
記住我


Access to good-quality housing is a foundational social determinant of health, and in the United States, housing instability continues to be a major public health concern.1,2 Housing instability is a broad term referring to people who move frequently, have trouble paying rent, spend the bulk of their income on housing costs, are experiencing overcrowding, or are unhoused entirely.3 There are certain populations that are at increased risk of experiencing housing instability, including young adults,4 veterans,5 and members of the Lesbian, Gay, Bisexual, Transgender, Queer, and more community as a result of discrimination, economic instability, and trauma.6
Individuals with housing instability are at risk for numerous health conditions and are hospitalized at a higher rate than the general population, especially in acute care and psychiatric settings.7,8 Not only are individuals with housing instability 1.7–2 times more likely to use hospital services than housed patients,9 this population also experiences higher rates of hospital readmission,10 longer hospital stays,11 and, therefore, higher associated hospital spending when compared with housed individuals.12 Recognition of the critical relationship between housing and health has led to the development of targeted health care services for individuals with housing instability and greater cross-sector collaborations between health care, public health, and community-based organizations to improve housing and overall population health.
A well-established body of literature that spans more than a half-century succinctly describes the so-called “neighborhood effect,” which outlines the critical impacts that housing-related factors have on individual health.13 This term encompasses housing instability, concentrated poverty, racial segregation, violence, trauma, and poorly performing schools, all of which have deleterious effects on social mobility and in turn, intergenerational poverty.14,15 Neighborhood factors have been associated with a broad range of health conditions, including hypertension and chronic disease, child development disorders, and mental health.16–19 Neighborhood-level social determinants of health have been demonstrated to decrease the efficacy of medical treatment and result in substantial disparities in health outcomes.20–22 As a result of growing costs associated with housing and other social determinants of health, health care systems are increasingly motivated to identify effective interventions as part of their formal service lines, charitable investments, and initiatives to improve population health.9,23
Approximately two thirds of hospitals in the United States are 501(c)(3) nonprofit organizations and are legally required to address substantial health needs in their communities as a condition for tax exemption. The Patient Protection and Affordable Care Act (ACA) introduced additional requirements for these organizations to complete a triennial Community Health Needs Assessment (CHNA) and corresponding implementation strategy (IS). In the IS, hospitals commit to addressing a subset of the most pressing needs with targeted investments and programs.24 This legislation required cross-collaboration between hospitals and their communities, inviting input from public health departments, community-based organizations, and local community members to identify and address priority health needs.25 Although hospitals traditionally met their community benefit requirements through the provision of free or reduced-cost clinical services for community members, the ACA encouraged hospitals to consider the impact of upstream social determinants of health, such as housing, on population health.
In the last decade, a new body of literature has developed, tracking hospital investments in population health improvement using hospital administrative reports and other public sources. Several national studies using Schedule H from hospital tax reports have demonstrated that community benefit spending did not increase significantly after new reporting requirements were added with the ACA. Most importantly, these studies suggest that the vast majority of community benefit dollars go toward unreimbursed care, rather than investments in community health improvement, which includes housing.26,27
Using a combination of CHNAs, ISs, and tax documents, one housing-focused study looked at hospitals in 5 communities with significant housing needs, finding that only 15% of hospital organizations addressed housing as part of their community benefit responsibilities.28 Another study used news articles and press releases to quantify the amount that health systems nationally are investing in social determinants of health, finding that between 2017 and 2019, 2.5 billion health system dollars were invested, of which 1.6 billion dollars were housing-specific.29 Published case studies additionally show targeted innovative hospital investments related to housing, including some that have demonstrated meaningful improvements in health outcomes. Published case studies additionally show targeted innovative hospital investments related to housing, including some that have demonstrated meaningful improvements in health outcomes. In 2018, a study conducted by Nationwide Children’s Hospital considered a nearby neighborhood as the “patient” and the “neighborhood effects” as the symptoms, of which housing instability was the most prominent. The hospital partnered with a local church to form an initiative focused on supporting home repairs, increasing rates of home ownership, constructing new affordable homes, and rental housing development. This initiative demonstrated a positive impact on housing instability, including improved quality of life among residents and reduced home vacancy rates in the neighborhood.14
Other hospitals and health care systems have integrated housing services as part of their formal service provision by establishing medical respite centers and facilitating rapid access to housing. Medical respite centers are acute and postacute care centers for individuals with housing instability. These facilities have been shown to decrease hospital admissions and medical costs among individuals with housing insecurity.30 In addition, rapid access to housing may be an important model for health care organizations to improve patient outcomes and mitigate hospital admissions from individuals with housing instability.31
Although the body of research on hospital investments in housing is growing, gaps in the literature remain, including a national overview of hospital investments to improve housing using the most recent round of published CHNAs and ISs. This approach is critical to capture the current programs that hospitals are using to assess housing needs in their community so that a national baseline can be created to establish hospital trends in addressing housing instability. In this study, we assessed the prevalence of hospital-based programs to address housing-related needs, categorized the specific actions taken to address housing, and determined organizational and community-level factors associated with investing in housing.
METHODS Data and SampleThis retrospective, cross-sectional study examined a nationally representative dataset of administrative documents from nonprofit hospitals that addressed social determinants of health in their federally mandated community benefit implementation plans. Specifically, we analyzed a national dataset of nonprofit hospital CHNAs and ISs. The over 600 nonprofit hospitals represented within the primary dataset that our team constructed were initially sampled from the 2015 American Hospital Association (AHA) Annual Survey. This database is updated annually and contains organizational characteristics on the entire universe of hospitals nationally and additional information that hospitals voluntarily report on their programs and services via survey. Stratifying by state, we included a random sample of 20% of all US general nonprofit community hospitals within each US state, excluding children’s, specialty, and long-term or rehabilitation hospitals, rounding up to the nearest whole number of hospitals to create our dataset (n = 613).
We collected and coded data from the sampled hospitals’ CHNAs and ISs, to identify the most common categories of health needs that hospitals identified in their surrounding community (eg, mental health, substance use, social determinants of health), and whether each of these needs were addressed in the corresponding IS.25 The primary dataset contains 2 waves of hospitals’ community benefit reporting data (2015–2018 and 2019–2021), which is supplemented with organizational characteristics from the 2018 AHA Annual Survey Database.32
We next created a secondary dataset that contained all hospitals from the primary dataset that had developed at least 1 program to address social determinants of health (SDOH) in their IS. For each hospital in this category, we added each specific strategy they adopted to address social determinants of health and the associated goal/objective, evaluation plan, and anticipated impact, if available. A team of coders reviewed each SDOH strategy and coded dichotomously (yes/no) whether each SDOH strategy addressed housing specifically. To assess whether a strategy addressed housing, the coders looked for keywords such as house, home, housing, or homelessness. Coders also read the full strategy to ascertain whether hospitals were addressing housing using other language, such as residence or dwelling.
We merged data on hospital and community characteristics to our dataset of housing strategies. Data on hospital characteristics came from the 2018 AHA Annual Survey,32 along with data on county characteristics from the 2020-2021 Area Health Resource File33 and 2018 County Health Rankings.34 From AHA, we utilized data on the total number of hospital beds, major teaching status, whether the hospital specializes in pediatrics (ie, a children’s hospital), and system membership status.
From the Area Health Resource File, we included the county rural classification. From the County Health Rankings data, we included the percentage of the county reporting severe housing problems over a 5-year average, as well as a measure of income inequality. Severe housing problems are defined as the percentage of households with at least 1 of 4 housing problems: overcrowding, defined as >1 person per room; high housing costs, defined as monthly housing costs that exceed 50% of income; lack of kitchen facilities, defined as a housing unit without a sink with running water, a stove, or a refrigerator; or lack of plumbing facilities, defined as a housing unit without hot and cold water, a toilet, or a bathtub/shower. The measure of income inequality is a ratio of income at the 80th percentile to income at the 20th percentile in a county. After excluding hospitals that did not provide either their CHNA or IS (n = 79), noncommunity hospitals, and hospitals where no community-level data were available, we had 433 hospitals in the analytic sample.
Analytic StrategyOnce all housing strategies were isolated in the dataset, we first used an inductive approach to sort these programs into distinct categories. The inductive approach was undertaken by 7 members of the research team who independently reviewed the housing strategies and then met to group the strategies based on common approaches and/or focus areas. Inductive coding of housing strategies resulted in 7 distinct categories (see Table 1 for definitions and examples in each category): (1) Collaboration with community and hospital-based partners to increase access to affordable housing initiatives, housing assistance, and employment for low-income residents. (2) Utilization of various assessment, screening, and reporting methods to serve as preventative measures for homelessness and housing instability. (3) Implementation of medical respite centers to provide temporary shelter for homeless individuals, thereby bridging the gap between acute care and long-term health maintenance. (4) Employment of intermediary groups and virtual tools to connect homeless patients with identified resources upon discharge. (5) Address specific needs of unhoused populations including educational programming, food and water insecurity, vaccines, employment, and clothing. (6) Extension of financial assistance by hospitals and partners for temporary and transitional housing. (7) Focusing preventive investments on specific populations at increased risk of housing instability (Veterans, Lesbian, Gay, Bisexual, Transgender, Queer, and more, youth, and elderly).
TABLE 1 - Housing Strategy Categories Derived From Housing Strategies Dataset Category Category description Example 1 Example 2 Example 3 Community partner collaboration Collaboration with community-based and hospital-based partners to increase access to affordable housing initiatives, housing assistance, and employment for low-income residents Work with community partners such as social services, health department, homeless shelters, Salvation Army, Habitat for Humanity, to establish referral patterns to address food insecurity, housing and transportation needs (FirstHealth Moore Regional Hospital) Participate in state and local coalitions addressing housing insecurity (Avista Adventist Hospital) Partner with Impact NW to connect families in need to appropriate housing resources through the Community Resource Desks (Providence Portland Medical Center) SDOH screenings Utilization of various assessment, screening, and reporting methods to serve as preventative measures for homelessness and housing instability Provide screening for patients to identify housing insecurity (Mount Auburn Hospital) Conduct housing insecurity screen with all incoming hospital patients in NYC (NYU Winthrop Hospital) Support the implementation of SDOH screening and referral for Gundersen Health System patients and families (Gundersen Lutheran Medical Center) Medical respite centers Implementation of medical respite centers to provide temporary shelter for homeless individuals, bridging the gap between acute care and long-term health maintenance In partnership with the Fresno Rescue Mission, CMC provides homeless patients with a safe place for recovery upon discharge. Patients at the Fresno Medical Respite Center receive health care, social services, and access to other community resources. Respite Center funding serves patients from all Fresno hospitals. In FY 2018, the Respite Center provided services to 330 patients (Community Regional Medical Center). Improve the infrastructure of available recuperative care/temporary shelter for homeless patients that are not medically stable enough to be discharged back to the streets (Providence Holy Cross Medical Center) Catholic Charities will provide short-term emergency shelter and case management for medically fragile homeless patients upon hospital discharge (Scripps Green Hospital) Community SDOH liaison Employment of intermediary groups and virtual tools to connect homeless patients with identified resources upon discharge Support outreach, navigation, and case management that connects individuals to coordinated entry services (Kaiser Permanente Antioch Medical Center) The Community Health Navigator will follow up with homeless persons who seek care in the ER but are not admitted to the hospital. The Community Health Navigator will provide connections to social service agencies (Saint Bernardine Medical Center) Develop and implement a community health worker (CHW) pilot program in 2 low-income apartment buildings in CD 3 and explore expansion to other locations in Brooklyn (New York University Langone Hospital - Brooklyn) Address specific needs of homeless populations Address specific needs of houseless populations including educational programming, food and water insecurity, vaccines, employment, and clothing Daily Meal Service 365 days/year for Brother Francis Emergency Homeless Shelter guests (Providence Alaska Medical Center) Build one new community water kiosk by the end of year 3 (Manchester Memorial Hospital) Provide individuals with care packets to include health information, wound care supplies and other personal care essentials (Holyoke Medical Center) Financial assistance Extension of financial assistance by hospitals and partners for temporary and transitional housing Provide grant support to community service agencies that address the multiple health and social needs of persons experiencing homelessness. (Marina Del Rey Hospital) Invest in community and hospital-based strategies (eg, housing navigators, behavioral health supports and case managers, integrated systems of care and community building) to support community members who are homeless or at risk of homelessness in their effort to search, apply for and secure affordable housing (Boston Children’s Hospital) Invests in organizations, programs, and initiatives that work to address housing and homelessness. Oakland Cabin Communities is one example of an initiative within the hospital service area that provides temporary housing to homeless residents and supports their transition to permanent or transitional housing (Alta Bates Summit Medical Center - Summit Campus (ABSMC) Targeting high-risk populations Focusing SDOH housing efforts to specifically target high-risk populations (Veterans, LGBTQ+, Youth, Elderly) Implement Community Solutions’ Built for Zero to address chronic and veteran homelessness (Kaiser Permanente San Rafael Medical Center) Support RYSE, a youth‐specific shelter on O’ahu, providing assistance to help homeless youth achieve housing and self‐sufficiency (Straub Clinic and Hospital) Improve infrastructure to serve LGBTQ+ patients and address disparities through provider training and adequate data collection (Queen of the Valley Medical Center)Categories were determined based upon a group analysis of the entire housing strategies dataset. Three examples of each category are listed to represent reliability in the interpretation of each strategy.
LGBTQ+ indicates Lesbian, Gay, Bisexual, Transgender, Queer, and more; SDOH, social determinants of health.
The next step involved assigning each housing program to 1 of the 7 categories. To ensure reliability, 7 members of the research team reviewed the first 10 housing strategies and independently coded for alignment with 1 of the 7 emergent categories. The coding team reached 100% consensus after initial training and discussion of categories. Four members of the team subsequently evaluated the remaining housing strategies to sort them into each category. We excluded hospitals that listed goals but no specific strategies from the data analysis. Hospital ISs listed broader goals, with a further breakdown into specific strategies as to how the mentioned goal would be implemented. Twenty-four hospitals provided broad goals related to housing with no further classification of how they would implement a strategy to address this goal and were excluded. Only hospitals that included specific strategies to address housing were included in the final categorization.
We computed descriptive statistics to examine hospital and community characteristics associated with hospital housing strategies. We used t tests and χ2 analysis to assess significant differences between these characteristics among hospitals that do and don’t address housing in their documents. We also used multivariable logistic regression to examine what hospital and community characteristics were associated with hospitals addressing housing in their documents. On the basis of prior literature, we included both organizational-level and county-level variables and regions that have been significantly associated with hospital community benefit investments in previous studies.28,35,36 Our regression model included bed size, major teaching hospital status, children’s hospital status, rural county status, severe housing problem, income inequality, and region. We included all covariates in a single model and excluded income inequality due to a high variance inflation factor, indicating multicollinearity.
RESULTSFrom this analytic sample of 433 hospitals, 80% of hospitals did not address the housing needs of their community within their IS. Of the remaining 20% (87) of hospitals that did address the housing needs of their community, 6.68% (29) documented only 1 strategy regarding housing needs. The 87 hospitals that address housing needs within their implementation strategies put forward a cumulative total of 302 specific strategies to address housing insecurity.
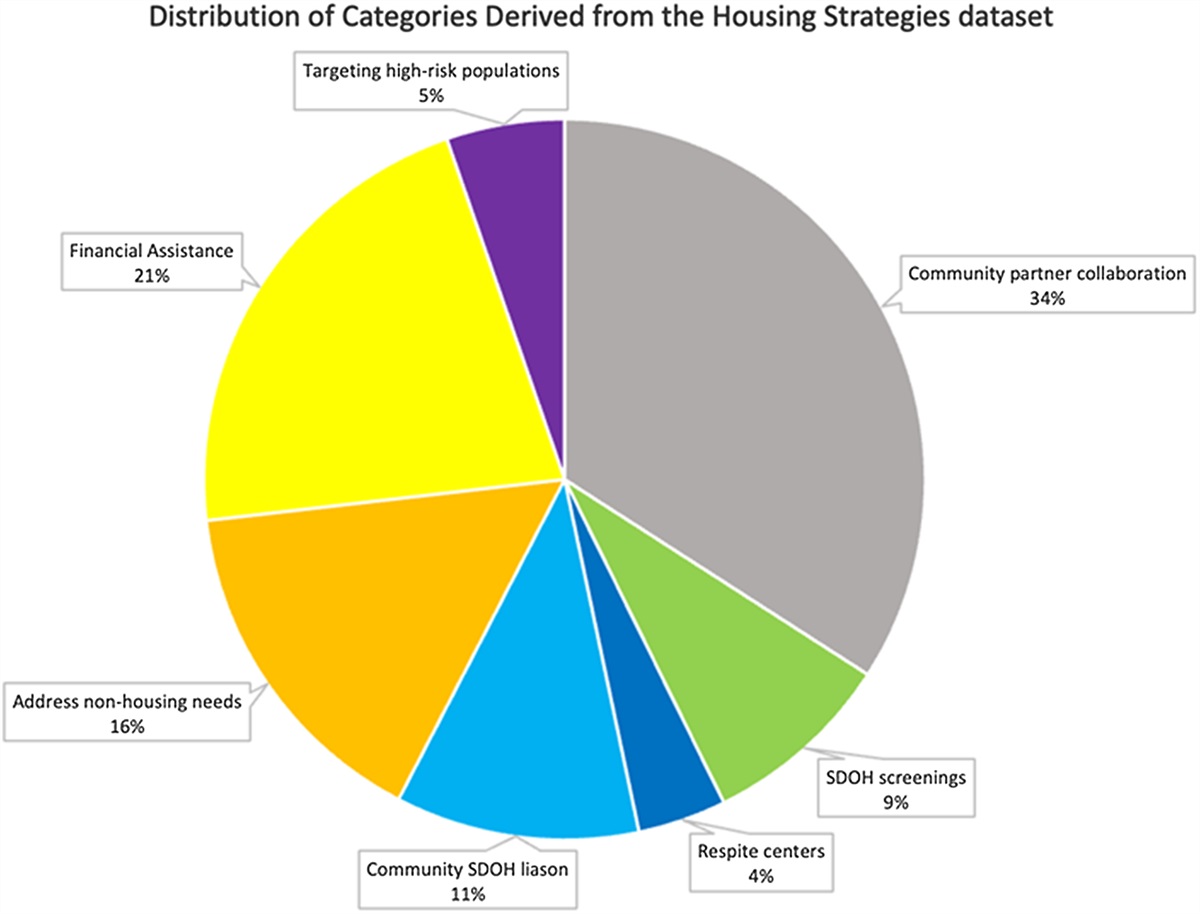
The most common strategy that hospitals utilized to address housing needs was community collaboration (Fig. 1) (see Supplemental Digital Content 1, https://links.lww.com/MLR/C803, which demonstrates the frequency of hospitals by hospital housing strategies). One hundred three (34%) hospitals utilized community collaboration. One example of this strategy mentioned by a hospital is “Working with community partners such as social services, health department, homeless shelters, Salvation Army, Habitat for Humanity, to establish referral patterns to address food insecurity, housing and transportation needs.”—FirstHealth Moore Regional Hospital (See Table 1 for examples from each category).
 FIGURE 1:
FIGURE 1: Distribution of housing strategy categories from housing strategy dataset. Pie graph distribution of how hospitals are addressing housing needs of homeless populations. Community partner collaboration was the most common approach to addressing housing needs, followed by financial assistance and addressing nonhousing needs. Of the 302 specific strategies, 103 were related to “Community Partner Collaboration,” 26 were related to “SDOH Screenings,” 12 were related to “Respite Centers,” 33 were related to “Community SDOH Liaison,” 47 were related to “Address Nonhousing Needs,” 65 were related to “Financial Assistance,” and 16 were related to “Targeting High-risk Populations.” SDOH indicates social determinants of health.
The second most common approach was the extension of financial assistance for temporary and transitional housing, with 65 (21%) of 302 strategies utilizing this approach (Fig. 1). One example of this solution came from Boston Children’s Hospital. Their IS was to “invest in community and hospital-based strategies (e.g., housing navigators, behavioral health supports and case managers, integrated systems of care and community building) to support community members who are homeless or at risk of homelessness, in their effort to search, apply for and secure affordable housing.” The least common route for addressing houseless citizens’ needs was through the implementation of respite centers, which provide temporary housing for those in need to help bridge the gap from acute to long-term care.
Descriptive ResultsHospitals that addressed housing in their IS were larger on average, less likely to be located in rural communities, more likely to be academic medical centers, more likely to be in communities with high-income inequality, and more likely to be serving populations with greater housing needs. The communities in which hospitals addressed housing had an average of 21.06% of their population facing severe housing problems, as compared with 16.01% of the population in communities where hospitals did not invest in housing. Only 3.7% of rural hospitals addressed housing. This is in contrast to nonrural hospitals of which 22.43% addressed housing. In communities where hospitals addressed housing, the average income inequality ratio was 5.01 compared with 4.61 in communities where hospitals did not address housing (Table 2).
TABLE 2 - Descriptive Statistics of Full Sample and Subgroups, With Tests for Significance Between Groups Variable Total sample (%) Hospital addressed housing (%) Hospital did not address housing (%) P n 433 87 346 — Mean percent county severe housing problem 17.15 (4.35–39.41) 21.06 16.16 0.000 Mean income inequality score 4.69 (2.95–9.15) 5.01 4.60 0.000 Mean hospital beds 244.73 (4–2875) 339 221 0.003 County rural location — — — 0.001 Yes 54 (12.74) 3.70 96.30 — No 379 (87.53) 22.43 77.57 — Hospital major teaching — — — 0.000 Yes 50 (11.55) 42.00 58.00 — No 383 (88.45) 17.23 82.77 — Children’s hospital — — — 0.818 Yes 18 (4.16) 22.22 77.78 — No 415 (95.84) 20.00 80.00 — Region — — — — Northeast 90 (20.79) 22.22 77.78 0.571 Midwest 150 (34.64) 7.33 92.67 0.000 South 93 (21.48) 11.83 88.17 0.025 West 100 (23.09) 45.00 55.00 0.000Logistic regression results indicated significant associations between several factors and housing investments, even after controlling for covariates (Table 3). Hospitals that were major teaching centers (odds ratio: 3.86; CI: 1.64–9.13) and hospitals in the Western region of the U.S. (odds ratio: 3.91; CI: 1.87–8.18) had higher odds of addressing housing.
TABLE 3 - Association of Hospital and Community Characteristics With Housing Investments OR SE P>z 95% CI Bed size <50 beds Reference Reference Reference Reference Reference Bed size 50-199 1.15 0.49 0.748 0.50 2.63 Bed size 200-399 1.24 0.57 0.643 0.50 3.06 Bed size 400+ 1.24 0.62 0.677 0.46 3.31 Major teaching hospital 3.86 1.70 0.002 1.64 9.13 Children’s hospital 0.75 0.48 0.648 0.22 2.60 County rural location 0.22 0.17 0.054 0.05 1.03 Severe housing problem 1.04 0.03 0.147 0.99 1.10 Northeast Reference Reference Reference Reference Reference Midwest 0.45 0.20 0.069 0.20 1.06 South 0.63 0.28 0.294 0.27 1.49 West 3.91 1.47 0.000 1.87 8.18The goals of this study were to assess the extent to which hospitals are addressing housing-related needs in their communities, to understand what strategies they use when doing so, and determine what factors are associated with hospitals undertaking this work. We found that hospitals are more likely to address housing-related needs in communities where severe housing problems are more common. This finding suggests that, at least for housing, hospitals are making charitable investments in ways that are in alignment with local needs. For example, Boston Children’s Hospital placed an emphasis on financial assistance to those who were already housing insecure to prevent further displacement, revealing the close link between housing instability and homelessness. Previous studies on hospital community benefits suggest that there is variation in the extent to which investments match the needs that communities identify.23,37
Hospitals also addressed housing more often in urban communities, as well as in the western region of the United States. Urban communities are typically home to larger hospitals or major teaching hospitals, which may be better positioned to obtain funding or federal grants than smaller hospitals with fewer resources for research and outreach. Studies on hospitals and community health have demonstrated that resources available to hospitals are directly linked to the ability of the hospital to address SDOH. Teaching hospitals and universities have supported SDOH evaluation, as student volunteers are available to assist in community health programs, such as free clinics and mobile health clinics. A study on mobile health clinics found that 24% of reporting clinics were affiliated with a university, and 38% of clinics reported targeting homeless populations.28 Severe housing needs are a critical SDOH, regardless of their location in urban or rural settings. Our study and others suggest that rural communities may have less access to hospital-supported programs to address SDOH.
Income inequality was higher in communities where hospitals made housing investments. We suspect this finding may be driven by income inequality in urban areas. This supports previous research, which suggests that income inequality is associated with higher housing costs and limited affordable rental options in the housing market.38,39 These findings suggest that addressing housing may be one important strategy to mitigate the poor health outcomes associated with income inequality.40,41 Importantly, hospitals seem to be responding to housing insecurity more often in their surrounding communities when income inequality is greater.
Finally, the SDOH screenings category was one of the least frequently utilized categories but perhaps one of the most actionable. With research demonstrating that screening for social determinants of health can improve outcomes by identifying increased risk factors for chronic disease, such as housing instability,42 some hospitals have begun to implement universal screening. For example, New York Presbyterian Hospital implemented SDOH screenings that yielded increased nutritional services referrals for those found to be food insecure to improve overall dietary intake.43 Beginning in 2024, the Center for Medicare and Medicaid Services will require hospitals to report the percentage of patients screened for health-related social needs, including housing status.44 Yet, studies suggest that important documentation and workflow barriers exist that limit the uptake of screening currently.45 As a result, SDOH screening is not yet common practice,46,47 which aligns with the results of our study.
Instead, the most frequently addressed housing category was collaboration with community and hospital-based partners to increase access to affordable housing initiatives, housing assistance, and employment for low-income residents. Speculating as to why this category was most consistently addressed, we concluded that it was the broadest category in terms of partnerships, creating more flexibility in strategy. Furthermore, strategies under this category may allow hospitals to work with community organizations that have prior expertise and funding in housing, providing hospitals with a foundation upon which to build their own programs.
LimitationsOf the hospitals that documented housing strategies, the majority only had 1 program related to housing. A few hospitals contained numerous categories, all of which were counted in our sample size. Due to this, a potential limitation is that the few hospitals that provided multiple housing strategies had a larger influence on our dataset than hospitals that provided only 1 strategy. In addition, not all hospitals had detailed strategies listed in their IS, requiring the group to reach consensus on categorization. Although this process has been used successfully in other studies of CHNAs,36 additional detail on hospital programs in their IS would aid further research efforts. Hospitals that were missing CHNA/IS data may also have been unique in some ways; thus, we may be missing a subset of hospitals in our analysis of housing strategies. We also included children’s hospitals in our data collection, which serve different patient populations than most hospitals.
Future research should include in-depth interviews with hospital leaders to better understand the factors, decisions, and program designs created to address housing instability. Research should also assess hospitals’ compliance with their IS, as well as determine whether their programs are successful. Future work could also analyze rural versus urban differences in the types of housing strategies, the funding allocated for housing needs by the hospital, whether there are formal evaluation plans, and how effective each of the various interventions was on improving housing-related needs.
CONCLUSIONSHousing insecurity continues to be a critical issue in the United States and is closely tied to the overall health of communities. It also puts a significant strain on the US health care system, given the increased care needs among individuals experiencing housing insecurity. Understanding the way hospitals currently address housing insecurity is an important step toward developing effective interventions. Currently, only a subset of hospitals nationally are addressing housing; and of those that do, most utilize community-based partnerships. Hospitals addressing housing-related needs were located in more urban areas and served populations with more significant housing needs, suggesting that certain populations may not have access to hospital-supported housing interventions. Future work should focus on supporting cross-sector partnerships and the integration of SDOH into hospitals’ community health programming.
REFERENCES 1. Tsai J. Lifetime and 1-year prevalence of homelessness in the US population: results from the National Epidemiologic Survey on Alcohol and Related Conditions-III. J Public Health (Bangkok). 2018;40:65–74. 2. Taylor LA Housing And Health: An Overview Of The Literature | Health Affairs. Accessed October 24, 2023. https://www.healthaffairs.org/do/10.1377/hpb20180313.396577/ 3. Kushel MB, Gupta R, Gee L, et al. Housing instability and food insecurity as barriers to health care among low-income Americans. J Gen Intern Med. 2006;21:71–77. 4. Loschiavo C, Krause KD, Singer SN, et al. The confluence of housing instability and psychosocial, mental, and physical health in sexual minority young adults: the P18 cohort study. J Health Care Poor Underserved. 2020;31:1693. 5. Tsai J, Szymkowiak D, Jutkowitz E. Developing an operational definition of housing instability and homelessness in Veterans Health Administration’s medical records. PLoS One. 2022;17:e0279973. 6. Bhat AC, Almeida DM, Fenelon A, et al. A longitudinal analysis of the relationship between housing insecurity and physical health among midlife and aging adults in the United States. SSM Popul Health. 2022;18:101128. 7. Franco A, Meldrum J, Ngaruiya C. Identifying homeless population needs in the Emergency Department using Community-Based Participatory Research. BMC Health Serv Res. 2021;21:1–11. 8. Martell JV, Seitz RS, Harada JK, et al. Hospitalization in an urban homeless population: the honolulu urban homeless project. Ann Intern Med. 1992;116:299–303. 9. Butler SM. Can hospitals help create healthy neighborhoods? JAMA. 2015;314:2494–2495. 10. Khatana SAM, Wadhera RK, Choi E, et al. Association of homelessness with hospital readmissions—an analysis of three large states. J Gen Intern Med. 2020;35:2576. 11. Wadhera RK, Choi E, Shen C, et al. Trends, causes, and outcomes of hospitalizations for homeless individuals: a retrospective cohort study. Med Care. 2019;57:21. 12. Koh KA, Racine M, Gaeta JM, et al. Health care spending and use among people experiencing unstable housing in the era of accountable care organizations. Health Aff. 2020;39:214–223. 13. Orum AM. The Wiley Blackwell Encyclopedia of Urban and Regional Studies. The Wiley Blackwell Encyclopedia of Urban and Regional Studies; 2019. 14. Kelleher K, Reece J, Sandel M. The healthy neighborhood, healthy families initiative. Pediatrics. 2018;142:20180261. 15. George C Galster. How Neighborhoods Affect Health, Well-Being, and Young People’s Futures.; 2014. Accessed May 23, 2023. https://www.macfound.org/media/files/hhm-neighborhoods_affect_health_well-being_young_peoples_futures.pdf 16. Ellen IG, Mijanovich T, Dillman KN. Neighborhood effects on health: exploring the links and assessing the evidence. J Urban Aff. 2016;23:391–408. 17. Leventhal T, Brooks-Gunn J. Moving to opportunity: an experimental study of neighborhood effects on mental health. Am J Public Health. 2011;93:1576–1582. 18. Minh A, Muhajarine N, Janus M, et al. A review of neighborhood effects and early child development: how, where, and for whom, do neighborhoods matter? Health Place. 2017;46:155–174. 19. Mujahid MS, Roux VD, Morenoff JD, et al. Neighborhood characteristics and hypertension. Epidemiology. 2008;19:590–598. 20. Does housing mobility policy improve health? - Database of Abstracts of Reviews of Effects (DARE): Quality-assessed Reviews - NCBI Bookshelf. Accessed May 23, 2023. https://www.ncbi.nlm.nih.gov/books/NBK70670/ 21. Morton SMB, Atatoa carr PE, Grant CC, et al. Cohort profile: growing up in New Zealand. Int J Epidemiol. 2013;42:65–75. 22. Molnar BE, Gortmaker SL, Bull FC, et al. Unsafe to play? Neighborhood disorder and lack of safety predict reduced physical activity among urban children and adolescents. Am J Health Promot. 2004;18:378–386.
留言 (0)