Main findings
To our knowledge, this is one of the first studies to examine the impact of SPC on children and young adults who died in a tertiary children’s hospital, with particular attention on ACP. This retrospective analysis compared the periods before and after palliative care implementation and those who received SPC and those who did not. The results demonstrated that patients who received SPC were more likely to have ACP and initiate discussions earlier. Furthermore, patients who received SPC were less likely to receive highly intensive care during the last month of life, including mechanical ventilation, CPR, and dialysis, and more likely to receive opioids.
Initiation of advance care planning
Facilitating ACP is a crucial role of palliative care, providing treatment and care in line with the values and preferences of patients and their families. Early initiation of discussions about the goals of care and routine revisiting of the care plan may improve patients’ and families’ experiences without increasing distress, strain, or emotional burden [17]. We found that patients who received SPC were more likely to engage in ACP, complete medical and legal documents on life-sustaining treatments, and even engage earlier than those who did not. This is meaningful considering the policy in South Korea that limits legal documentation to patients expected to have imminent death, despite the difficulty in clearly defining “imminent death” [18]. This trend to more frequent and earlier ACP was also observed in the post-period than in the pre-period. Our findings are consistent with a previous retrospective cohort study in the U.S., which investigated changes in ACP among children with cancer at the end of life through historical comparisons [19]. Additionally, our study demonstrated an improvement in ACP during the post-period following the implementation of SPC, even in pediatric patients with conditions other than cancer. A possible explanation for this could be that the implementation of SPC within a healthcare institution not only improves the quality of care for patients and families enrolled in SPC but also enhances the culture within the entire institution, allowing a general palliative approach. Our finding of increased opportunities for early ACP among patients with SPC highlights the role of palliative care in setting the goals of care for patients and their families.
Our results showed that ACP would likely be delayed if the patient was an infant. Previous qualitative research of NICU healthcare professionals reported that ACP was challenging owing to the uncertain prognosis of infants and various possible options for advanced medical treatment [20]. Nonetheless, parents found that routine ACP, rather than a startling or desperate event, and standardized psychosocial support helped make end-of-life decisions for high-risk infants [21]. Several factors could facilitate systematic early ACP, including designated personnel, professional awareness, and knowledge of ACP [22]. Further research is needed to address how to standardize ACP for neonates and infants.
Use of intensive care at the end-of-life
Our results showed that patients with SPC received less intensive care such as less mechanical ventilation and CPR, and more opioids during the last month of life. These results were consistent with previous studies indicating higher inpatient service use among children with cancer, yet among them, patients with SPC received less intensive end-of-life care [10, 23]. However, patients with SPC had longer PICU stays and more PICU deaths in the present study, which is inconsistent with previous studies [10]. In conjunction with our findings, recent studies have also presented mixed results regarding the impact of palliative care on end-of-life ICU utilization [24, 25]. Subsequent investigations are required to examine whether these observations indicate goal-concordant care or are influenced by systemic factors, such as the timing of palliative care referrals [25]. Often, reduced use of acute healthcare services, such as fewer hospitalizations, fewer ICU admissions, and more home deaths, are considered quality indicators of hospice and palliative care [26]. Child- and family-centered quality indicators of palliative care should be adopted, regardless of the location of care and/or death, including systematic care planning, expressive therapies [2], encouraging normalcy, and independence for adolescents [27]. Furthermore, our results that ICU deaths were consistent regardless of palliative care involvement emphasize the importance of integrating palliative care into ICU settings.
Palliative care involvement
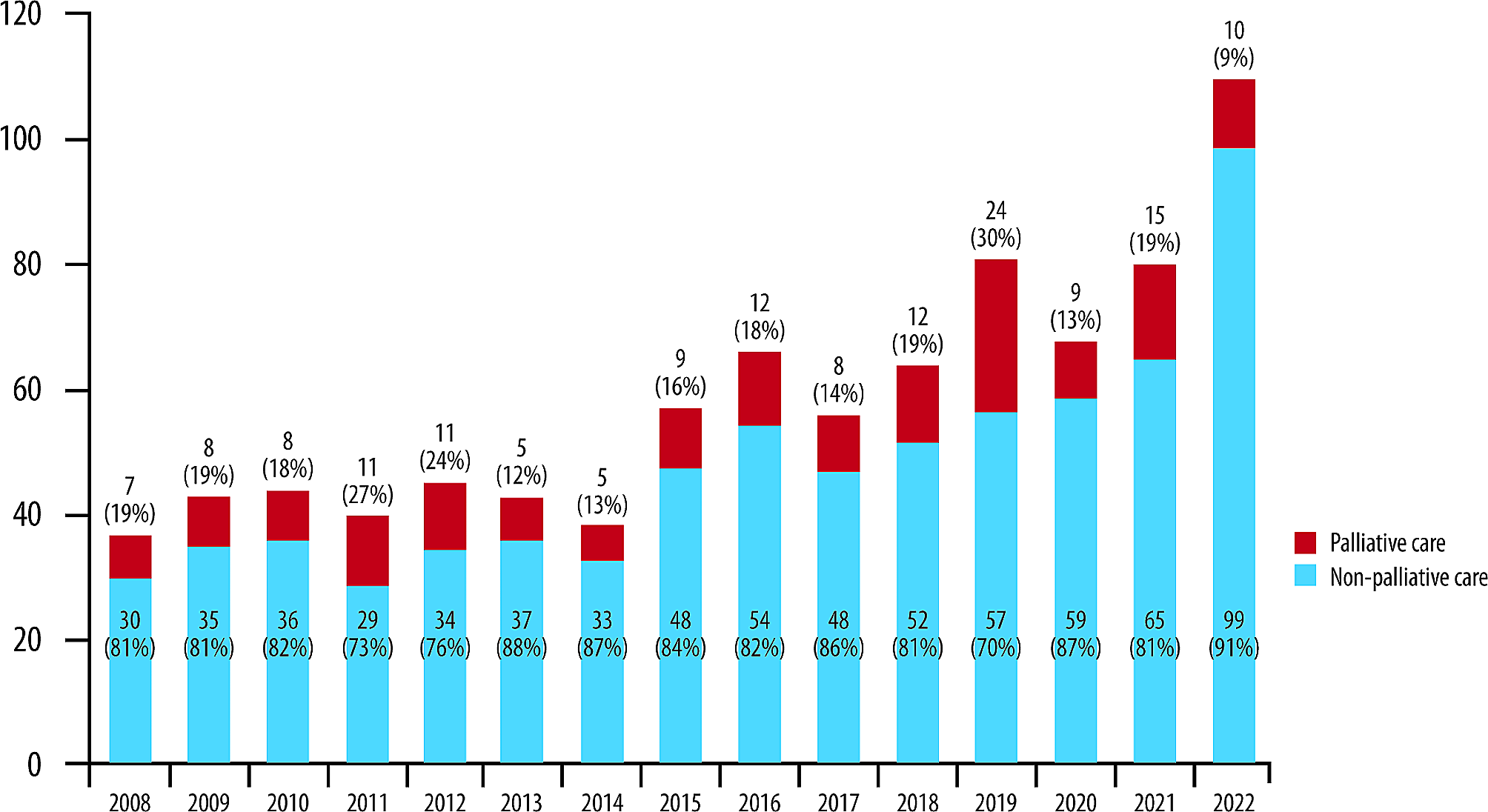
Although it is difficult to directly compare the referral rate owing to the varying roles of the SPC team in patient care, the SPC referral rate of 60% was relatively high within the wide range reported in the previous literature [28, 29]. Rather, the overall involvement of SPC was probably underestimated because patients who were discharged under hospice care or transferred to another children’s hospital before death were not included in our analysis.
This study demonstrated that most children and young adult patients with malignancy received SPC, whereas those with premature and neonatal disease or cardiovascular disease did not. SPC involvement was less common in patients who died in the NICU and in younger patients, which was similar to a previous study [28]. The limited utilization of SPC in the NICU could be attributed to various barriers, including the complex and uncertain nature of the diseases, the lack of education and awareness among healthcare professionals, and the lack of institutional policies [30]. Our findings reveal missed opportunities to integrate palliative care into the NICU, as palliative care for neonates may benefit babies, parents, and healthcare professionals in pain and symptom management, decision-making and collaboration with parents, and psychological support [31].
Strength and weaknesses
This study contributes to our understanding of the demographic and clinical characteristics of children and young adults who died in the hospital across different age groups as well as diverse disease groups. Furthermore, by comparing in-hospital deaths before and after the implementation of SPC, our findings address the impact of SPC on the acculturation of the general palliative approach within the children’s hospital.
This study has some limitations. First, the retrospective nature depends on complete documentation and accurate data retrieval, which makes it vulnerable, as it may depend on the provider and data collection process. However, this study utilized an automatic data-retrieval process to minimize these weaknesses. Second, patients who were cared for at the children’s hospital and died outside the hospital were excluded from the analyses due to limited access to the dataset. In the post-period, 59 patients died outside the hospital while maintaining SPC involvement. Therefore, our study has the potential to underestimate the impact of the SPC intervention on end-of-life healthcare utilization. Further studies are needed to investigate the effect of the SPC on end-of-life care, including deaths outside the hospital, to investigate the complete nature of SPC’s impacts on end-of-life care. Finally, this study investigated a single tertiary children’s hospital, which limits the generalizability of our findings to other institutions in different healthcare contexts. Given the substantial variation in the operations and structures of SPC programs across hospitals [32], the results from the robust SPC program at SNUCH may be challenging to generalize to settings with more limited PPC resources. Further multi-institutional prospective studies are required to validate the results of our study.




留言 (0)