
記住我
Over 25 million individuals in the United States (or 8% of the population) are described as having limited English proficiency (LEP), or as speaking English “less than very well.”1 These individuals have long encountered a unique set of challenges when accessing health care. Compared to individuals with English proficiency (EP), LEP individuals have significantly worse access and care, including greater difficulty gaining insurance coverage, being less likely to receive preventive care, and more likely to have preventable emergency department visits.2–4
The COVID-19 pandemic amplified the challenges that many individuals face in accessing health care. The percentage of US adults experiencing delayed or forgone medical care during early in the pandemic was estimated to be between 25% to 40%, compared with 8%–14% before the pandemic.5–13 Postponed or skipped care may increase the risk of morbidity and mortality, particularly among those with chronic health conditions; worsening health conditions can also limit the ability to work or perform other daily activities.9 Reductions in access to care were found to be worse among traditionally underserved populations such as people with disabilities and racial and ethnic minorities.6–8
Previous studies have largely focused on access to medical care, yet the pandemic disrupted all aspects of the health care system. Few studies have explored the extent of delayed and forgone health care across different types of health care services during the pandemic9,10 and none have examined the experiences among individuals with LEP. To address these gaps, we aimed to assess the impact of English language proficiency on delayed and forgone health care across several services (ie, medical, dental, mental health, pharmacy, and home care) during the early COVID-19 pandemic, using a nationally representative sample. Our primary research questions were whether there was an association between English proficiency and delayed and forgone health care; and what factors were associated with delayed and forgone health care among LEP adults. We hypothesized that during the early period of the COVID-19 pandemic, LEP adults had significantly more delayed and forgone health care than English proficiency adults. As a group that has long faced longstanding barriers in accessing care and subsequent disparities in health outcomes, it is important to understand health care access among LEP adults during the pandemic to better develop strategies to address their health care needs in future crises.
METHODS Data and SampleData were from adult respondents to the 2020 National Health Interview Survey (NHIS) collected during July–December 2020. NHIS is a nationally representative, cross-sectional household survey of the civilian, noninstitutionalized US population.14 The COVID-19 pandemic necessitated changes to data collection.15 Interviews were typically conducted in person with a telephone follow-up visit; 2020 interviews were conducted over the telephone first with limited in-person follow-up visits. The 2020 response rate was 48.9% (compared to 59.1% in 2019).15,16 The analytic sample included 16,941 adult respondents aged 18 years and older who were interviewed in the third and fourth quarter of 2020 and had data on all measures of interest. All study variables had <5% missing. This study was determined to be not Human Subjects Research by the Advocate Aurora Health Institutional Review Board.
MeasuresOur main outcomes were 2 dichotomous measures, self-reported delayed and forgone health care. Delayed health care was a composite measure constructed from respondents who answered yes to a delay in medical care, dental care, mental health care, or prescriptions due to cost in the past 12 months or the coronavirus pandemic. Similarly, forgone health care was constructed from respondents who answered yes to not getting medical care, dental care, mental health care, prescriptions, or home care due to cost in the past 12 months or the coronavirus pandemic. Questions related to the pandemic were added in July 2020.15 All questions were asked to all adults except delays in filling prescriptions due to cost was asked only from respondents who had taken prescription medication in the past 12 months. Full question texts can be found in Appendix A, Supplemental Digital Content 1, https://links.lww.com/MLR/C775.
The key independent variable was English proficiency (proficient vs. limited proficiency). Respondents were categorized as limited proficiency if their interview was conducted in Spanish, both English and Spanish, or some other language. Interview language has commonly been used as a proxy for English proficiency in the health care access and utilization literature.11,17
Covariates included demographic, socioeconomic, and health characteristics. Covariates included: race and ethnicity (non-Hispanic White, Hispanic, non-Hispanic Asian, non-Hispanic Other), age (18–44, 45–64, ≥65 years), sex (male, female), education (college degree or higher, some college, high school diploma, less than high school diploma), poverty status [family income <100% of federal poverty level (FPL), 100%–199% FPL, ≥200% FPL], insurance (private, public, uninsured), worked last week (yes, no), and having any one of 6 common chronic conditions (arthritis, cancer, congestive heart disease, diabetes, hypertension, high cholesterol). Respondents were considered to have a usual place of care if they responded to having one or more places. The presence of a disability (yes or no) was included using the Washington Group Short Set Composite Disability Indicator. We did not control for overall health status because the measure has been found to be susceptible to cultural bias among Asian and Latinx populations.18
Statistical AnalysisWe conducted descriptive and multivariate analyses. Descriptive statistics were produced to understand differences in characteristics between LEP and English proficiency groups. We conducted bivariate analyses using χ2 tests to compare the distribution of the outcomes and other characteristics. We then performed 2 analyses using multivariate logistic regression models. The first analysis assessed the association between English proficiency and delayed and forgone health care. In the second analysis, we separately modeled characteristics associated with delayed and forgone health care in the LEP and English proficiency groups.
All analyses were conducted using Stata version 17.0 (Stata Corporation) and used statistical methods to account for the complex survey design (ie, weighting). Two-sided P<0.05 was considered statistically significant.
RESULTS Descriptive CharacteristicsThe 16,941 respondents in our sample represented over 223 million adults nationally. Approximately 7% of respondents, representing over 16 million adults, were identified as LEP. A greater percentage of LEP adults were between 45 and 64 years, were Hispanic or Asian, had less education, were poorer, had public insurance or were uninsured, had not worked last week, and did not have a usual place of care (Table 1). We observed no differences by sex, having a disability, or having one or more chronic conditions.
TABLE 1 - Demographic, Socioeconomic, and Health Characteristics of Adult Respondents in the United States, by English Proficiency, National Health Interview Survey, July–December 2020 Total (N=16,941) English proficient (N=16,257) Limited English proficient* (N=684) % (95% CI) % (95% CI) % (95% CI) P Age P=0.009 18–44 years 45.7 (44.6, 46.9) 45.7 (44.5, 46.9) 45.7 (41.2, 50.2) 45–64 years 32.5 (31.6, 33.4) 32.1 (31.2, 33.1) 37.4 (32.9, 42.1) 65+ years 21.8 (21.0, 22.6) 22.1 (21.3, 23.0) 16.9 (14.0, 20.3) Male 48.2 (47.2, 49.2) 48.3 (47.2, 49.3) 46.8 (42.4, 51.3) P=0.54 Race and ethnicity P<0.001 Non-Hispanic White 63.5 (61.6, 65.4) 68.1 (66.4, 69.7) 1.7 (0.9, 3.1) Hispanic 16.7 (15.1, 18.4) 11.4 (10.3, 12.6) 88.5 (84.6, 91.5) Non-Hispanic Asian 5.9 (5.2, 6.6) 5.6 (5.0, 6.4) 9.0 (6.3, 12.8) Non-Hispanic Other† 14.0 (12.9, 15.1) 14.9 (13.8, 16.1) 0.8 (0.3, 2.1) Education P<0.001 College degree or higher 30.2 (29.1, 31.3) 31.8 (30.7, 32.9) 8.1 (5.9, 10.9) Some college 29.8 (28.8, 30.8) 31.1 (30.1, 32.1) 12.1 (9.4, 15.5) High school diploma 28.9 (27.9, 30.0) 29.0 (27.9, 30.1) 28.3 (24.1, 33.0) Less than high school diploma 11.1 (10.2, 12.1) 8.1 (7.4, 8.9) 51.5 (46.4, 56.5) Poverty status P<0.001 ≥200% FPL 71.5 (70.2, 72.7) 74.3 (73.1, 75.5) 33.5 (29.0, 38.3) 100%–199% FPL 18.3 (17.4, 19.3) 17.1 (16.2, 18.1) 35.0 (30.9, 39.3) <100% FPL 10.2 (9.4, 11.0) 8.6 (7.9, 9.3) 31.5 (27.0, 36.5) Insurance P<0.001 Private 67.1 (65.9, 68.4) 69.8 (68.6, 71.0) 30.1 (25.8, 34.8) Public 21.7 (20.7, 22.7) 21.0 (20.0, 22.0) 31.4 (27.4, 35.7) Uninsured 11.2 (10.3, 12.1) 9.2 (8.4, 10.0) 38.5 (34.1, 43.0) Worked last week P<0.001 Yes 61.3 (60.3, 62.4) 61.9 (60.9, 63.0) 53.2 (48.5, 57.8) No 38.7 (37.6, 39.7) 38.1 (37.0, 39.1) 46.8 (42.2, 51.5) Has a disability 8.2 (7.6, 8.7) 8.1 (7.6, 8.7) 8.6 (6.4, 11.5) P=0.72 Has ≥1 chronic condition 51.5 (50.4, 52.6) 51.7 (50.6, 52.8) 49.2 (44.3, 54.1) P=0.33 Has a usual place of care 89.9 (89.2, 90.6) 90.4 (89.6, 91.1) 84.0 (80.3, 87.2) P<0.001*Respondents with limited English proficiency were identified using the language they used to respond to the survey.
†Non-Hispanic Other includes respondents who self-identified as Black/African American, American Indian/Alaska Native, and other single and multiple races.
FPL indicates federal poverty level.
Data Source: National Center for Health Statistics, National Health Interview Survey, 2020.
LEP and English proficiency adults were markedly different in several demographic and socioeconomic characteristics. Almost all LEP adults were Hispanic (88.5%) or Asian (9.0%) while most English proficiency adults were White (68.1%). LEP adults also had much lower levels of educational attainment and income. More than half of LEP adults (51.5%) had less than a high school diploma, which is more than 6 times greater than English proficiency adults (8.1%). Almost one-third (31.5%) of LEP adults had an income below the FPL compared to only 8.6% of English proficiency adults. In addition, 38.5% of LEP adults were uninsured and 31.4% had public insurance compared to 9.2% and 21.0% of English proficiency adults, respectively. Finally, a smaller percentage of LEP adults reported a usual place of care (84.0%) compared to English proficiency adults (90.4%).
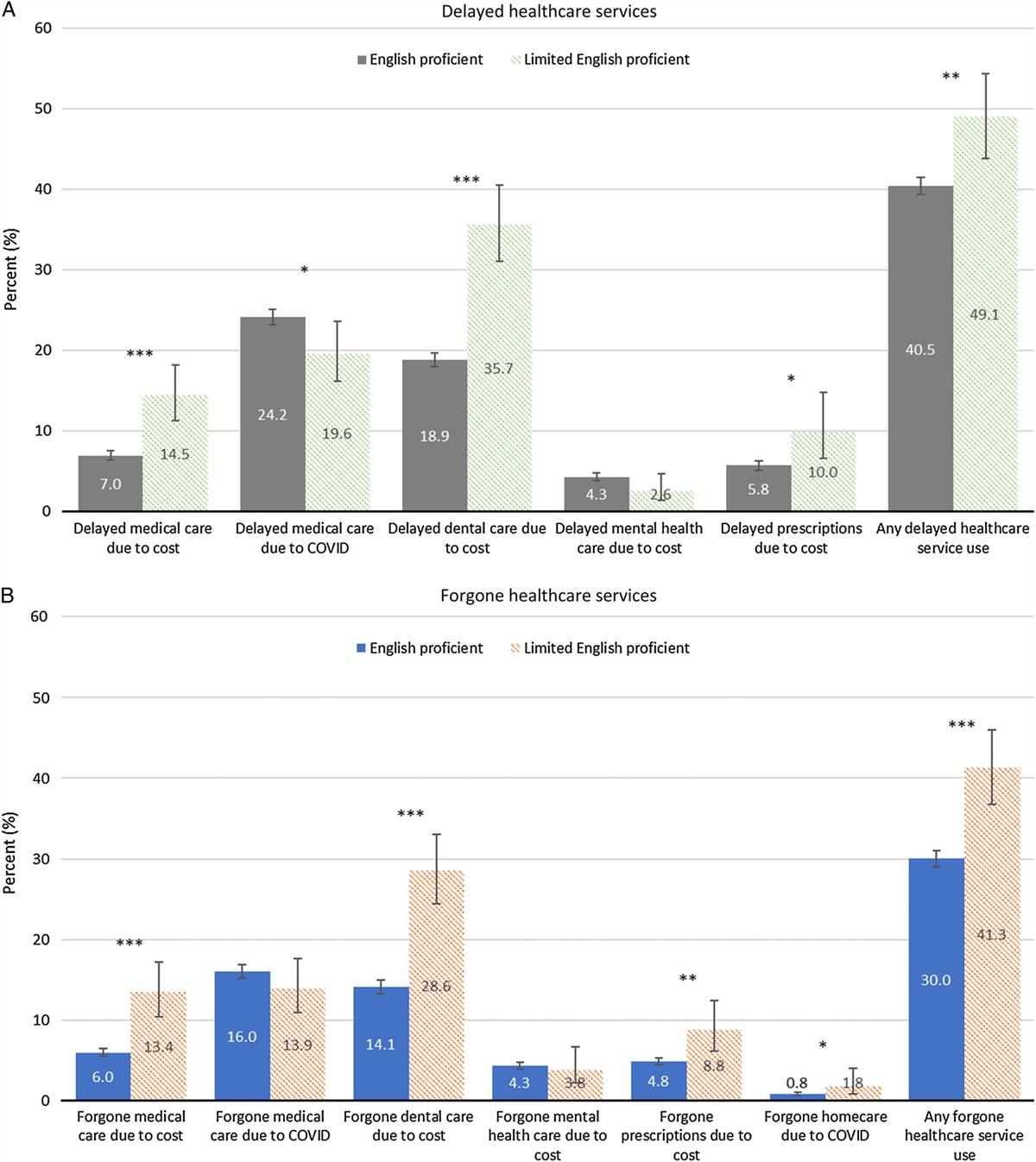
Differences in Delayed and Forgone Health CareIn aggregate, 44.9% of adults reported delaying or forgoing health care during the pandemic (41.1% reported delayed health care and 30.8% reported forgone health care). Descriptive analyses showed many statistically significant differences between LEP and English proficiency adults (54.1% of LEP adults and 44.2% of English proficiency adults reported delaying or forgoing health care, P<0.001). LEP adults reported a significantly higher proportion of both delayed and forgone health care compared to English proficiency adults (delayed: 49.1% and 40.5%, P<0.01; forgone: 41.3% and 30.0%, P<0.001) (Figs. 1A, B). Among specific measures of delayed health care (Fig. 1A), LEP adults were significantly more likely than English proficiency adults to report delays in medical care due to cost (14.5% vs. 7.0%), dental care due to cost (35.7% vs. 18.9%), and prescriptions due to cost (10.0% vs. 5.8%) while LEP adults were significantly less likely than English proficiency adults to report delays in medical care due to the pandemic (19.6% vs. 24.2%). Similarly, LEP adults were also significantly more likely than English proficiency adults to report forgone medical care due to cost, dental care due to cost, prescriptions due to cost, and home care due to the pandemic (Fig. 1B). There were no significant differences between LEP and English proficiency adults reports of forgone medical care due to the pandemic or delayed or forgone mental health care due to cost.
 FIGURE 1:
FIGURE 1: Delayed and forgone health care services, by English proficiency, National Health Interview Survey, July–December 2020. (A) Delayed Health Care Services. (B) Foregone Health Care Services. *P<0.05, **P<0.01, ***P<0.001. Data Source: National Center for Health Statistics, National Health Interview Survey, 2020.
While similar percentages of LEP and English proficiency adults reported delayed medical care (due to costs or the pandemic; 30.1% and 28.5%, P=0.46), a greater percentage of LEP adults reported forgone medical care (23.8% and 19.8%, P=0.04). Reasons for delayed and forgone medical care also differed (Fig. 2). A greater percentage of LEP adults reported cost as the sole reason for delaying (10.5%) and forgoing (9.9%) medical care compared to English proficiency adults (4.3% and 3.8%, respectively). In contrast, a greater proportion of English proficiency adults reported the pandemic as the sole reason for both delaying (21.5% vs. 15.7% for LEP adults) and forgoing medical care (13.8% vs. 10.4%).
 FIGURE 2:
FIGURE 2: Reasons for delayed and forgone medical care, by English proficiency, National Health Interview Survey, July–December 2020. Data Source: National Center for Health Statistics, National Health Interview Survey, 2020.
Unadjusted and Multivariate Associations With Delayed and Forgone Health Care Use for Adults With Limited English ProficiencyTable 2 presents the unadjusted and multivariate associations in delayed and forgone health care by English proficiency. Unadjusted logistic regression showed that compared to English proficiency adults, LEP adults had significantly greater odds of delaying prescriptions, medical care, and dental care because of costs and significantly lower odds of delaying medical care due to the pandemic. This resulted in LEP having greater odds of delaying health care in aggregate [odds ratio (OR)=1.42, 95% CI: 1.14, 1.77). Similar associations were seen in forgone health care; LEP adults had significantly greater odds of forgoing needed health care (OR: 1.64, 95% CI: 1.35, 1.99) due to their greater odds of forgoing medical care, dental care, prescriptions, and home care due to costs. After controlling for demographic, socioeconomic, and health characteristics, the relationships between English proficiency and delayed and forgone health care were no longer statistically significant.
TABLE 2 - Relationship Between Delay and Forgone Health Care Use Outcomes and English Proficiency (Reference English Proficient) Among Adult Respondents, National Health Interview Survey, July–December 2020 Limited English proficient (reference: English proficient), OR (95% CI) Outcome Unadjusted odds ratio Adjusted odds ratio Delayed health care service use 1.42 (1.14, 1.77)** 1.17 (0.89, 1.55) Delayed medical care due to costs 2.26 (1.67, 3.05)*** 1.05 (0.71, 1.55) Delayed medical care due to COVID-19 0.77 (0.60, 0.97)* 1.17 (0.87, 1.56) Delayed dental care due to costs 2.39 (1.92, 2.97)*** 1.09 (0.82, 1.46) Delayed mental health care due to costs 0.59 (0.31, 1.12) 0.65 (0.31, 1.35) Delayed prescriptions due to costs 1.71 (1.07, 2.74)* 0.98 (0.56, 1.73) Forgone health care service use 1.64 (1.35, 1.99)*** 1.16 (0.88, 1.52) Forgone medical care due to costs 2.45 (1.82, 3.31)*** 1.25 (0.85, 1.83) Forgone medical care due to COVID-19 0.85 (0.64, 1.12) 0.91 (0.63, 1.32) Forgone dental care due to costs 2.43 (1.94, 3.05)*** 1.06 (0.79, 1.43) Forgone mental health care due to costs 0.88 (0.48, 1.60) 0.86 (0.43, 1.73) Forgone prescriptions due to costs 1.89 (1.26, 2.83)** 1.12 (0.66, 1.89) Forgone home care due to COVID-19 2.40 (1.02, 5.66)* 1.52 (0.55, 4.24)*P<0.05.
**P<0.01.
***P<0.001.
Adjusted models controlled for race and ethnicity, age, sex, education, poverty status, insurance, employment, disability status, chronic condition, and usual place of care.
OR indicates odds ratio.
Multivariate analyses showed that among LEP adults, insurance, having a disability, and chronic conditions were significantly associated with reports of both delayed and forgone health care (Table 3). Specifically, LEP adults without insurance had greater odds of reporting delayed health care [adjusted odds ratio (aOR): 4.32, 95% CI: 2.39, 7.84] and forgone health care (aOR: 2.98, 95% CI: 1.63, 5.46) than those with private insurance; LEP adults with public insurance also had greater odds of delayed health care (aOR: 2.02, 95% CI: 1.16, 3.53). Similarly, compared to LEP adults without a disability or chronic conditions, LEP adults with a disability and chronic conditions had greater odds of reporting delayed [disability (aOR: 1.92, 95% CI: 1.00, 3.66); chronic conditions (aOR: 2.42, 95% CI: 1.49, 3.93)] and forgone [disability (aOR: 1.85, 95% CI: 1.01, 3.39); chronic conditions (aOR: 3.15, 95% CI: 1.83, 5.41)] health care. In addition, race/ethnicity and age were also associated with reports of any forgone health care among LEP adults. Hispanic (aOR: 6.90, 95% CI: 1.71, 27.86) and Asian (aOR: 6.71; 95% CI: 1.36, 33.18) LEP adults had greater odds of forgoing any health care service use than White, non-Hispanic LEP adults, while adults 65+ years had lower odds than adults 18–44 years (aOR: 0.46; 95% CI: 0.23, 0.94).
TABLE 3 - Adjusted English Proficiency-Specific Associations With Delayed and Forgone Health Care Among Adults, National Health Interview Survey, July–December 2020 Adjusted odds ratio (95% CI) Delay in health care services Forgone health care services Limited English proficient English proficient Limited English proficient English proficient Race and ethnicity Non-Hispanic White Reference Reference Reference Reference Hispanic 0.95 (0.31, 2.90) 0.97 (0.83, 1.13) 6.90 (1.71, 27.86)** 1.07 (0.89, 1.28) Non-Hispanic Asian 1.10 (0.31, 3.97) 0.64 (0.52, 0.79)*** 6.71 (1.36, 33.18)* 0.64 (0.51, 0.80)*** Non-Hispanic Other 0.51 (0.04, 6.91) 0.95 (0.83, 1.09) 2.88 (0.21, 38.94) 1.17 (1.01, 1.35)* Age 18–44 years Reference Reference Reference Reference 45–64 years 1.10 (0.68, 1.79) 1.06 (0.95, 1.18) 1.05 (0.4, 1.74) 0.97 (0.87, 1.09) 65+ years 0.56 (0.28, 1.12) 0.62 (0.53, 0.72)*** 0.46 (0.23, 0.94)* 0.48 (0.41, 0.57)*** Sex Male Reference Reference Reference Reference Female 1.28 (0.85, 1.93) 1.59 (1.46, 1.74)*** 1.31 (0.88, 1.93) 1.54 (1.40, 1.69)*** Education College degree or higher Reference Reference Reference Reference Some college 1.48 (0.63, 3.43) 0.79 (0.71, 0.87)*** 1.29 (0.49, 3.42) 0.94 (0.83, 1.05) High school diploma 0.92 (0.39, 2.13) 0.67 (0.60, 0.75)*** 1.09 (0.45, 2.66) 0.77 (0.67, 0.87)*** Less than high school diploma 0.77 (0.35, 1.67) 0.58 (0.47, 0.71)*** 0.89 (0.37, 2.13) 0.65 (0.53, 0.81)*** Poverty status ≥200% FPL Reference Reference Reference Reference 100%–199% FPL 0.93 (0.56, 1.56) 1.37 (1.20, 1.56)*** 1.06 (0.65, 1.72) 1.64 (1.42, 1.89)*** <100% FPL 1.12 (0.65, 1.94) 1.33 (1.10, 1.59)** 1.54 (0.88, 2.68) 1.51 (1.24, 1.82)*** Insurance Private Reference Reference Reference Reference Public 2.02 (1.16, 3.53)* 1.24 (1.09, 1.41)** 1.22 (0.66, 2.26) 1.34 (1.17, 1.54)*** Not insured 4.32 (2.39, 7.84)*** 2.33 (1.92, 2.82)*** 2.98 (1.63, 5.46)*** 2.37 (1.95, 2.86)*** Worked last week Yes Reference Reference Reference Reference No 0.80 (0.49, 1.28) 0.92 (0.82, 1.03) 0.72 (0.45, 1.16) 0.98 (0.87, 1.11) Disability No disability Reference Reference Reference Reference Has a disability 1.92 (1.00, 3.66)* 1.93 (1.67, 2.22)*** 1.85 (1.01, 3.39)* 2.23 (1.92, 2.59)*** Has ≥1 chronic condition No Reference Reference Reference Reference Yes 2.42 (1.49, 3.93)*** 1.71 (1.53, 1.90)*** 3.15 (1.83, 5.41)*** 1.88 (1.67, 2.12)*** Has a usual place of care Has a usual place of care Reference Reference Reference Reference No usual place of care 1.25 (0.73, 2.13) 1.29 (1.08, 1.54)** 0.97 (0.50, 1.88) 1.25 (1.03, 1.53)**P<0.05.
**P<0.01.
***P<0.00.
FPL indicates federal poverty level.
Data Source: National Center for Health Statistics, National Health Interview Survey, 2020.
Among English proficiency adults, experiencing delayed health care varied across multiple factors. Like LEP adults, English proficiency adults who were uninsured (aOR: 2.33, 95% CI: 1.92, 2.82) or had public insurance (aOR: 1.24, 95% CI: 1.09, 1.41), had a disability (aOR: 1.93, 95% CI: 1.67, 2.22), and one or more chronic conditions (aOR: 1.71, 95% CI: 1.53, 1.90) had greater odds of delaying health care than English proficiency adults who had private insurance, no disabilities, and no chronic conditions, respectively. In addition, English proficiency adults who were Asian (aOR: 0.64, 95% CI: 0.52, 0.79), 65+ years (aOR: 0.62, 95% CI: 0.53, 0.72), and lower education levels had lower odds of delaying health care than their respective English proficiency adult counterparts. In contrast, English proficiency adults who were female (aOR: 1.59, 95% CI: 1.46, 1.74), had lower family income [less than 100% FPL (aOR: 1.33, 95% CI: 1.10, 1.59); between 100% and 199% FPL (aOR: 1.37, 95% CI: 1.20, 1.56)], and did not have a usual place of care (aOR: 1.29, 95% CI: 1.08, 1.54) had greater odds of delaying health care than their respective English proficiency adult counterparts.
The associations in delayed health care for English proficiency adults translated to similar associations in significance, magnitude, and direction to forgone health care for almost all characteristics (Table 3).
DISCUSSIONUsing a nationally representative sample of US adults, this study examined differences in delayed and forgone health care services by English proficiency, early in the COVID-19 pandemic. We found that while 45% of all adults experienced delayed or forgone health care during the period, a significantly greater percentage of LEP adults experienced delayed or forgone health care (54%) compared to English proficiency adults (44%). The differences between the two groups were explained by differences in their health, socioeconomic status, and demographic characteristics. For LEP adults, insurance, health (ie, having a disability or a chronic condition), race and ethnicity, and age were significantly associated with delayed and forgone health care.
The study findings showed that almost half of all adults put off or missed health care during the early period of the COVID-19 pandemic and that the pandemic disproportionately affected LEP adults compared to English proficiency adults. Previous studies examining a range of health care services found that 36%–38% of adults had delayed or forgone health care in 2020.9,10 Our findings are higher than previous reports conducted during this period,
留言 (0)