
記住我








Ebstein's anomaly (EA) is a rare complex congenital heart disease with variable malformations occurring in one per 200,000 live births and accounting for <1% of all cases of congenital heart disease.[1] Downward displacement of tricuspid leaflets, tricuspid valve regurgitation, and the atrialized right ventricle, as well as complicated malformation are the main pathological changes in EA. Due to the wide pathological variation of EA, a range of surgical techniques have been employed with variable outcomes.[2–7] Therefore, it would be valuable to better define the indications for specific surgical management strategies.[7]
In this paper, we reviewed our experience concerning patients who underwent surgical correction of EA and reported that the excellent results can be achieved based on pathological changes of the patients by choosing individualized management strategies, operative principles, and surgical techniques.
Methods PatientsThis retrospective study reported the patients who underwent EA surgery performed by the same surgeon at The First Hospital of Tsinghua University from March 2004 to January 2020. The Research Ethics Committee of First Hospital of Tsinghua University approved the study (No.HX200403-022). Informed consent was obtained from all patients or family members.
The diagnosis of all patients was made by ultrasonic cardiography (UCG), chest X-ray, electrocardiography (ECG), computed tomography (CT) scan, and magnetic resonance imaging (MRI,in some patients) and was confirmed intraoperatively. All operations were performed through sternotomy under cardiopulmonary bypass (CPB) with hypothermia and a right-angled cannula was used for cannulation of superior vena cava.
Intraoperative transesophageal echocardiography (TEE) was used to monitor cardiac and valvular function during the operation.
Operative techniquesThe surgical techniques of anatomic correction consist of the following steps:
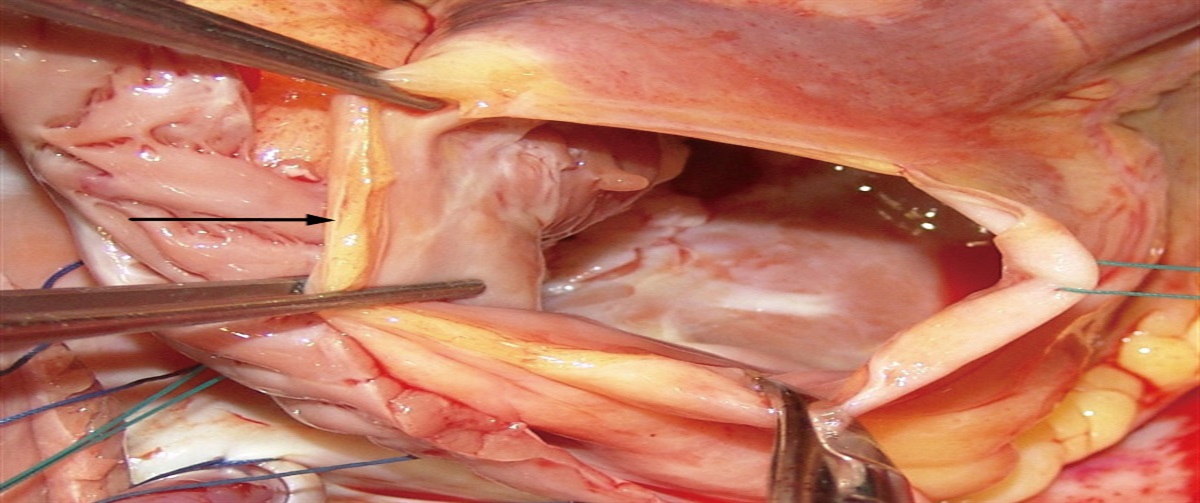
First, management of atrialized right ventricle. The size and location of atrialized right ventricle vary considerably. The atrialized right ventricle is located above the attachment of downward displaced leaflets and below the true tricuspid valve annulus. In some patients, if the anterior leaflet is the only downward displaced leaflet, then the atrialized right ventricle will be located anterior to the right ventricle. The atrialized right ventricle may extend to the left of the posterior descending branch of coronary artery. The wall of the atrialized ventricle is thin, with hypoplastic myocardial tissue or myocardium being replaced by adipose metaplasia [Figure 1], which may impair right ventricular function. We consider that the length is relevant to cardiac function of the atrialized ventricle since the shape of the atrialized ventricle is irregular; if the length is greater than 3 cm, we will excise the redundant portion in the shape of a trapezoid or triangle. If the length is less than 3 cm and the thickness of the wall is greater than 1.5 mm, we will retain the myocardium, and the cut edges are sutured together with continuous 4/0 or 5/0 prolene (Ethicon, Somerville, NJ, USA) longitudinally. As a result, the atrialized ventricular wall remains, containing the coronary artery with a strip of muscle.
 Figure 1:
Figure 1: The cut edge of a thin-walled atrialized RV reveals the absence of myocardial tissue that is replaced by adipose tissue. The black arrow shows myocardium replaced by adipose metaplasia. RV: Right ventricle.
Second, reconstruction of tricuspid valve. The operation is to fully release the downward displaced valve leaflets with residual chordae tendineae and abnormal papillary muscles, and then completely detach it from the annulus and ventricular wall. Normal leaflets, chordate, and papillary muscles must always be retained in their position and never be detached, which is significantly different from other techniques. The tricuspid valve should be reconstructed using as much autologous tissue as possible. If the leaflet surface area is insufficient, a segment of detached abnormal leaflet can be used to enlarge it [Figure 2], or if local leaflet tissue is insufficient, a freshly prepared autologous pericardial graft can be fashioned as the "new leaflet"; it is then to be reattached at the normal level of the tricuspid annulus. Chordae tendineae and papillary muscles can also be reconstructed by incorporating autologous tissue such as abnormal muscles or leaflet. Gore-tex® (W.L. Gore & Associates, Inc, Flagstaff, Ariz) artificial chordae can also be used, which can be transferred and sutured to the free edge of a segment of pericardium or to reconstructed valvular leaflets. With adequately sized posterior and septal leaflets, the detached leaflets may be reattached to the plicated anulus, and the papillary muscles re-implanted in mechanically appropriate positions. When reconstructing the septal leaflet, it is advised to suture the base of the leaflet to a point of 0.8–1.0 cm below the membranous septum to avoid damaging the conduction bundle. We found that almost all patients could avoid complete atrio-ventricular block by use of this technique.
 Figure 2:
Figure 2: Two pieces of rudimentary valvular tissue have been sutured to increase the surface area of one leaflet. The black arrow shows the suture line.
Third, plication of tricuspid valve annulus. Enlarged tricuspid valve annulus is one of the major causes of regurgitation in EA patients. Therefore, the tricuspid annulus was plicated (annuloplasty) in all patients after the atrialized right ventricle portion was excised, achieved by running a 4/0 Prolene® (Ethicon, Inc., Somerville, NJ, USA) suture in the enlarged anteroposterior commissure. We avoided the use of rigid rings in children because stenosis may occur during growth. Annulus circumference was determined based on predicted tricuspid valve size according to patient body surface area to avoid stenosis. The risk of suture line avulsion following annulus plication of dilated tricuspid valve is significant due to large hoop stresses. Reliable suture-lines are essential.
Fourth, plasty of enlarged right atrium. Patients with EA usually have an enlarged right atrium and thick atrial wall, and a normal sized atrium can easily be achieved by trimming and excision of redundant anterior right atrial wall.
Fifth, deal with complicated malformations.
Sixth, reoperation. Reoperation should be performed in time when the patients experienced severe operative complications.
Seventh, intraoperative assessment of valve and cardiac function. Before weaning from CPB, we inspected directly the function of the valves and right ventricle with the heart beating and ECG changes. We temporarily closed the right atrium if necessary and checked the function of the valves and right ventricle by TEE. TEE was routinely used for observing which was very helpful. In cases of abnormal valve function or ECG, we recommend to start CPB again and correct the remained abnormality; for example, in right ventricle with low cardiac output, despite pharmacological intervention, a Glenn shunt procedure would be added.
Statistical analysesContinuous variables were expressed as mean ± standard deviation, while categorical variables were shown as number (percentage). A t-test was used to compare the statistical differences between values such as New York Heart Association (NYHA) functional class and severity of tricuspid valve insufficiency at baseline and various time points. A P-value of <0.05 was considered statistically significant. Cumulative survival rates and reoperation-free survival were analyzed according to Kaplan–Meier estimates. All statistical analyses were performed using STATA 16.0 software (Stata Corp LLC, College Station, TX, USA).
Results PatientsBetween March 2004 and January 2020, 253 patients with EA, including 145 (57.3%) females and 108 (42.7%) males, underwent 258 surgical corrections. Patients were aged 3 months to 64 years and weighted 3.0–88.6 kg [Table 1]. There are 33 patients aged less than 3 years and 80 aged 4–14 years. All patients have symptoms at baseline. 199 patients had cardiac malformation, such as atrial septal defect (ASD), patent ductus arteriosus (PDA), partial endocardium cushion defect (PECD), complete transposition of great artery (c-TGA), and right ventricular outflow tract obstruction (RVOTO) [Table 2]. A total of 32 patients accepted previous surgery, of which 14 patients received Danielson procedure in other hospitals [Table 3].
Table 1 - Baseline data of patients with EA. Characteristics Values (n = 253) Age (years) 19.4 ± 16.7 (3 months–64 years) Female 145 (57.3) Weight (kg) 45.4 ± 21.5 (3.0–88.6) Cyanosis 42 (16.6) Palpitation 123 (48.6) Exercise intolerance 253 (100.0)Data are expressed as n (%), or mean ± standard deviation (range). EA: Ebstein's anomaly.
ASD: Atrial septal defect; AVB: Atrioventricular block; c-TGA: Complete transposition of great artery; EA: Ebstein's anomaly; MI: Mitral valve insufficiency; PDA: Patent ductus atrial; PECD: Partial endocardium cushion defect; PFO: Patent foramen ovale; RBBB: Right bundle branch block; RVOTO: Right ventricular outflow tract obstruction; VSD: Ventricular septal defect; W–P–W syndrome: Wolff–Parkinson–White syndrome.
ASD: Atrial septal defect; EA: Ebstein's anomaly; VSD: Ventricular septal defect.
Anatomical correction was performed in 203 (78.7%) operations. Among them, 131 operations (50.8%) had autologous pericardial graft due to limited availability of leaflet material. 1½ ventricle repair was performed in 38 (14.7%) operations, tricuspid valve repair only in 4 operations (1.6%), tricuspid valve replacement in 10 operations (3.9%), total cavopulmonary connection (TCPC) in 2 (0.8%), and Glenn operation in one operation (0.4%). Five patients died with an early mortality rate of 2.0%. Complete atrioventricular conduction block was complicated in one patient (0.4%).
Surgery for complex cardiac malformations was performed in 202/253 (79.8%) patients [Table 2]. ASD or patent foramen ovale (PFO) were closed in 153 and 8 patients, respectively; double switch operation for corrected transposition of great arteries was performed in one patient; ligation of patent ductus arteriosus in 8 patients and resection of the abnormal muscles to widen right ventricle outflow tract stenosis in 18 patients. Kent bundle was interrupted for Wolff–Parkinson–White syndrome (W–P–W) preexcitation syndrome after radiofrequency ablation failed in three patients, and partial atrium ventricle septal defect canal with mitral valve regurgitation was concomitantly repaired in three patients.
Pathological featuresA total of 221 patients underwent their first open-heart surgery in our center, and a large variety of pathological changes were found including leaflet absence. Atrialized ventricle was found in 190 patients (86.0%) with irregular geometry. The wall of the atrialized portion of right ventricle (RV) was very thin and myocardial muscle tissue was replaced by adipose tissue in some patients. Rarely, the atrialized portion appeared as a large aneurysm, which was located anterior to the right ventricle in seven patients [Figure 3].
 Figure 3:
Figure 3: A huge atrialized RV is located anterior to the RV. (a) Aorta; (b) Atrialized RV. RV: Right ventricle.
The degree of downward displacement and abnormal sub-valvular apparatus of tricuspid valve was highly variable [Figure 4], ranging from valve leaflets' absence, as indicated in Figure 5, to normal, which caused moderate to severe tricuspid valve insufficiency. Sub-valvular apparatus was also abnormal in most patients. There was no chordae tendineae at the free margin of anterior leaflets in some patients. Sixty two out of 221 patients had normal anterior leaflets. One hundred and fifty nine patients had anterior leaflets downwards displacement. Nine patients had normal septal leaflets, one hundred and fifty eight patients had septal leaflets downwards displacement, and 54 patients had septal leaflets absence. Thirteen patients had normal posterior leaflets, 138 patients had posterior leaflets downwards displacement, and 70 patients had posterior leaflets absence. This is much different from the literature reports.[8] A total of 199 patients had other malformation. 33 patients had arrhythmia including W–P–W syndrome, atrial fibrillation, and III˚ AVB [Table 2].
 Figure 4:
Figure 4: (A) Anterior leaflet is normal. (B) Anterior leaflet downward displaced was seen in the posterior half of the leaflet. (C, D) Anterior leaflets downward displacement and severe dysplasia. The dotted line is the position of normal annulus.
 Figure 5:
Figure 5: Septal leaflet is absent (a) and ASD (b). ASD: Atrial septal defect.
According to the Carpentier's classification,[9] 47/221 (21.3%) patients were of types A or B, 108/221 (48.9%) patients were of type C, and 56/221 (25.3%) patients were of type D. Ten out of 221 (4.5%) patients were beyond the classification, including seven isolated anterior leaflet downward displacement and three patients without anterior leaflets. All patients had moderate to severe tricuspid valve regurgitation. Based on what we found in the surgery, the anterior leaflet is related to the severity of the disease. In order to verify our observation, we divided the pathological changes of EA into three types: type I, anterior leaflet attached at normal position [Figure 4A], including 62 patients; type II, anterior leaflet downward displacement in the posterior part of the leaflet (less than half affected) [Figure 4B], including 83 patients; and type III, anterior leaflet downward displacement in the posterior part of the leaflet (more than half affected) with complex severe hypoplasia [Figures 4C,D] or absent, including 76 patients. From our experience, the pathological changes in types I and II patients can be corrected completely. However, for the type III patients, 1½ ventricle repair or other procedures may be a better choice. In this series of patients, the anatomical correction, which means reconstruction of tricuspid valve and right ventricle, was performed in 202/253 (79.8%) individuals among the types I and II patients.
Outcomes of operationsA total of five patients died in the postoperative period (four of them died from low cardiac output syndrome and one from lung infection). The early mortality rate was 2.0%. A–V block occurred in one patient (0.4%).
During the operations, TEE confirmed tricuspid competence in 230 patients and mild incompetence in 23 patients. The mean grade of tricuspid valve regurgitation improved from 3.6 to 1.5 (P <0.01) in 253 patients. No patient had tricuspid valve stenosis. The mean class of cardiac function (NYHA) recovered significantly from 3.5 to 1.1 (P <0.01) by the time of patient discharge.
Chest echocardiography showed that heart size significantly decreased, the atrialized chamber had been obliterated, and tricuspid valve leaflets were located at a normal annular level. These findings were maintained during the follow-up period.
Four patients were lost to follow up. The duration of follow-up for 244 patients was 3.0–168.0 (mean 87.6 ± 38.4) months and annually thereafter, the follow up of which consisted of ECG, X-ray, UCG, and documentation of any adverse events, including death. Three patients died after one year: one patient died from sudden death after tricuspid mechanical valve replacement; one died from an accident; and one died from hemoptysis seven years after TCPC procedure. The survival rates at five and ten years were 98.6% and 98.2%, respectively [Figure 6A].
 Figure 6:
Figure 6: Kaplan–Meier curves with 95% CI showing (A) survival rate, (B) freedom from TR recurrence, and (C) freedom from reoperation.
Recurrence of tricuspid valvular insufficiency was moderate in 13/244 (5.3%) patients and severe in 4/244 (1.6%) patients. The Kaplan–Meier curve of freedom of moderate tricuspid valvular regurgitation is shown in Figure 6B. Reoperation was performed in five patients (2.0%) in this group [Figure 6C]: tricuspid valve replacement was done in one patient, 1½ ventricle repair in two patients, and tricuspid valve annulus reinforced in two patients.
DiscussionPatients with obvious symptoms, moderate or severe tricuspid regurgitation, and a cardiothoracic ratio >0.55 should be considered for operation. In cases where patients are asymptomatic and there are no notable changes in heart size, a continued follow-up is recommended, particularly for younger patients, as tricuspid valve insufficiency could potentially recur post-operation. However, individuals experiencing heart failure should undergo surgery promptly.
Anatomic correction may be the best option for the patients with EA. All associated abnormalities in EA patients should be corrected simultaneously, such as repairing ASD, VSD and ligation of PDA. Double switch procedure for EA patients associated with c-TGA is the best choice. Patients with W–P–W syndrome can be treated surgically by cutting off the Kent bundle simultaneously. Because the results of tricuspid valve replacement are poor, particularly when mechanical valves are used, artificial tricuspid valve replacement should be avoided if possible,[10] the same as the 1½ ventricular repair,[11] total cavopulmonary connection (TCPC), and some other procedures.
In line with other complex congenital heart diseases, biventricular repair technique should be always preferred for patients with EA. The severity of the patient's malformation is the most important factor affecting the outcome of the operation. The strategy, surgical principles and techniques for patients with EA should be individualized. By reference to the normal right ventricle and tricuspid valve anatomy, anatomical correction procedure was performed to correct all abnormality of the tricuspid valve and right ventricle including enlarged right atrium, as we have previously reported.[12–14] This is significantly different from the report by others.[5,9,15–16] Considering long-term results and recurrence of tricuspid valve regurgitation, the first operation have to be postponed and performed properly to ensure durability of the new tricuspid valve with respect to life expectancy and childhood growth. Also, close long-term follow-up is necessary after surgery.
Downward displacement of tricuspid valvular leaflet, tricuspid valve regurgitation and the atrialized right ventricle as well as associated malformation are the main pathological changes, so all operations should be performed under CPB with hypothermia, and all abnormalities should be corrected properly. Based on our understanding of cardiac reconstruction and right heart function, the best results of surgical treatment for EA can be obtained by anatomic correction. Protecting myocardium well and keeping the heart in normal sinus rhythm are needed.
Anatomical correction procedure aims at normalizing geometry of right ventricle by eliminating atrialized portion of the right ventricle. Atrialized ventricle is common in EA. When the atrialized portion of ventricle exceeds 3 cm in length, excising atrialized ventricle wall can reduce the size of the annulus and aid recovery of right ventricular geometry and function; however, attention must be paid to protecting the coronary arteries and myocardium. This complication of injury to coronary artery which can cause myocardial ischemia should be avoided.
Reconstruction of tricuspid valve is a very important factor to the good results for surgical treatment of EA patients. It is imperative to providing sufficient surface area of valvular leaflets to cover the orifice of the tricuspid valve and to rebuild the sub-valvular apparatus. Tricuspid valve annulus dilated can be reduced to normal size which needs to avoid stenosis in nearly all patients with EA. The downwards displacement valvular leaflets and abnormal chordae tendineae can be detached and reimplanted to normal level annulus. The normal leaflets, chordate, and papillary muscles should be kept in their position and never be detached, especially the anterior leaflet. If it was detached and the position was changed, it may cause the overtension of the leaflets and chordate and affect the compete closure of tricuspid valve and function of the right ventricle. This is significantly different from other techniques.[1–7,9] If the tricuspid leaflets' area is not large enough, one solution is to enlarge the leaflet with detached abnormal autologous leaflet, or with the addition of autologous pericardium. To avoid autologous pericardium shrinking or stiffening, which may cause valvular insufficiency after surgery, using an oversized autologous pericardium to increase the area of the effective valve leaflets is advantageous. A total of 131 patients (50.8%) had autologous pericardium enlargement of leaflets in this series of patients.
Due to the significant variety of pathological changes in EA patients, these factors exert a profound influence on the surgical outcomes. Therefore, we have to select different procedures for patients based on the findings before or during the operation. Drawing from our experience, the development of the anterior leaflets of the tricuspid valve serves as a pivotal indicator of the malformation's severity. The more severe the anterior leaflet downwards displacement or hypoplasia, the more severe the patient's cardiac malformation is. This may be due to the embryonic period development of the right ventricle, usually the anterior leaflet and anterior wall develop and mature earlier than the septal and posterior leaflets.[17–18] That is the reason we classify three types of our operative findings for procedures selection. Type I and Type II cases are amenable to anatomic correction, yielding exceptional outcomes. While for most type III patients, we have to select 1½ ventricle repair, valvular replacement, and other procedures where the results may be not satisfied. This classification is easier for surgeons to select the procedures and to compare different techniques and results of surgical treatment of EA.
There are limitations in this study. This study is retrospective in nature, encompassing varying patient ages, surgeries, follow-up durations, and incomplete follow-up data, which may potentially influence the conclusions drawn.
In conclusion, based on the management strategies, operative principles, and surgical techniques outlined above, anatomical correction procedures can achieve excellent long-term results with low rates of TCPC, 1½ ventricle repair, and valvular replacement.
Conflicts of interestNone.
References 1. Attenhofer Jost CH, Connolly HM, Dearani JA, Edwards WD, Danielson GK. Ebstein's anomaly. Circulation 2007;115: 277–285. doi: 10.1161/CIRCULATIONAHA.106.619338. 2. Brown ML, Dearani JA, Danielson GK, Cetta F, Connolly HM, Warnes CA, et al. The outcomes of operations for 539 patients with Ebstein anomaly. J Thorac Cardiovasc Surg 2008;135: 1120–1136, 1136.e1–7. doi: 10.1016/j.jtcvs.2008.02.034. 3. Dearani JA, Said SM, O'Leary PW, Burkhart HM, Barnes RD, Cetta F. Anatomic repair of Ebstein's malformation: lessons learned with cone reconstruction. Ann Thorac Surg 2012;95: 220–226. doi: 10.1016/j.athoracsur.2012.04.146. 4. Chauvaud S, Berrebi A, d'Attellis N, Mousseaux E, Hernigou A, Carpentier A. Ebstein's anomaly: repair based on functional analysis. Eur J Cardiothorac Surg 2003;23: 525–531. doi: 10.1016/S1010-7940(02)00836-9. 5. da Silva JP, Baumgratz JF, da Fonseca L, Franchi SM, Lopes LM, Tavares GM, et al. The cone reconstruction of the tricuspid valve in Ebstein's anomaly. The operation: early and midterm results. J Thorac Cardiovasc Surg 2007;133: 215–223. doi: 10.1016/j.jtcvs.2006.09.018. 6. Wu Q, Huang Z, Pan G, Wang L, Li L, Xue H. Early and midterm results in anatomic repair of Ebstein anomaly. J Thorac Cardiovasc Surg 2007;134: 1438–1440; discussion 1440–1442. doi: 10.1016/j.jtcvs.2007.08.019. 7. Davies RR, Pasquali SK, Jacobs ML, Jacobs JJ, Wallace AS, Pizarro C. Current spectrum of surgical procedures performed for Ebstein's malformation: an analysis of the Society of Thoracic Surgeons Congenital Heart Surgery Database. Ann Thorac Surg 2013;96: 1703–1709. doi: 10.1016/j.athoracsur.2013.05.005. 8. Anderson KR, Lie JT. The right ventricular myocardium in Ebstein's anomaly: a morphometric histopathologic study. Mayo Clin Proc 1979;54: 181–184. 9. Carpentier A, Chauvaud S, Macé L, Relland J, Mihaileanu S, Marino JP, et al. A new reconstructive operation for Ebstein's anomaly of the tricuspid valve. J Thorac Cardiovasc Surg 1988;96: 92–101. doi: 10.1378/chest.94.1.224. 10. Bartlett HL, Atkins DL, Burns TL, Engelkes KJ, Powell SJ, Hills CB, et al. Early outcomes of tricuspid valve replacement in young children. Circulation 2007;115: 319–325. doi: 10.1161/CIRCULATIONAHA.106.618652. 11. Chauvaud S, Fuzellier JF, Berrebi A, Lajos P, Marino JP, Mihaileanu S, et al. Bi-directional cavopulmonary shunt associated with ventriculo and valvuloplasty in Ebstein's anomaly: benefits in high risk patients. Eur J Cardiothorac Surg 1998;13: 514–519. doi: 10.1016/S1010-7940(98)00057-8. 12. Wu Q, Huang Z. Anatomic correction of Ebstein anomaly. J Thorac Cardiovasc Surg 2001;122: 1237–1238. doi: 10.1067/mtc.2001.116463. 13. Wu Q, Huang Z. A new procedure for Ebstein's anomaly. Ann Thorac Surg 2004;77: 470–476. doi: 10.1016/S0003-4975(03)01492-9. 14. Wu Q, Pan G, Li H, Kong X. Anatomic repair of Ebstein's anomaly with isolated anterior leaflet downward displacement. J Thorac Cardiovasc Surg 2014;148: 1454–1458.e1. doi: 10.1016/j.jtcvs.2014.02.075. 15. Danielson GK, Driscoll DJ, Mair DD, Warnes CA, Oliver WC Jr. Operative treatment of Ebstein's anomaly. J Thorac Cardiovasc Surg 1992;104: 1195–1202. doi: 10.1007/BF00705581. 16. Hetzer R, Nagdyman N, Ewert P, Weng YG, Alexi-Meskhisvili V, Berger F, et al. A modified repair technique for tricuspid incompetence in Ebstein's anomaly. J Thorac Cardiovasc Surg 1998;115: 857–868. doi: 10.1016/S0022-5223(98)70367-8. 17. Ramcharan TKW, Goff DA, Greenleaf CE, Shebani SO, Salazar JD, Corno AF. Ebstein's Anomaly: from Fetus to Adult—Literature Review and Pathway for Patient Care. Pediatr Cardiol. 2022;43: 1409–1428. doi: 10.1007/s00246-022-02908-x. 18. Wouter H. Lamers, Szabolcs Virágh, Andy Wessels, Antoon F.M. Moorman, Robert H. Anderson. Formation of the Tricuspid Valve in the Human Heart. Circulation. 1995;91: 111–121. doi: 10.1161/01.CIR.91.1.111.
留言 (0)