
記住我








Hidradenocarcinoma is a rare adnexal tumor of the sweat glands with a high rate of recurrence and metastasis (Tolkachjov et al., 2015). Although sweat gland carcinomas have a 0.05% incidence, hidradenocarcinomas account for only 0.001% of all cancers (Soni et al., 2015) and are typically found on the head and neck (McMains et al., 2020; Rafols et al., 2020). Given the rarity of the malignancy, there is limited consensus on treatment. Here, we present a case of recurrent hidradenocarcinoma at the knee despite excision and radiation.
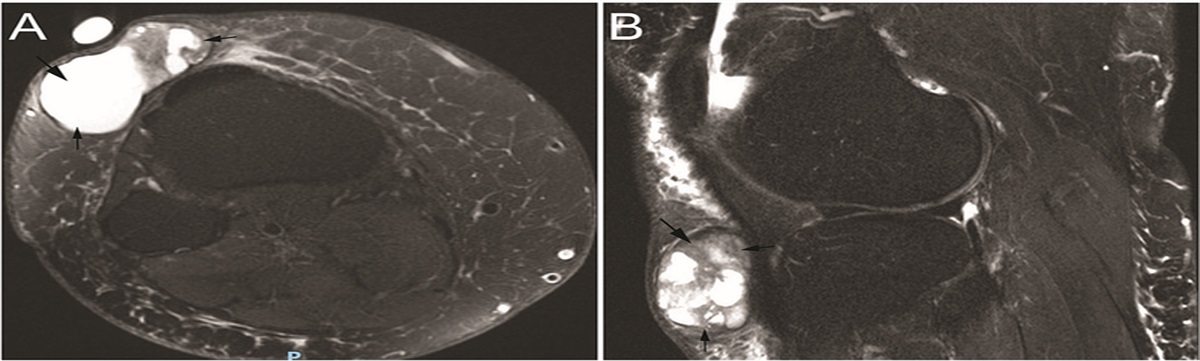
REPORTA 67-year-old woman presented with a small subcutaneous mass over her right knee that had been present for nearly 20 years. She was told over the years by several providers that this was a ganglion cyst. Despite not noticing a change in size, she recently found the lesion was becoming more uncomfortable, particularly when kneeling. She denied any trauma or inciting events. Physical examination found an approximately 5-cm mobile, nontender mass over the anterior knee, distal to the patella. A subsequent magnetic resonance imaging study indicated a 3.8 cm × 4.9 cm × 2.1 cm subcutaneous multilobulated fluid-filled mass with no penetration into the knee joint fascia (Figure 1A and B). She underwent surgical excision with positive margins. Histopathology of the resection specimen, which was received in multiple fragments, showed a tumor with a multilobulated architecture with numerous infiltrative smaller islands and nests embedded in a hyalinized stroma (Figure 2A). The tumor was composed of cuboidal epithelial cells with interspersed areas of squamous differentiation. Areas of necrosis and cystic change were identified in the larger tumor lobules (Figure 2B and C). Ductal differentiation was identified in both areas with cuboidal and squamous areas (Figure 2C). The tumor was sampled extensively, but no residual component of a benign-appearing tumor such as hidradenoma was identified in the sections examined. A diagnosis of hidradenocarcinoma was rendered. Positron emission tomography–computed tomography after excision exhibited mild F-fluorodeoxyglucose uptake in the right inguinal lymph nodes. Ultrasound-guided fine-needle aspiration was performed to rule out metastases, showing only lymphoid tissue with no malignant cells. Given the positive margin status of the excision and the unexpected diagnosis of carcinoma, the patient completed 60-Gray adjuvant radiation to the surgical bed postoperatively.
 FIGURE 1.:
FIGURE 1.: Preoperative T2-weighted contrast-enhanced magnetic resonance imaging of the knee joint region, (A) axial section and (B) sagittal section. The arrows point to the cystic heterogenous mass without communication with the joint space.
 FIGURE 2.:
FIGURE 2.: (A) (36× original magnification) Hidradenocarcinoma, composed of multilobulated tumor with cystic spaces (diagonal arrows) and smaller infiltrative nests and islands of tumor in a hyalinized stroma (vertical arrows), received in multiple fragments. (B) (112× original magnification) The tumor exhibits cystic areas composed of cuboidal cells interspersed with squamous cells (diagonal arrows). (C) (200× original magnification) Tumor areas show evidence of ductal differentiation (vertical arrows).
Eight months later, the patient returned with a concern for recurrence as she noticed a small nodular lesion at the prior incision site (Figure 3A). She underwent biopsy that was consistent with recurrence of hidradenocarcinoma (Figure 3B and C). The malignancy was then reexcised with 2-cm margins, leaving a large soft tissue deficit. After confirmation of negative margins, plastic surgery colleagues performed reconstruction using a local medial gastrocnemius muscle flap. The patient has had no evidence of recurrence at follow-up 1 year after the reconstructive flap.
 FIGURE 3.:
FIGURE 3.: (A) A small pink nodular lesion consistent with clinically recurrent hidradenocarcinoma at prior incision site on the right knee. (B) (3.8× original magnification with hematoxylin-eosin staining) The overlying epidermis, although ulcerated with formation of a hyperparakeratotic scale and in direct communication with the underlying tumor, does not show evidence of dysplasia or actinic change. Scattered tumor islands show variably sized microcystic and duct-like spaces. (C) (200× original magnification with hematoxylin-eosin staining) Eosinophilic tumor cells with moderately pleomorphic centrally placed nuclei, arranged in irregular and serpiginous islands infiltrative in the dermis.
DISCUSSIONHidradenocarcinoma is a malignant adnexal tumor arising from the apocrine and eccrine glands. These nodules have a variable natural history and may be asymptomatic for decades (Soni et al., 2015). It often presents as solitary mass that arises de novo but can also transform from a benign hidradenoma (Guillot, 2009; Jinnah et al., 2016). Hidradenocarcinoma is most often seen on the face and neck but less commonly at the distal extremities (Soni et al., 2015). After conversion to a malignant phenotype, it has a predilection to metastasize to the lymph nodes and bone (Rafols et al., 2020; Soni et al., 2015). The risk of local tumor recurrence is high, with a probability of approximately 50% (Guillot, 2009). Patients with hidradenocarcinomas have a 39% risk of nodal metastasis and a 28% risk of visceral metastatic involvement (Guillot, 2009).
As with our patient, hidradenocarcinoma can easily mimic other dermatologic conditions, and it is vital to distinguish it from benign pathologies like lipomas and cysts (McMains et al., 2020). In a retrospective chart review of patients with hidradenocarcinoma at Mayo Clinic, zero of seven patients were suspected to have the malignancy when evaluated by academic dermatologists (Tolkachjov et al., 2015). Thus, it is vital to keep this in the differential diagnosis of hemangiomas, basal and squamous cell carcinomas, and lymphangiomas (Jinnah et al., 2016; Soni et al., 2015). The diagnosis of hidradenocarcinoma is based on histologic and morphologic examination of the tumor, and immunohistochemistry has a limited role. As in other skin adnexal tumors, high-molecular-weight cytokeratin (CK5/6) expression is seen (Gauerke & Driscoll, 2010; Jinnah et al., 2016). Histologic features include nest of cells formed from a mixture of squamous, mucinous, and polygonal cell types (Gauerke & Driscoll, 2010). Clear cells expressing periodic acid–Schiff and spindle cells can also be present (Guillot, 2009). The diagnosis of malignancy is based on the presence of an infiltrative growth pattern, cytologic atypia, necrosis, increased mitotic activity, and lymphovascular invasion (Gauerke & Driscoll, 2010; Soni et al., 2015).
Considering the condition's rarity, there is little agreement on how to proceed with treatment as no clinical trials have been performed. A surgical approach with wide local excision is the current mainstay. Previous reports of Mohs micrographic surgery have shown improved outcomes with no recurrence or metastasis in follow-up from 1 to 5 years (Tolkachjov et al., 2015). In cases of a large defect after wide local excision, reconstruction using a local muscle flap is a viable option, particularly in the lower extremity (McMains et al., 2020). Radiation therapy is helpful as adjuvant therapy to excision in instances of vasculature or neural involvement (Miller et al., 2015; Soni et al., 2015). Despite these options, tumor recurrence after surgical excision remains approximately 50% (Soni et al., 2015).
Given its metastatic potential, hidradenocarcinoma requires not only local biopsy but also sentinel nodes examination and imaging to rule out local spread (Soni et al., 2015). There has been a recommendation to excise biopsy-proven hidradenocarcinoma with 3-cm margins as well as perform sentinel lymph node biopsy to help with staging (McMains et al., 2020). Fine-needle aspiration may also be utilized to rule out metastasis (Rafols et al., 2020). Imaging with magnetic resonance imaging can help with diagnosis when metastatic hidradenocarcinoma is suspected but histologic examination is not confirmatory (Moore et al., 2021). Targeted therapy using drugs like sunitinib and capecitabine can be helpful in some cases of metastases (Guillot, 2009; Korbi et al., 2020).
This case highlights the aggressive nature of hidradenocarcinoma and that, despite local excision and large-dose radiation, malignancy can recur. Additional research is needed to determine potential treatment options, but patients will need annual lifelong follow-up.
REFERENCES Gauerke S., Driscoll J. J. (2010). Hidradenocarcinomas: A brief review and future directions. Archives of Pathology & Laboratory Medicine, 134(5), 781–785. 10.5858/134.5.781 Guillot B. (2009). From unusual cutaneous malignancies: Cutaneous adnexal tumors. In Y. Belkacemi, R. Mirimanoff, M. Ozsahin (Eds.), Management of rare adult tumors ( ed., pp. 471–477). Springer-Verlag France. Jinnah A. H., Emory C. L., Mai N. H., Bergman S., Salih Z. T. (2016). Hidradenocarcinoma presenting as soft tissue mass: Case report with cytomorphologic description, histologic correlation, and differential diagnosis. Diagnostic Cytopathology, 44(5), 438–441. 10.1002/dc.23449 Korbi S., Rachdi H., El Benna H., Mejri N., Berrazaga Y., Daoud N., Labidi S., Boussen H. (2020). Objective clinical and radiological response under sunitinib in a case of thigh hidradenocarcinoma. Case Reports in Oncological Medicine, 2020, 9656475. 10.1155/2020/9656475 McMains C. J., Hung R. W., Deng T., Masden D. L. (2020). A case for a local flap as primary reconstruction for hidradenocarcinoma of the leg. Plastic and Reconstructive Surgery. Global Open, 8(5), e2780. 10.1097/GOX.0000000000002780 Miller D. H., Peterson J. L., Buskirk S. J., Vallow L. A., Ta R., Joseph R., Krishna M., Ko S. J., Tzou K. S. (2015). Management of metastatic apocrine hidradenocarcinoma with chemotherapy and radiation. Rare Tumors, 7(3), 6082. 10.4081/rt.2015.6082 Moore J. A., Cui S., Berger N., Kim S., O'Guinn D., Labow D., Kamath A. (2021). Hidradenocarcinoma: A rare but challenging diagnosis. Clinical Imaging, 75, 138–142. 10.1016/j.clinimag.2021.01.024 Rafols M., Mejia O., Oh K. S., Bendixen B., Jorge I., Narayanan S. (2020). An unusual case of lower extremity clear cell hidradenocarcinoma. Case Reports in Surgery, 2020, 6192109. 10.1155/2020/6192109 Soni A., Bansal N., Kaushal V., Chauhan A. K. (2015). Current management approach to hidradenocarcinoma: A comprehensive review of the literature. Ecancermedicalscience, 9, 517. 10.3332/ecancer.2015.517 Tolkachjov S. N., Hocker T. L., Hochwalt P. C., Camilleri M. J., Arpey C. J., Brewer J. D., Otley C. C., Roenigk R. K., Baum C. L. (2015). Mohs micrographic surgery for the treatment of hidradenocarcinoma: The Mayo Clinic experience from 1993 to 2013. Dermatologic Surgery, 41(2), 226–231. 10.1097/DSS.0000000000000242
留言 (0)