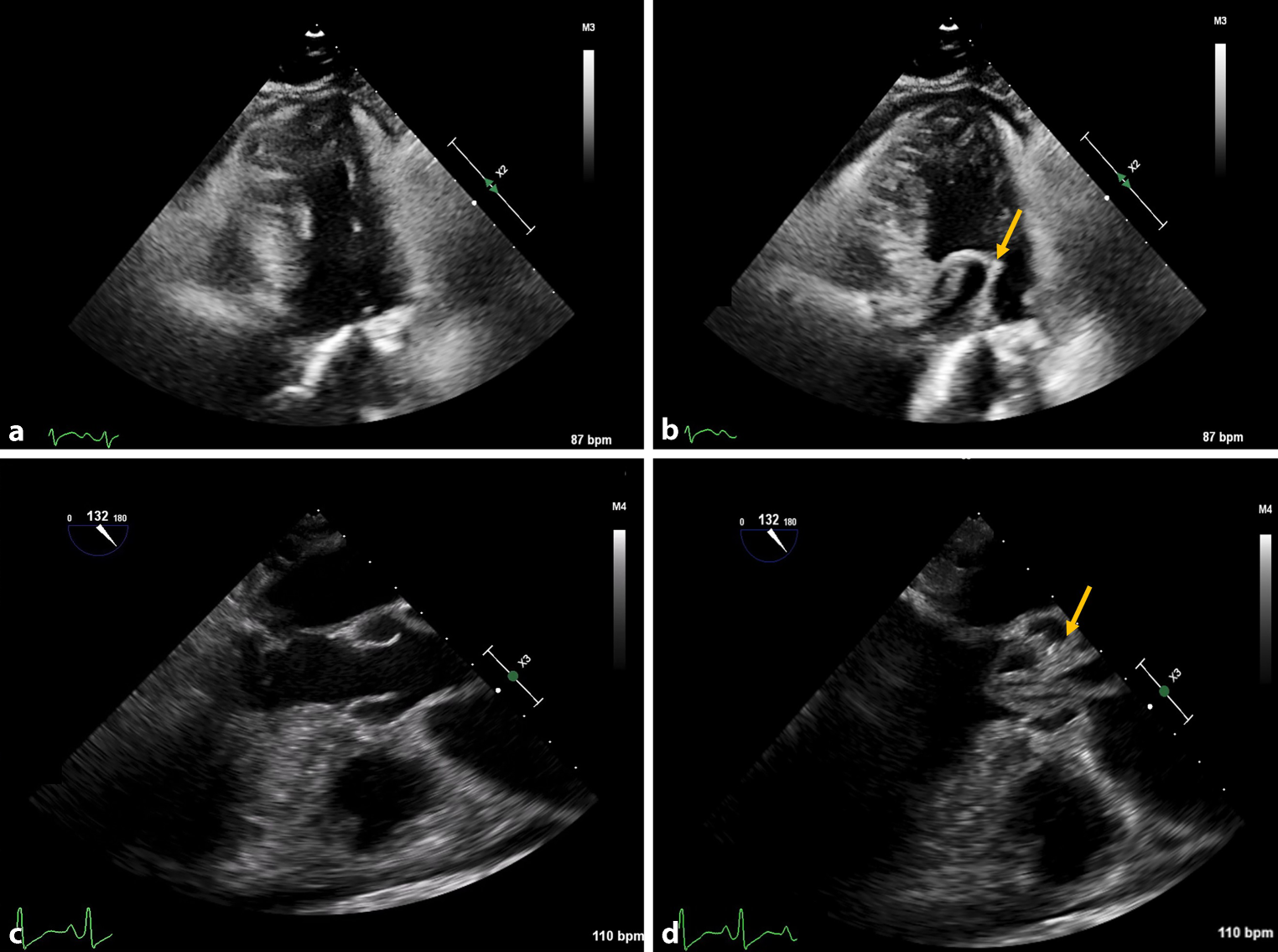
The procedure was performed at the bedside at the Cardiac Care Unit using an ultrasound-guided paratracheal approach. Ultrasound was used to visualise critical structures, including the carotid and vertebral arteries, the left jugular vein, the 6th cervical vertebra, the longus colli muscle and the stellate ganglion, in order to reduce the risk of major vascular complications [24]. Direct oral anticoagulants were discontinued 24 h in advance when possible. An INR of < 2.0 was desired if a vitamin‑K antagonist was administered.
While supine the patient’s head was rotated to the right and a sterile field was created around the neck. After local anaesthesia of the skin a 5-cm echogenic needle (Pajunk, Geisingen, Germany) was inserted in plane from lateral towards medial using the paratracheal approach with a route dorsal to the carotid artery and jugular vein to the stellate ganglion area. An aspiration test was performed and, if negative, the injection was performed. Initially, the type of anaesthetic agent used was determined by the operator. Subsequently, a protocol was implemented whereby 5 ml levobupivacaine 0.25% and 10 mg dexamethasone were used. Dexamethasone is co-administered to shorten the time to onset of the block and to increase the duration for up to 2 weeks [25].
Study endpoints
The primary outcome was the number of times ATP was delivered and the number of ICD shocks or external cardioversions performed for VA in the week before and the week following PSGB. External cardioversions were counted as shocks. This period was chosen to both account for the daily variation in VA episodes as well as PSGB being used as a bridge to a more definitive treatment which would influence the arrhythmia burden. Due to limitations of the patient monitoring system and ICD therapy being disabled in several patients with ES, we were unable to accurately reconstruct the exact onset of VA on the day of PSGB in several cases, and this was therefore not reported. Charts were checked for potential complications, such as local haematoma, paravertebral haematoma, vascular damage, or neurological symptoms.
Statistical analysis
Baseline characteristics (Tab. 1) were evaluated with a mean ± standard deviation being reported. Categorical data are presented as number/total cases (percentage). Event rates before and after PSGB were compared using the Wilcoxon signed rank test. A two-tailed probability value of < 0.05 was considered statistically significant. All statistical analyses were performed with IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA).
Table 1 Patient baseline characteristics (n = 12) 





留言 (0)