
記住我









An 11-year-old female adolescent was brought to the emergency department with a 3-day history of progressive neck pain with limited mobility associated with left facial swelling. There was no history of trauma, fever, sore throat, ear pain, runny nose, cough, abdominal pain, nausea or vomiting. The patient had no difficulty swallowing but reported decreased appetite. She had not been ill, has no known sick contacts and her immunizations are up to date. She lived with her parents in a rural area with no animal exposure. On arrival in the emergency department, she had a temperature of 36.8 °C, heart rate of 68 beats per minute, blood pressure of 112/74 mm Hg, respiratory rate of 18 breaths per minute and oxygen saturation of 98% ambient air. On physical examination, she was uncomfortable, with left torticollis, diffuse tenderness upon palpation of the trapezius muscles bilaterally, associated with muscle contraction and significant limitation in range of motion (especially cervical rotation). No pain was elicited in the cervical spinous processes. Neurological deficits were not observed. Examination of the oropharynx and ear revealed no abnormalities with no dental problems. There were no palpable enlarged lymph nodes and no peripheral edemas. The remainder of the physical examination was normal. Laboratory analysis revealed a white blood cell count of 6.9 × 103/μL with 52% neutrophils, 42% lymphocytes, 3% monocytes and 0.5% eosinophils, hemoglobin of 14.7 g/dL, platelets count of 323 × 103/μL, C-reactive protein of 5.0 mg/L and erythrocyte sedimentation rate of 8 mm/h. Blood culture results were negative and the blood chemistry panel was normal. Rapid Streptococcus pyogenes test on throat swab was negative. She was initially treated with ibuprofen, diazepam and ketorolac, but the patient showed no clinical improvement. A cervical and soft tissue computed tomography (CT) scan revealed the diagnosis.
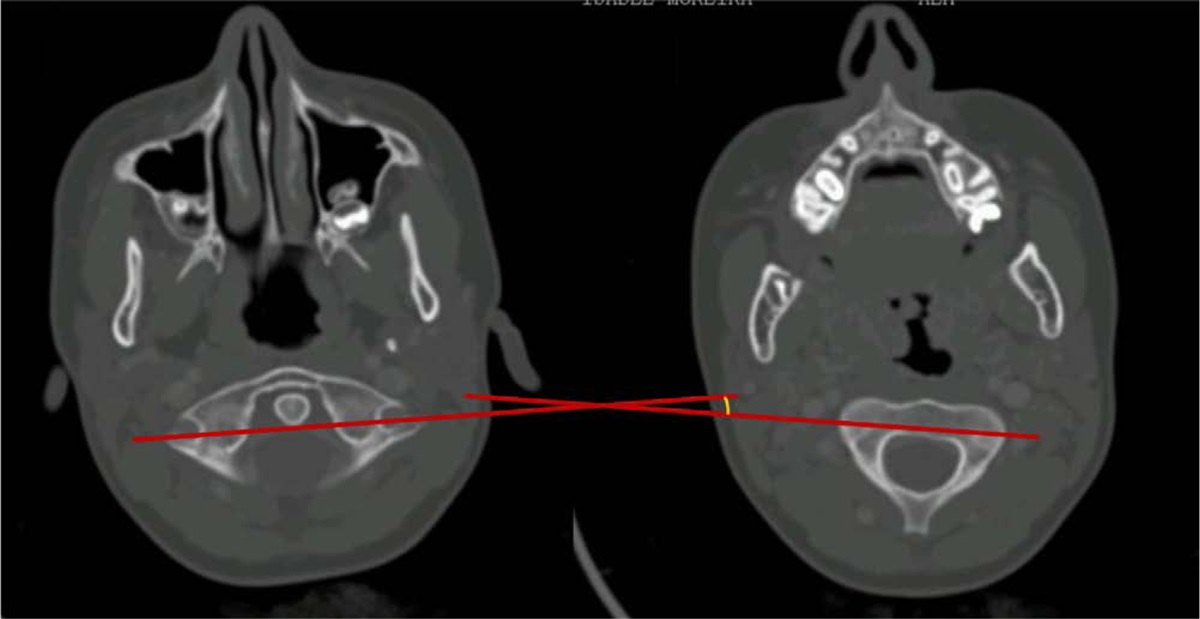
DENOUEMENTThe cervical and soft tissue CT scan revealed a peritonsillar abscess (3 × 8 mm) on the right side with multiple bilateral cervical lymph nodes, as well as grade I Fielding rotatory subluxation of C1-C2 without associated bony lesions (Fig. 1). These findings established the diagnosis of Grisel syndrome (GS). The patient was evaluated by the orthopedics department and subsequently admitted to the hospital. She received amoxicillin-clavulanate intravenously (150 mg/kg/d), a soft cervical collar, muscle relaxants and nonsteroidal anti-inflammatory drugs medication. Otolaryngological consultation recommended cervical immobilization for 7 days. The patient’s symptoms resolved and she was discharged on the 9th day of hospitalization to complete 14-day course of antibiotic therapy. One month later, she was reevaluated, and there were no complaints. A cervical CT scan done 2 months later showed complete resolution of the rotatory atlantoaxial subluxation (Fig. 2).
 FIGURE 1.:
FIGURE 1.: Rotatory C1-C2 subluxation (Fielding I).
 FIGURE 2.:
FIGURE 2.: CT scan at follow-up (2 months later).
GS is a rare condition characterized by nontraumatic atlantoaxial rotatory displacement, a rotatory subluxation between the C1 and C2 vertebrae. It was first described in 1830, when Bell1 reported a case of atlantoaxial subluxation that resulted in spinal cord compression in a patient with pharyngeal syphilitic ulceration. Later, in 1930, Grisel2 described 2 similar cases, and his name was given to the disorder. Common causes include infections (upper respiratory tract infections, pharyngeal abscess, otitis media and mumps), recent head or neck surgery (mainly postadenotonsillectomy) and idiopathic or other associated conditions, such as Down syndrome, instillation of eye drops in patients with ligament laxity and central line placement.3 The pathophysiology is poorly understood. Some authors postulate that the hematogenous spread of infection from the posterior-superior pharynx to the cervical spine is the initial event. Subsequently, hyperemia, distension and abnormal relaxation of the atlantoaxial ligaments lead to destabilization and subsequent subluxation of the joint. The transverse and alar ligaments, which primarily resist the forward movement of the atlas on the axis, are likely to be affected. Alternatively, some authors suggest that subluxation is secondary to muscle spasms in the cervical region, triggered by circulating inflammatory mediators in the bloodstream.4 It typically presents with symptoms, such as torticollis, cervical pain, head tilting and limited, painful neck movements. A strong suspicion of this condition may arise when there is an obvious displacement of the spinous process of the axis corresponding to the side of neck rotation during manual examination. Additional signs include muscle spasm in the sternocleidomastoid muscle on the same side as the rotation and an inability to turn the head past the midline toward the side opposite to the affected area.5 This syndrome is predominantly encountered in childhood and rarely occurs in adults.5 Neuroimaging evaluation with CT of the cervical spine is essential to confirm the diagnosis. Magnetic resonance imaging offers valuable insights into the severity of lymphadenopathy and provides additional information regarding the condition of the ligaments in the C1-C2 joints.4 It also helps to rule out possible associated deep space infections.
In the case of our patient, GS syndrome developed as a complication of peritonsillar abscess, which is uncommon, being that GS more commonly occurs with retropharyngeal abscesses.6 Her main complaint was progressive neck pain with limited mobility and associated with left facial swelling, with no sore throat, fever or palpable cervical lymph nodes. A negative rapid S. pyogenes test along with unremarkable blood work and no sore throat made the diagnosis of peritonsillar abscess quite challenging. However, persistent pain unresponsive to nonsteroidal anti-inflammatory drugs and muscular relaxants prompted the imaging study to evaluate for an underlying process in the neck. Her initial left facial edema (atypical in peritonsillar abscess) could be explained by edema of the neck fascia in response to inflammation and sternocleidomastoid muscle spasm. Regarding the classification of the GS, Fielding and Hawkins7 proposed a grading scale to guide the choice of treatment and to evaluate prognosis. Types I and II are characterized by absence of neurological impairments and are typically treated conservatively with oral nonsteroidal anti-inflammatory drugs, antibiotics, physical therapy and the use of a soft cervical collar. In contrast, types III and IV are more severe and are characterized by neurological deficits and potentially serious complications, which may require surgical fusion.8 Prompt diagnosis is needed because a delay in recognition increases the risk of neurological complications that may require surgical therapy.9 A good outcome is expected when there is early detection and treatment, as observed in our patient with full recovery.
REFERENCES 1. Bell. The Nervous System of the Human Body. 1830. Available at: http://hdl.handle.net/10713/3152. Accessed November 11, 2023. 2. Grisel P. Enucléation de l’atlas et torcicolis nasopharyngien. Presse Médicale; 1930:50–53 3. Karkos PD, Benton J, Leong SC, et al. Grisel’s syndrome in otolaryngology: a systematic review. Int J Pediatr Otorhinolaryngol. 2007;71:1823–1827. 4. Richter GT, Bower CM. Cervical complications following routine tonsillectomy and adenoidectomy. Curr Opin Otolaryngol Head Neck Surg. 2006;14:375–380. 5. Iaccarino C, Francesca O, Piero S, et al. Grisel’s syndrome: non-traumatic atlantoaxial rotatory subluxation-report of five cases and review of the literature. Acta Neurochir Suppl. 2019;125:279–288. 6. White MD, Hansberry DR, Prabhu AV, et al. Grisel’s syndrome: a rare cause of torticollis with subluxation of the atlantoaxial joint secondary to a retropharyngeal abscess. Interdiscip Neurosurg. 2020;22:1–4. 7. Fielding JW, Hawkins RJ. Atlanto-axial rotatory fixation. (Fixed rotatory subluxation of the atlanto-axial joint). J Bone Joint Surg Am. 1977;59:37–44. 8. Reddy KN, Baig SM, Batra M, et al. Grisel’s syndrome: a case report on this rare pediatric disease and its anesthetic challenges. BMC Anesthesiol. 2020;20:255. 9. Dagtekin A, Kara E, Vayisoglu Y, et al. The importance of early diagnosis and appropriate treatment in Grisel’s syndrome: report of two cases. Turk Neurosurg. 2011;21:680–684.
留言 (0)