
記住我


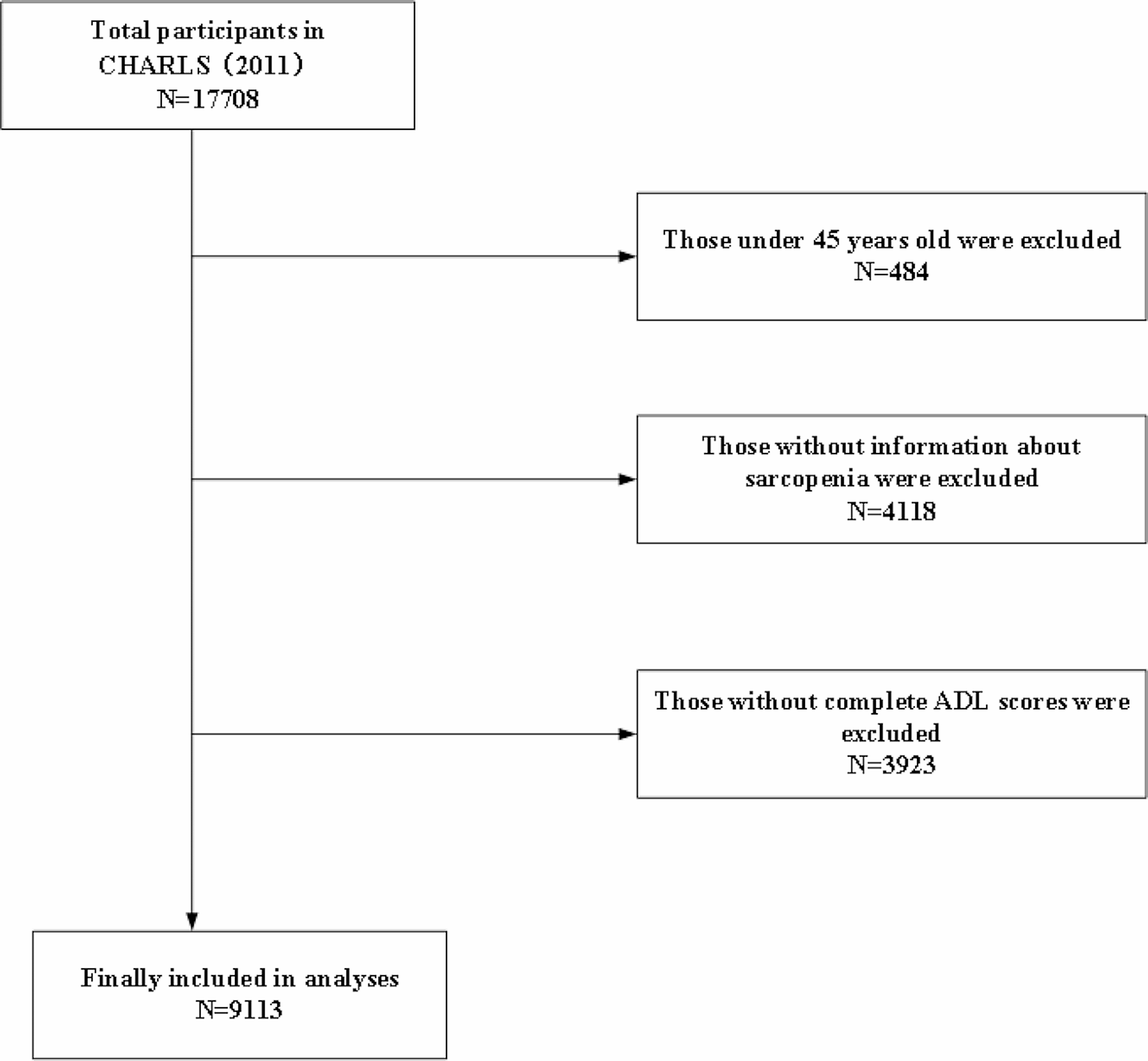
A total of 569 potentially eligible titles and abstracts across databases were screened and after excluding duplicates and those that did not meet this eligibility criteria, included 20 [13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32] studies for data extraction and analysis (Fig. 1).
Fig. 1 Characteristics and quality appraisal of the included studies
Characteristics and quality appraisal of the included studiesOf the 20 included studies, the majority (n = 4; 20%) were from South Africa, and mostly (n = 11; 55%) published between 2012 and 2022. The majority (n = 9, 45%) were cross-sectional studies, and mostly (n = 15; 75%) involved women. The mean quality score ± SD of the 20 included studies was 87% ± 13. All details on the characteristics and quality appraisal of the included studies are provided in Table 2.
Table 2 Characteristics and quality appraisal of the included studies (N = 20)Study findingsTheme 1: physical injuries/trauma due to SGBV occurrence/prevalence, pattern, and associated factorsSeveral studies have explored the prevalence and factors associated with injuries/trauma due to SGBV (Table 3). Ssewanyana et al. highlighted the occurrence of genital trauma among adolescent girls resulting from sexual assault [14]. Apatinga et al. demonstrated that sexual violence was accompanied by physical abuse, leading to physical injuries among women [15]. Azumah et al. reported that visually impaired women who experienced gender-based violence faced a higher risk of injuries including genital injuries [16]. Amashnee et al. identified specific patterns in the occurrence of sexual assault injuries, with higher prevalence on Mondays (28%) and Fridays (27.3%), during specific months, and predominantly during working hours [17]. Abubeker et al. examined the impact of physical violence on female students, with findings indicating various injuries such as bruising, cuts, scratches, and fractures, leading to missed classes and fear of walking alone [19]. Biribawa et al. investigated the burden of GBV-related injuries and found a significant number of hospital visits in Uganda, with slightly declining injury rates (from 13.6 to 13.5 per 10,000 population) from 2012 to 2016 [18]. Umana et al. documented that 6.6% of undergraduate and postgraduate female students experienced sexual intimate partner violence, leading to injuries such as cuts, bruises, and sprains [20]. Mukanangana et al. reported the prevalence of virginal bleeding, genital irritation and urinary tract infection among women in reproductive age in Zimbabwe [21]. These findings collectively underscore the occurrence/prevalence physical injuries/trauma, pattern and specific associated factors associated resulting from SGBV.
Table 3 Physical injuries/trauma due to SGBV occurrence/prevalence, pattern, and associated factorsTheme 2: consequences and impact on mental healthSeveral studies highlighted the significant consequences and impact of SGBV on mental health (Table 4). Ombok et al. found that sexually abused children had a high prevalence (49%) of post-traumatic stress disorder (PTSD), which was associated with the duration of abuse, severity of injuries sustained, parents’ marital status, and family dynamics [13]. Apatinga et al. demonstrated that sexual violence was accompanied by emotional abuse, leading to psychological problems, sexual and reproductive health issues, and suicidal ideations among women [15]. Azumah et al. reported that visually impaired women who experienced gender-based violence faced a higher risk of suicide attempts, and marital breakdown [16]. Liebling et al. found that women and girls who experienced SGBV frequently became pregnant and suffered from injuries, disability, and psychological trauma [22]. Morof et al. highlighted the high prevalence of violence and its association with PTSD symptoms and depression among women [23]. Nguyen et al. demonstrated that exposure to various forms of gender-based violence, including intimate partner violence and sexual harassment, was significantly associated with hypertension, mediated by depression, post-traumatic stress symptoms, and alcohol binge-drinking [24]. Abrahams et al. reported that women raped by intimate partners had higher levels of depressive symptoms compared to those raped by strangers [25]. Pitpitan et al. found a significant association between gender-based violence and increased alcohol use, as well as heightened levels of depressive symptoms and PTSD symptoms [26]. Okunola et al. revealed the complications experienced by survivors of sexual assault, including sexually transmitted infections, depression, and post-traumatic stress disorder [27]. Umana et al. identified the negative impact of violence on academic performance, with victims experiencing loss of concentration, self-confidence, and school absenteeism [20]. Roberts et al. highlighted the association between severe GBV and higher depressive symptoms, PTSD symptoms, disordered alcohol use, and more sex partners [29]. Tantu et al. emphasized the wide range of social, health-related, and psychological consequences resulting from gender-based violence [28]. Finally, Mukanangana et al. revealed that the majority of respondents who experienced rape suffered from psychological trauma, exposure to sexually transmitted infections, unwanted pregnancies, loss of libido, and illegal abortions [21]. These findings collectively demonstrate the significant impact of SGBV on mental health, including psychological trauma, depression, PTSD symptoms, and various adverse outcomes.
Table 4 Consequences and impact on mental healthTheme 3: healthcare access and support servicesThe findings from the studies conducted in the Democratic Republic of the Congo and Togo highlight significant barriers and challenges faced by survivors of SGBV in accessing healthcare and receiving proper psychological care. In the Democratic Republic of the Congo, Scott et al. reported that SGBV survivors faced barriers to accessing healthcare, such as availability and affordability, in their study to evaluate community attitudes of SGBV and health facility capacity to address SGBV in the eastern part of the country [30]. Access to mental health care was difficult [30]. Witch doctors and other traditional healers provided mental health services to some survivors [30]. Burgos-Soto et al.‘s study in Togo, which sought to estimate the prevalence and contributing factors of intimate partner physical and sexual violence among HIV-infected and -uninfected women, found that lifetime prevalence rates of physical and sexual violence were significantly higher among HIV-infected women compared to uninfected women [31]. 42% of the women admitted to ever suffering physical harm as a result of intimate partner abuse [31]. Only one-third of the injured women had ever told the medical professionals the true nature of their injuries, and none had been directed to neighbourhood organizations for the proper psychological care [31].
Theme 4: rural vs. urban disparitiesAccording to a study conducted in Nigeria by Na et al. to identify the trends in sexual assault against women in urban and rural areas of Osun State, completed rapes occurred 10.0% of the time in urban areas and 9.2% of the time in rural areas, while attempted rapes occurred 31.4% of the time in urban areas and 20.0% of the time in rural areas [32]. Rural women were more likely than urban women to endure repeated sexual assault and non-genital injuries [32]. This study findings suggest that sexual assault against women occurs in both urban and rural areas, with notable differences in the patterns and outcomes.
留言 (0)