
記住我

In this prospective study, girls who were referred to our department for appearance of breast enlargement before the age of 8 years were recruited consecutively between May 2019 and January 2022.
Inclusion criteria were having a complaint of breast development noticed before 8 years of age, determination of glandular or lipoid breast enlargement on physical examination, and giving consent for inclusion in the study. Patients who clearly had palpable glandular breast tissue on physical examination formed one group (n = 100); patients who had the appearance of breast enlargement but had softer consistency on palpation hence were judged to have predominantly lipomastia formed the second group (n = 25) (Fig. 1). None of the patients had neurological signs or symptoms or known CNS pathology (except for one girl with spina bifida). Diagnostic evaluation was performed in University Hospital Pediatric Endocrinology Clinic by experienced board-certified pediatric endocrinologists (D.H., A.B., T.G., S.T., and B.G.T.), with experience ranging from 5 to 27 years and included measurements of height and weight, body mass index, physical examination with Tanner staging, bone age assessment, measurement of basal serum follicle stimulating hormone (FSH), luteinizing hormone (LH) and estradiol concentrations, and uterine and ovarian measurements by pelvic US. Pubertal development was staged according to the Marshall and Tanner criteria [13]. Palpable breast budding in at least one breast was considered Tanner stage 2 breast development. Both breasts were staged separately in each patient and in case of asymmetric breast development, the value for the more developed breast was taken and used in the calculations. Height and weight were measured using a Harpenden stadiometer (Holtain Ltd. Crosswell, Crymyh Pembs UK). Body mass index was calculated using the standard formula (weight in kg/height in m2), and the respective standard deviation scores (SDS) were calculated, based on local reference data [14,15,16]. Bone age was assessed from radiographs of the left hand, according to the method of Greulich and Pyle [17]. Bone age to chronological age ratio was calculated for each patient. Fasting venous blood samples were obtained from all girls in the morning for FSH, LH, and estradiol measurements using semi-automated chemiluminescence methods. In patients with basal LH < 0.6 mIU/mL, a GnRH stimulation test was performed.
Fig. 1
Study outline. CPP central precocious puberty, PE + physical examination confirmed palpable glandular breast development on physical examination, PE- physical examination did not confirm palpable glandular breast development on physical examination, US + ultrasound evaluation confirmed glandular breast development, US- ultrasound evaluation did not confirm glandular breast development
The criteria for the diagnosis of central precocious puberty were (1) progressive breast development starting before 8 years of age, associated with accelerated growth (> 6 cm/year) and skeletal maturation (advanced by at least 1 year) [18]; and (2) a basal LH > 0.6 mIU/mL or a GnRH-stimulated LH of at least 5 mIU/mL [4, 18,19,20,21,22,23,24] as accepted previously in the literature and consensus papers. Uterine length > 34 mm and ovarian volume > 2 cubic centimeters (cc) were taken as supportive criteria [4, 25, 26].
Breast US and shear-wave US elastography were performed in the Radiology Department in a supine position using an Acuson S2000 device (Siemens Healthineers, Erlangen, Germany) with a 9L4 linear array probe (4–9 MHz operating range) by a single board-certified radiologist (E.B.) who has 7 years of experience in evaluating pediatric endocrinology patients. The operator was blinded to the clinical information of the patients.
Breast development evident by US examination was graded according to the system proposed by Garcia et al. [5] who described five morphological stages of glandular development associated with conventional Tanner stages of breast development. These are:
Tanner stage 1, US stage I—US scan shows ill-defined hyperechoic retroareolar tissue.
Tanner stage 2, US stage II—US scan shows a hyperechoic retroareolar nodule with a central hypoechoic area that represents mostly simple branched ducts.
Tanner stage 3, US stage III—US scan shows hyperechoic glandular tissue extending away from the retroareolar area and a central spider-shaped hypoechoic retroareolar region.
Tanner stage 4, US stage IV—US scan shows hyperechoic fibroglandular periareolar tissue with a prominent central retroareolar hypoechoic nodule.
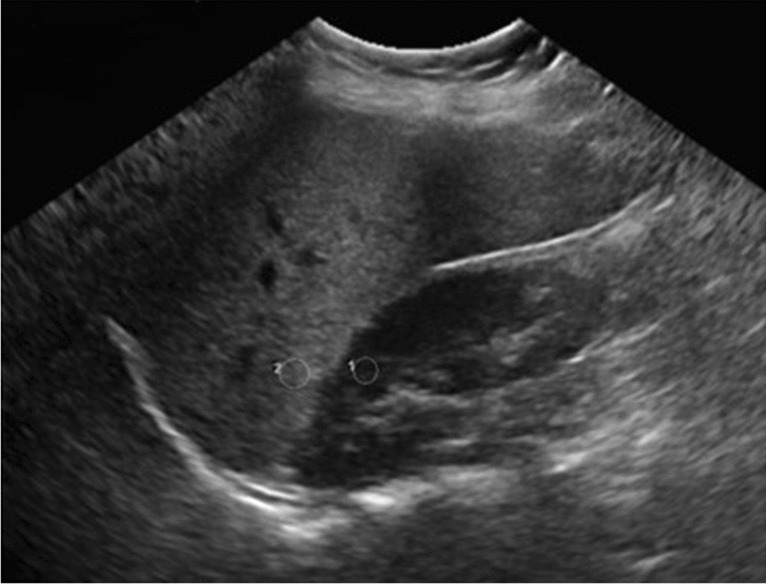
Tanner stage 5, US stage V—US scan shows hyperechoic glandular tissue, with increased subcutaneous adipose tissue anteriorly and without the hypoechoic central nodule seen in previous Tanner stages (Fig. 2).
Fig. 2
Axial plane grayscale breast ultrasound images show ultrasonographic staging of breast development (a–e) and lipomastia (f). a Stage I in a 6-year-old girl with an ill-defined hyperechoic area in the retroareolar zone (calipers). b Stage II in a 7-year-old girl with a hypoechoic core and hyperechoic nodule limited to the retroareolar area (calipers). c Stage III in an 8-year-old girl with a spider-shaped hypoechoic nodule within hyperechoic tissue exceeding subareolar area (calipers). d Stage IV in an 8.5-year-old girl with significant amount of hyperechoic tissue with secondary branching hypoechoic nodule. e Stage V in a 12-year-old girl with prominent hyperechoic tissue without central nodule. f An 8-year-old girl with prominent retroareolar adipose tissue but without any glandular breast tissue (lipomatous pattern)
Breast retroareolar glandular volume was calculated by measuring the glandular area (including the echogenic fibroglandular tissue) in three dimensions using the formula:
Fibroglandular volume = Length × Width × Height × 0.520 (Fig. 3).
Fig. 3
Grayscale ultrasound volume measurements of a stage III breast bud in a 4-year-old girl who was diagnosed with premature thelarche. a Longitudinal plane image shows the superoinferior measurement (calipers). b Axial plane image shows the mediolateral (calipers +) and anteroposterior (calipers x) measurements. Breast volume was calculated to be 1.6 cc
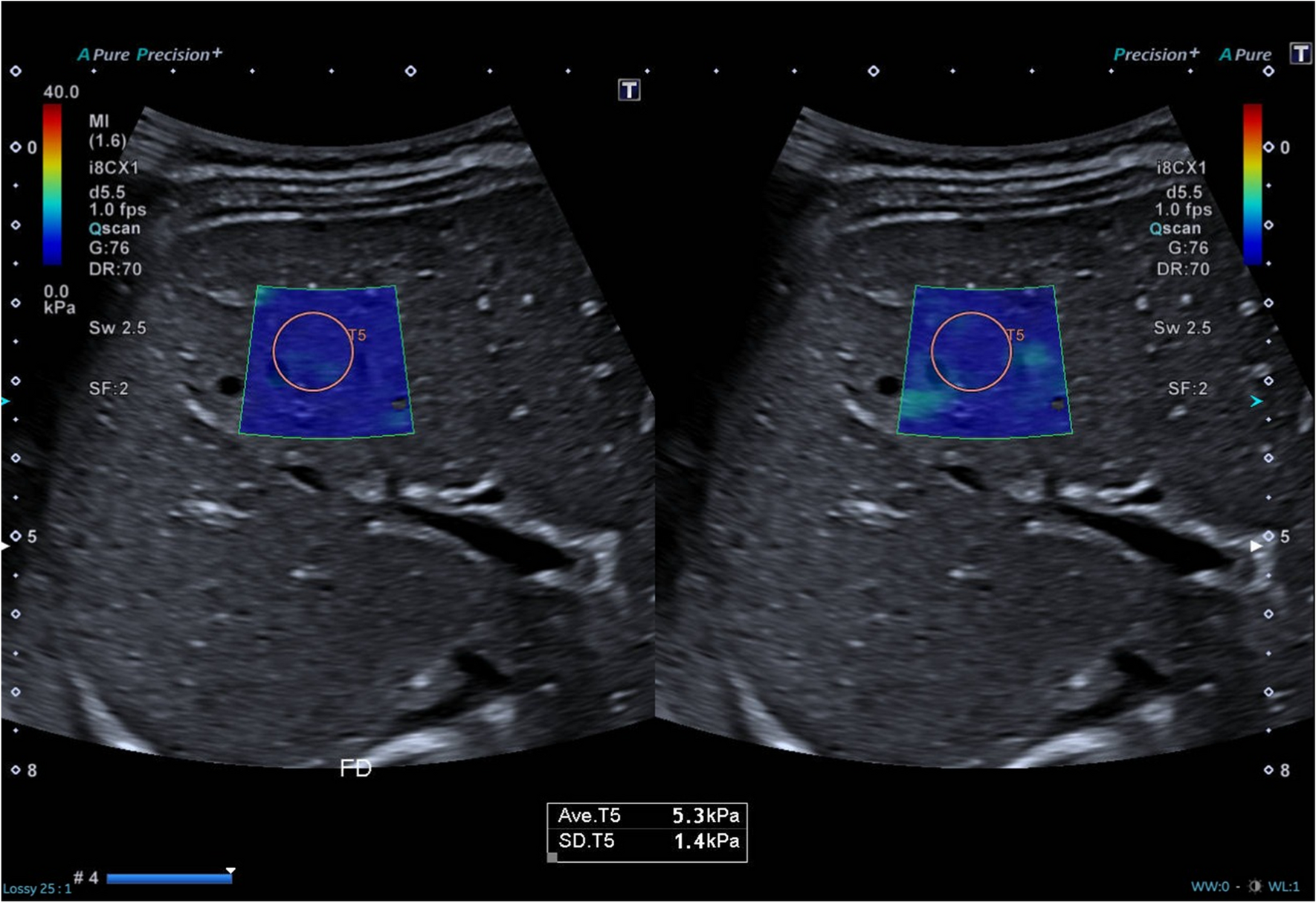
Shear-wave US elastography measurements were performed on the slice with the largest fibroglandular width, applying as little pressure as possible. A 2 × 2 mm square region of interest (ROI) was placed in three different locations on the slice, based on the color map paying attention to include those parts of the hypoechoic tissue with the highest shear velocities (Fig. 4). The average of these three values was recorded in meters per second.
Fig. 4
Shear-wave elastography assessment in an 8-year-old girl with a stage III breast bud who was diagnosed with premature thelarche. Grayscale axial ultrasound without (a) and with (b) shear-wave speed measurements at different locations (squares). Mean shear wave velocity was calculated to be 3.66 m/s (b)
For breast volume and breast elastography, the sum of the two breasts was used for presentation and analysis.
Clinical evaluation of the rate of progression of pubertal development was performed after a follow-up period of at least 6 months. All girls with rapidly progressive precocious puberty underwent cranial magnetic resonance imaging and treatment with GnRH analog.
Informed consent was obtained from each parent or guardian and the study protocol was approved by the ethical committee of our institution.
Statistical evaluation was performed using Number Cruncher Statistical System2020 Statistical Software (NCSS LLC, Kaysville, UT). Quantitative data are expressed as mean ± standard deviation (SD), or median and range as appropriate. Distribution of the data was evaluated by the Shapiro–Wilk test and Box Plot graphics. Pairwise comparisons were performed using an independent samples test (Student t test) when data was normally distributed. The non-parametric Mann–Whitney U test was used when the normality assumption of data distribution was absent. Bonferroni’s correction was used where appropriate. Statistical significance was set at P < 0.05.
Diagnostic accuracy (sensitivity, specificity, positive predictive value, negative predictive value) and receiver operating characteristic (ROC) curve assessments were used to determine the most appropriate parameters and cut-offs for potential clinical predictors of progressive precocious puberty requiring treatment. Dependent variables included being in either the treatment or no treatment group, whereas breast volume by US, elastography results, peak LH, uterine volume, uterine length, and total ovarian volume were independent variables. The optimal cut-off values were evaluated using the Youden index (J) which is defined as J = maximum (sensitivity + specificity − 1). Multivariate evaluations were performed using backward logistic regression analyses. Significance of the model was evaluated by the chi-square test. Pearson’s correlation coefficient for continuous variables was used to investigate the associations between the variables.
留言 (0)