
記住我








Skin tumors encompass a wide range of benign and malignant lesions that can arise from various cellular components of the skin. The pattern of skin cancer in different geographical areas depends on genetic and environmental factors (Ghasemzadeh et al., 2017; Khan et al., 2022). Skin cancers are associated with diminished quality of life and high levels of disability (Q. Liu et al., 2023). However, most skin cancers, except melanoma, have a relatively low mortality rate (So et al., 2021). Skin tumors can be broadly classified into benign and malignant lesions, including keratinocyte, melanocytic, appendageal, and hematolymphoid tumors (Elder et al., 2018).
The origin of skin tumors can be from basal cell layer cells, squamous cells, melanocytes, immune system cells, skin appendages, vascular tissue, connective tissue, or metastases from internal organs (Gandhi & Kampp, 2015). Basal cell carcinoma (BCC) is the most common type of skin cancer globally, accounting for approximately 80% of all cases, primarily affecting sun-exposed areas such as the face, scalp, ears, and neck. Its incidence is exceptionally high in regions with high levels of sun exposure (Cojocaru et al., 2021; Naik & Desai, 2022). Squamous cell carcinoma (SCC) is the second most prevalent type, representing approximately 20% of skin cancer cases worldwide. It commonly arises from chronically sun-damaged skin, including the head, neck, upper extremities, and lower legs (Fania et al., 2021). SCC is also seen in the setting of trauma, chronic inflammation, and immune suppression (Liu et al., 2021; Xu et al., 2022). Melanoma, although less common, is the most aggressive form of skin cancer, responsible for most skin-cancer-related deaths. Melanomas can arise in both sun-exposed and non-sun-exposed areas, including the trunk, extremities, and mucosal surfaces (Davey et al., 2021).
Ultraviolet (UV) radiation exposure is the primary environmental risk factor for developing skin tumors, especially in areas without a protective covering, such as the face (Teng et al., 2021).
Prolonged exposure to UV radiation, whether from sunlight or artificial sources such as tanning beds, leads to DNA damage and genetic mutations in the skin cells (D'Orazio et al., 2013). Fair skin, upper age, a history of sunburns, and a family history of skin cancer are associated with an increased risk of developing skin tumors (Davis et al., 2021). Accurate and timely diagnosis is crucial for effective management of skin tumors. Diagnosing skin tumors involves a comprehensive evaluation of clinical features, dermoscopic examination, and histopathological analysis (Kalloniati et al., 2021).
Because of the increasing prevalence of skin cancer and the associated high treatment costs, knowledge about its associated risk factors is imperative. Moreover, the prevalence and patterns of skin tumors remain unclear in Guilan Province, Iran, and further research is warranted to advance our knowledge of the underlying mechanisms, improve diagnostic techniques, and develop targeted therapies to enhance patient outcomes in the management of skin tumors. In this regard, the current study investigated the prevalence of various skin lesions among patients from 2016 to 2021 in Guilan, Iran.
METHODS Study Design and PatientsThis descriptive cross-sectional study was conducted on 559 patients with skin lesions diagnosed with a dermatologist or specialist and sent to Razi Pathobiology Laboratory, Rasht, Iran, from 2016 to 2021. The demographical data, clinical characteristics, and tumor types were collected through a checklist. Skin findings were evaluated by clinical examination and histopathological findings, and the agreement between the results was assessed. Data included age and gender, area of involvement (head, face, neck, anterior trunk, posterior trunk, upper limb, lower limb, and genital area), and type of tumors (benign, premalignant, malignant, and malformation). Various types of detected skin lesions were seborrheic keratosis, skin tag, dermatofibroma, keloid and hypertrophic scar, nevus sebaceous, epidermal cyst, pilar cyst, sebaceous hyperplasia, BCC, SCC, actinic keratosis, Bowen's disease, Paget's disease of the breast, cutaneous metastasis, congenital melanocytic nevus, melanoma, angiokeratoma, pyogenic granuloma, Kaposi's sarcoma, cutaneous T-cell lymphoma (mycosis fungoides type), dermatofibrosarcoma protuberans, keratoacanthoma, pilar sheath acanthoma, arteriovenous malformation, capillary hemangioma, Spitz nevus, epidermal nevus, compound nevus, angiofibroma, basosquamous cell carcinoma, intradermal nevus, atypical fibroxanthoma, benign squamous papilloma, venous lake, fibroma, syringoma, extramammary Paget's disease, cherry angioma, pilomatricoma, junctional nevus, angiosarcoma (lymphangiosarcoma), halo nevus, and storiform collagenoma. Patients with incomplete data, a previous history of skin tumors, and immunodeficiency were excluded from the study. This study was approved by the ethical committee of the Guilan University of Medical Sciences, Rasht, Iran (IR.GUMS.REC.1400.559). All patients gave their consent to participate in the study.
Statistical AnalysisMean ± standard deviations, numbers, and percentages were used to report variables. Pearson's correlation coefficient, chi-square test, and Fisher exact test were performed to assess the association between variables. On the basis of phi's agreement coefficient, the rate of agreement between results was assessed. Data were analyzed using the IBM SPSS Statistics Version 21, based on a significance level of less than current study's findings illustrated that, from 559 evaluated skin lesions, 286 (51.2%) and 273 (48.8%) were detected in males and females, respectively. Among males, 144 (50.3%), 14 (4.9%), 127 (44.4%), and 1 (0.4%) patients had benign tumors, premalignant tumors, malignant tumors, and malformation lesions, respectively, and among females, 152 (55.7%), 24 (8.8%), and 97 (35.5%) patients had benign, premalignant, and malignant tumors, respectively (Pearson correlation = 7.567, p = .056). The mean age of patients was 54.86 ± 19.57 years (ranging from 3 to 93 years). Among males, the average age was 59.18 ± 18.8 years (ranging from 3 to 92 years), whereas among females, it was 50.34 ± 19.37 years (ranging from 6 to 93 years). As shown in Table 1, the age group of 58–68 years had the highest frequency of skin lesions, whereas the age group of 3–13 years had the lowest frequency of skin lesions (p < .001).
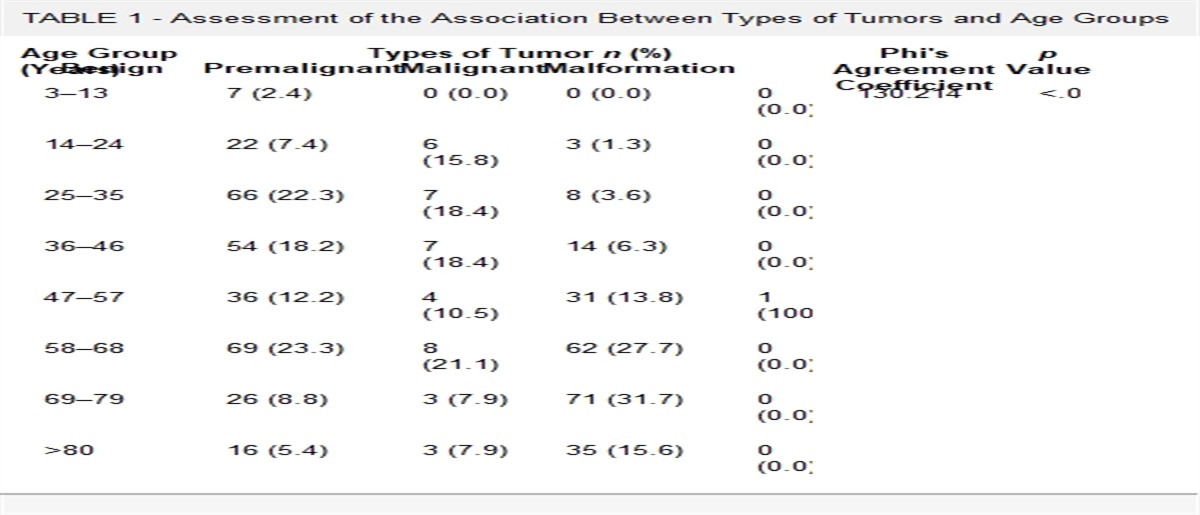
TABLE 1 - Assessment of the Association Between Types of Tumors and Age Groups Age Group (Years) Types of Tumor n (%) Phi's Agreement Coefficient p Value Benign Premalignant Malignant Malformation 3–13 7 (2.4) 0 (0.0) 0 (0.0) 0 (0.0) 130.214 <.001 14–24 22 (7.4) 6 (15.8) 3 (1.3) 0 (0.0) 25–35 66 (22.3) 7 (18.4) 8 (3.6) 0 (0.0) 36–46 54 (18.2) 7 (18.4) 14 (6.3) 0 (0.0) 47–57 36 (12.2) 4 (10.5) 31 (13.8) 1 (100.0) 58–68 69 (23.3) 8 (21.1) 62 (27.7) 0 (0.0) 69–79 26 (8.8) 3 (7.9) 71 (31.7) 0 (0.0) >80 16 (5.4) 3 (7.9) 35 (15.6) 0 (0.0)Most lesions were located on the face, and benign tumors had a higher frequency than others; most skin lesions were reported in 2016 and 2021 (Table 2). Among benign tumors, seborrheic keratosis and intradermal nevus were more prevalent. Actinic keratosis and BCC were more frequent among premalignant and malignant tumors, respectively (Table 3). Evaluation of the agreement between histopathological findings and clinical examination showed a 79.4% similarity (n = 444) and a 20.6% disparity (n = 115). In these cases, a dermatologist diagnosed 70.8% (n = 396) of the cases, and 29.2% (n = 163) were diagnosed by other specialists. Among diagnosed benign, premalignant, and malignant tumors, 77% (n = 228), 71.1% (n = 27), and 84.4% (n = 189), respectively, were similarly diagnosed by both clinical and histopathological examination (Pearson correlation = 9.891, p = .020). As illustrated in Table 4, the face was the most frequent area engaged with skin lesions, and the genital area had the lowest frequency (Pearson correlation = 37.189, p = .05).
TABLE 2 - Frequency of Skin Lesions According to the Years Year Type of Tumors n (%) Benign Premalignant Malignant Malformation Total 2016 110 (54.2) 10 (4.9) 82 (40.4) 1 (0.5) 203 2017 8 (34.8) 1 (4.3) 14 (60.9) 0 23 2018 11 (47.8) 3 (13.0) 9 (39.1) 0 23 2019 6 (37.5) 0 (0.0) 10 (62.5) 0 16 2020 6 (54.4) 2 (18.2) 3 (27.3) 0 11 2021 155 (54.8) 22 (7.8) 106 (37.5) 0 283Skin cancer is the most common carcinoma with an increased incidence that threatens public health. In this regard, the knowledge of the frequency, epidemiology, etiology, and risk factors related to this disease is essential for the healthcare system to enhance patients' outcomes. The current study investigated the frequency of different types of skin lesions in Guilan, Iran, from 2016 to 2021. According to our results, the ratio of skin tumors in males to females was 1.04:1. Our findings align with the reports of Sinikumpu et al., which highlight that males have a twofold increased risk of developing skin tumors compared with females (Sinikumpu et al., 2022). Environmental factors, ethics, different physiology, skin structure, and the effect of sex hormones may interact to exert the influences of gender on the chance of developing skin lesions (Chen et al., 2010). Similar to our findings, the male–female ratio was reported to be 1.03:1 with the age range of 5–85 years. They also observed that the age group of 20–39 years (40.91%) followed by 40–59 years (26.36) were more affected by skin cancers compared with other age groups (Kaur et al., 2017). The mean age of patients in the current study was approximately 55 years, which showed the prevalence of skin disease at a younger age for females than males. As expected, malignant skin tumors were more common in older adults (Shrestha et al., 2021; Thapa et al., 2018). Numerous studies have revealed that benign tumors occur more frequently in younger age groups (≤50 years; Shrestha et al., 2021; Thapa et al., 2018), and malignant tumors occur mainly in older age groups (≥51 years; Harahap, 1982; Rajbhar et al., 2020; Shrestha et al., 2021; Thapa et al., 2018).
Our findings indicated that the highest frequency of benign tumors was observed in patients aged 58–68 and 25–35 years, respectively. In addition, the highest frequency of malignant tumors was shown in the age group of 69–79 years, which increases with aging. However, regarding tumor trends in our population, women have a higher proportion of benign skin tumors, and a higher prevalence of malignant skin tumors was seen in men. This finding was similar to the reported frequency of skin tumors in the Philippines, India, Singapore, Nepal, and Indonesia (Bhuvan et al., 2017; Harahap, 1982; Tan et al., 1995; Thapa et al., 2018; Villanueva, 2022). Al-Naggar's findings could explain that men are less likely than women to take skin cancer prevention care, such as using sunscreen and wearing hats, especially for those who work outdoors (Al-Naggar, 2013). Consequently, men are more susceptible to exposure to UV radiation, a risk factor for developing skin cancer (Bradford, 2009). Moreover, aging affects all skin layers and alters skin structure, possibly resulting in skin tumors (Csekes & Račková, 2021). Exposure to UV increases melanogenesis caused by oxidative stress that results in cellular dysfunction with aging, and damage is the core biomarker of aging that is commonly observed in photodamaged skin (Hipkiss, 2006; Lee et al., 2021).
The face is the area with the most exposure to UV (DNA damage), making it more susceptible to UV-related skin lesions. In the current study, skin tumors originating in the face were more frequent than those in other areas. Furthermore, the head and neck were the second most frequent areas for benign and premalignant tumors. In line with our findings, it has been reported that most skin tumors were located on the face/head/neck, which are less covered and protected against UV (Fijałkowska et al., 2021; Rajbhar et al., 2020). According to our results, the frequency of all kinds of tumors was higher in 2021 compared with other years studied. However, there was no observed increase in the incidence of skin tumors in Guilan, Iran, from 2016 to 2021. This is in contrast to a previous report that showed a significant increasing trend in skin tumors during 2010–2014 (Darjani et al., 2021). Moreover, Afzali et al. showed a rising trend for skin tumors between 2000 and 2011 (Afzali et al., 2013).
According to our findings, seborrheic keratosis, actinic keratosis, and BCC were the most reported benign, premalignant, and malignant tumors, respectively. Similarly, various studies reported seborrheic keratosis as the most common benign skin tumor in clinical dermatological practice, with an increasing incidence with age that can be diagnosed clinically in most cases because of its characteristics and appearance (Barthelmann et al., 2023; Wollina, 2018). In addition, studies reported that actinic keratosis and Bowen's disease are common premalignant skin tumors triggered by excessive exposure to UV (Bakshi et al., 2020; Korhonen et al., 2021). Consistent with our findings, Kim et al. reported that BCC and SCC were the most prevalent malignant tumors (Kim et al., 2010). Our findings highlighted a high agreement (79.4%) between clinical diagnosis and histopathological findings. The compatibility between clinical diagnosis and histopathological diagnosis is essential because both findings are required for correct and definite diagnosis of the tumors (Jamshidi et al., 2019). The concordance level between histopathological and clinical findings varies for different types of skin tumors (Sopjani et al., 2022). Our results illustrated that clinicians could correctly diagnose most skin tumors, which would help with early treatment strategies.
CONCLUSIONThe current study showed that the prevalence of skin tumors increased with age, and some areas of the body without protective covers, such as the head and neck and, most commonly, the face, are more vulnerable to developing skin tumors. In addition, we observed a high level of compatibility between clinical diagnosis and histopathological findings of skin tumors. As BCC was the most commonly malignant tumor among the study population, better patient education of sun-protective measures is required to reduce the development of this skin cancer.
REFERENCES Afzali M., Mirzaei M., Saadati H., Mazloomi-mahmood-abadi S. S. (2013). Epidemiology of skin cancer and changes in its trends in Iran. 17(5), 501–511. 10.32598/JGUMS.29.4.1606.1 Al-Naggar R. A. (2013). Practice of skin cancer prevention among road traffic police officers in Malaysia. Asian Pacific Journal of Cancer Prevention, 14(8), 4577–4481. 10.7314/APJCP.2013.14.8.4577 Bakshi A., Shafi R., Nelson J., Cantrell W. C., Subhadarshani S., Andea A., Athar M., Elmets C. A. (2020). The clinical course of actinic keratosis correlates with underlying molecular mechanisms. The British Journal of Dermatology, 182(4), 995–1002. 10.1111/bjd.18338 Barthelmann S., Butsch F., Lang B. M., Stege H., Großmann B., Schepler H., Grabbe S. (2023). Seborrheic keratosis. JDDG: Journal der Deutschen Dermatologischen Gesellschaft, 21(3), 265–277. 10.1111/ddg.14984 Bhuvan A., Miskin A. T., Inamdar S. S., Mural P. (2017). A histomorphological study of malignant skin tumors. International Journal of Life-Sciences Scientific Research, 3(4), 1162–1166. Bradford P. T. (2009). Skin cancer in skin of color. Dermatology Nursing, 21(4), 170–177. Chen W., Mempel M., Traidl-Hofmann C., Al Khusaei S., Ring J. (2010). Gender aspects in skin diseases. Journal of the European Academy of Dermatology and Venereology, 24(12), 1378–1385. 10.1111/j.1468-3083.2010.03668.x Cojocaru A., Marinescu E. A., Nica O., Ilinoiu E., Negrila A., Ciurea M. E. (2021). Basal cell carcinoma and its impact on different anatomical regions. Current Health Sciences Journal, 47(1), 75–83. 10.12865/CHSJ.47.01.12 Csekes E., Račková L. (2021). Skin aging, cellular senescence and natural polyphenols. International Journal of Molecular Sciences, 22(23), 12641. 10.3390/ijms222312641 Darjani A., Alizadeh A., Gharaei Nejad K., Hojat Eftekhari, Rafiei R., Shafaei Tonekaboni S., Shamsa F. (2021). Epidemiology and trends of skin cancers in Guilan Province, Iran during 2010–2014. Gums-Med, 29(4), 154–165. http://journal.gums.ac.ir/article-1-2294-en.html. 10.32598/JGUMS.29.4.1606.1 Davey M. G., Miller N., McInerney N. M. (2021). A review of epidemiology and cancer biology of malignant melanoma. Cureus, 13(5), e15087. 10.7759/cureus.15087 Davis D. S., Robinson C., Callender V. D. (2021). Skin cancer in women of color: Epidemiology, pathogenesis and clinical manifestations. International Journal of Women's Dermatology, 7(2), 127–134. 10.1016/j.ijwd.2021.01.017 D'Orazio J., Jarrett S., Amaro-Ortiz A., Scott T. (2013). UV radiation and the skin. International Journal of Molecular Sciences, 14(6), 12222–12248. 10.3390/ijms140612222 Elder D. E., Massi D., Scolyer R. A., Willemze R. 2018. WHO classification of skin tumours. Lyon, France: IARC, 4th edition. https://cir.nii.ac.jp/crid/1130282272667884288 Fania L., Didona D., di Pietro F. R., Verkhovskaia S., Morese R., Paolino G., Donati M., Ricci F., Coco V., Ricci F., Candi E., Abeni D., Dellambra E. (2021). Cutaneous squamous cell carcinoma: From pathophysiology to novel therapeutic approaches. Biomedicine, 9(2), 171. 10.3390/biomedicines9020171 Fijałkowska M., Koziej M., Antoszewski B. (2021). Detailed head localization and incidence of skin cancers. Scientific Reports, 11(1), 12391. 10.1038/s41598-021-91942-5 Gandhi S. A., Kampp J. (2015). Skin cancer epidemiology, detection, and management. The Medical Clinics of North America, 99(6), 1323–1335. 10.1016/j.mcna.2015.06.002 Ghasemzadeh F., et al. (2017). Determination of the most important factors affecting non-melanoma skin cancer using data mining algorithms. Jhbmi, 4(1), 39–47. http://jhbmi.ir/article-1-204-en.html Harahap M. (1982). Skin cancer among Indonesians in three provinces of Indonesia. International Journal of Dermatology, 21(9), 521–525. 10.1111/j.1365-4362.1982.tb01197.x Hipkiss A. R. (2006). Accumulation of altered proteins and ageing: Causes and effects. Experimental Gerontology, 41(5), 464–473. 10.1016/j.exger.2006.03.004
留言 (0)