
記住我


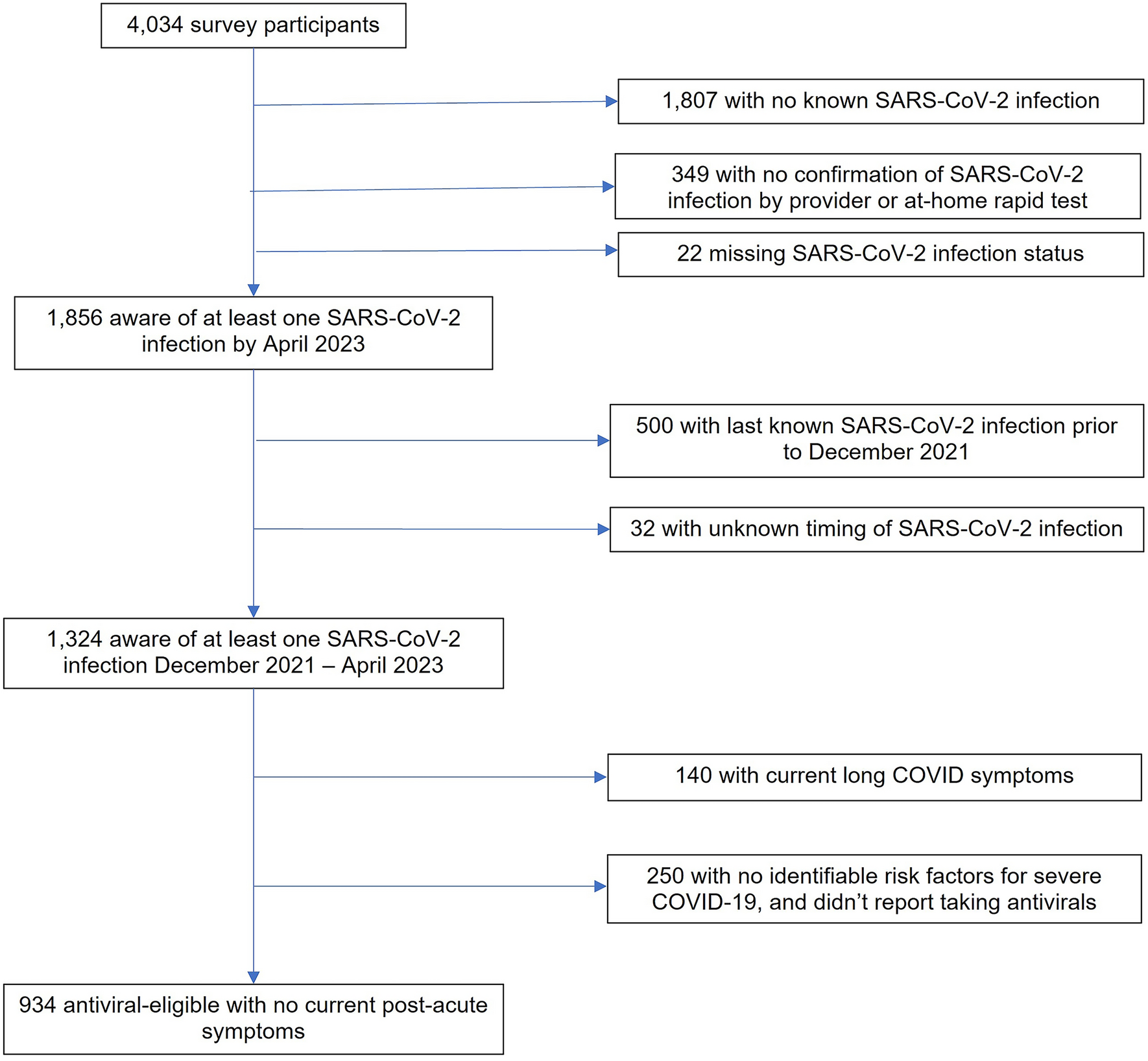
In total, 138 participants from four European countries with complete information in the initial questionnaire were included in the study. Of these, 59 also responded to the follow-up survey. A flow chart of inclusion is shown in Fig. 1. Baseline characteristics for the total set of the study sample and broken down by country can be found in Table 1 and the Supplementary Table S1. In short, most of the participants filling out the questionnaire were mothers (n = 134, 97.1%; fathers n = 3, 2.2%; “other” n = 1, 0.7%), had a median age of 32.5 (range 22–45 years) and had a higher level of education (university degree n = 79, 57.7%). When examining the children affected, 78.3% had an older sibling and half of them were exclusively breastfed until they were hospitalised. Respiratory comorbidities such as previous hyperresponsiveness of the airways, previous bronchiolitis, other previous respiratory diseases (frequent respiratory infections, frequent coughing, abnormal breathing patterns etc.) or previous pneumonia were present in 33.6%, 33.1%, 29.4% and 6.6%, of the surveyed population, respectively. Further pre-existing conditions, e.g. affecting the heart or other organs, were prevalent in 3.6%. In a country comparison, significantly more parents of preterm-born babies showing substantial higher levels of respiratory comorbidities participated from France (Table 1a). Similarly, the compliance with general immunisation recommendations for children displayed significant cross-country variations with France demonstrating the highest willingness to vaccinate (p < 0.001).
Fig. 1
Flow chart of questionnaire respondents
Table 1 Key characteristics of the main study population (n = 138) at time t0RSV Symptoms and Healthcare Resource UtilisationExcept for Italy, most of the RSV cases were diagnosed in hospital and confirmed by test (79.6% and 84.8% of the total population, respectively). The average time spent in hospital was 6 days with 35.5% of the affected children being treated at a neonatal or pediatric intensive care unit. All symptoms related to the RSV infection along with the respective duration reported are displayed in Tables 1b and S1b. Parents across all four participating countries, but in particular evident for France, reported that their children experienced cough, dyspnoea, wheezing and reduced appetite for more than 7 days. Regarding the clinical manifestations of RSV, 76.1% of affected children experienced bronchiolitis with significant differences between countries (p < 0.001) indicating higher occurrence in France and Italy within our study sample. Pneumonia was specified in 19.6% of the patients, with similar rates across all countries. During hospitalisation most of the children were supported by additional oxygen (80.4%).
Parental Worry and FeelingsThe majority of all parents (91%) felt quite or very worried about their child’s overall health status with the occurrence of dyspnoea (fast breathing, retractions of the chest) being the symptom that worried parents the most in all participating countries equally (Table 1c). Further, apnoea (breathing pauses) was also deemed a concerning symptom, particularly reported by German and Swedish parents (p = 0.03).
Several negative emotions related to the child’s health status emerged during the hospitalisation. At country level significant differences were shown, particularly regarding the feeling of guilt towards the separation from other family members at home (e.g. siblings) and the feeling of loneliness with parents from France and Italy being the most impacted (p = 0.001 and p = 0.03 respectively). French participants were also significantly more likely to feel guilty for not having prevented the RSV infection, which was less evident in the remaining countries (p = 0.04).
Parental HRQoL and Family FunctioningThe average scores for the PedsQL FIM measured during the acute infection phase (t0) were as follows: 55.6 for the total score, 52.5 for the parent HRQoL summary score and 59.4 for the family functioning summary score (country-specific results can be found in Table 1d). Across all countries and at the dimension level, “daily activities” emerged as the most impacted aspect relative to the other factors, while “family relationships” demonstrated the highest score. All remaining dimensions differed significantly between the subgroups with the French population consistently exhibiting the lowest scores and participants from Germany and Italy showing relatively higher quality of life (Table 1d).
Loss of Work ProductivityWhile the majority of the population surveyed was (still) on parental leave (55.5%), 31.3% stated that they were full-time or part-time employed with a median of 35 working hours per week at time t0. Of these, 40.5% indicated that their job productivity was “very much” influenced by the RSV-induced hospitalisation of their child. Between the outbreak of the disease until the completion of the initial survey, parents reported missing an average of 29 working hours. Additional barriers when visiting the child in hospital such as additional costs, conflicts with the care of siblings or other family members and long distance were reported by 30.2%, 25.6% and 20.9% of the working population respectively. German and Italian participants were thereby significantly more affected by overlaps in care as compared to France and Sweden (p = 0.008; Table 1e).
RSV Awareness and Support StructuresAbout one-quarter (21.7%) of the population surveyed had not been aware of RSV and its possible complications for the child prior to this hospitalisation. Moreover, 48.6% reported that they were not aware of the consequences for the whole family, 28.3% lacked the information about measures for preventing RSV and 24.8% did not know where to find support for managing mental health problems like stress during this period. On country level, participants from France and Sweden showed significantly higher levels of disease awareness and knowledge of prevention measures as compared to Germany and Italy (Table 1f).
Before discharge from hospital, 40% of the participants did not receive any information or did not feel adequately informed about how to protect the child (and their family) from reinfection with the virus. Similarly, 71.1% stated that during the child’s hospitalisation no or no adequate information about mental health support was offered. Significant cross-country differences were shown in both categories with Germany offering the fewest support structures (p < 0.001 and p = 0.025 respectively).
Overall Burden of Families During Acute Infection Phase and 6 Weeks Later (Follow-up)Fifty-nine participants of the total set (n = 138) also responded to the follow-up survey (t1) which was carried out about 6 weeks after completion of the initial questionnaire (t0). Across all countries RSV-related symptoms of cough, reduced appetite, wheezing and dyspnoea were still present for more than 7 days in 55.9%, 22.0%, 16.9% and 15.3% of the affected children, respectively, with 32.2% of the parents still feeling quite or very worried about their child’s overall health status.
When examining the overall burden of the surveyed population, significant differences were shown in the subjectively perceived general health before, during and after the child’s RSV-induced hospitalisation with parents demonstrating the worst scores at the time of the acute infection phase (p < 0.001; Fig. 2). Comparing PedsQL FIM results at time t0 and t1, participants reported a significant improvement in the total score (t(58) = 4.13, p < 0.001, d = 0.54), the parent HRQoL summary score (t(58) = 5.13, p < 0.001, d = 0.67) and the family functioning summary score (t(58) = 2.56, p = 0.007, d = 0.33) 6 weeks after the acute infection phase (Table 2 and Fig. 3). According to Cohen, these effects were medium for both quality-of-life summary scores and small for the family functioning summary score. At subscale level, caregivers of RSV-infected children showed no significant differences from t0 to t1 for “cognitive functioning,” “communication” and “family relationships”, while the remaining dimensions—similar to the three sum scores—demonstrated significantly higher scores at the time of the follow-up survey.
Fig. 2
Subjectively perceived general health from 10 (excellent) to 1 (very bad) for each participant before, during and approximately 6 weeks after the RSV infection (n = 58)
Table 2 Key characteristics of the main study population 6 weeks after the acute infection phase (t1, follow-up survey)Fig. 3
Country-specific PedsQL FIM sum scores at t0 and t1. The shape of each violin plot represents the density estimate of each variable. The line dividing the box in each violin plot into two parts represents the median of the data. The ends of the box show the upper (Q3) and lower (Q1) quartiles
Overall, 27.1% of the caregivers stated that the child’s hospitalisation for RSV is still affecting them “often” or “always” 6 weeks after the acute infection phase. Also, 20% of the employed participants who conducted the follow-up survey reported a lasting impact on their job productivity with an average of 13.5 missed working hours since the child’s discharge from hospital. No major country-differences were identified in the results of the follow-up survey (Table 2).
留言 (0)