
記住我
Primary immune thrombocytopenia (ITP) is an autoimmune disease characterized by idiopathic thrombocytopenia, with an annual prevalence of two to four instances per 100 000 people. Clinical manifestations are mainly skin and mucous membrane bleeding, and in severe cases, there may be internal organs or even intracranial hemorrhage [1]. As the main treatment for ITP, glucocorticoids achieve initial remission in two-thirds of patients, but the relapse rate is high after drug reduction or discontinuation [2]. Second-line therapy also has a variety of practical limitations. So there is a need to find new agents that can sustain platelet levels and provide a viable treatment for patients with recurrent/refractory ITP.
Sirolimus is an immunosuppressive drug that belongs to the class of mammalian targets of rapamycin (mTOR) inhibitors [3]. It can prevent the formation of platelet antibodies and weaken the immune response [3,4]. It has since been used to treat various immune-mediated disorders, including autoimmune lymphocyte hyperplasia syndrome (ALPS), autoimmune hemolytic anemia (AIHA), Evans syndrome, and ITP [5–7]. However, the available data on sirolimus's efficacy in these conditions are still limited, and its overall application may be constrained. In addition to sharing the institution's experience with sirolimus in treating ITP, the mentioned study aims to compare the regulatory T cells (Treg cells) in patients before and after sirolimus therapy with those in healthy control groups. This comparison would provide a better understanding of the pathophysiology of ITP and the impact of sirolimus treatment on Treg cells.
Materials and methods PatientsAll patients included had been diagnosed with primary ITP and had undergone at least two tests showing a low platelet count, with normal blood cell morphology. Physical examination did not reveal any enlargement of the spleen. The number of megakaryocytes found in the bone marrow was either normal or elevated, indicating a maturation problem. Other potential causes of secondary thrombocytopenia, such as connective tissue disorders, thyroid disorders, lymphatic system proliferative disorders, myelodysplastic disorders (aplastic anemia and myelodysplastic syndrome), hematologic malignancies, chronic liver disease, hyperplenism, common immunodeficiency diseases, infections, or drug-induced thrombocytopenia were ruled out.
The patients included in the study had been initially treated with glucocorticoids and/or intravenous immunoglobulin (IVIG) therapy, which are the typical first-line treatments for ITP. However, they either relapsed or did not respond to these treatments. Some patients had previously received second-line therapies other than mTOR inhibitors, whereas others had not. The age range of the patients varied from 13 to 83 years. Specifically, the study focused on patients who had not responded.
Study designThis retrospective study aimed at evaluating the effectiveness and safety of sirolimus monotherapy in the treatment of primary ITP. Prior to participating in the study, each patient provided written informed consent and agreed to be managed by the approved physicians for the trial and follow-up.
The patients were monitored at various time points, including before starting the medication, at 1, 2, and 3 weeks, and at 1, 2, and 3 months after starting treatment. Regular assessments of blood lipids, kidney function, and liver function were conducted every 2 weeks. The proportion of regulatory T (Treg) cells was measured using flow cytometry before starting medication and at 3 months after initiation of treatment. All laboratory assays were performed by the same laboratory within the same institution.
Data on the patients’ gender, age, and immunologic features were gathered concurrently. Before the study was conducted, it received approval from the Ethics Committee of the unit (YQ/012023/01) and adhered to the principles outlined in the Declaration of Helsinki.
TreatmentThe starting dose of sirolimus for adults ranged from 2 to 4 mg/day, with a maintenance dose of 1–2 mg/day. For children, the starting dose was 1–2 mg/day, with a maintenance dose of 0.5–1 mg/day. The dosage could be adjusted if needed to maintain a specific blood concentration of sirolimus, typically between 5 and 15 ng/ml, throughout the treatment period.
The blood concentration of sirolimus was monitored after 1 week of treatment, 1 month, or whenever significant side effects were observed. This was done to ensure the drug was within the therapeutic range and make any necessary dosage adjustments.
To maintain consistent bioavailability, patients were usually instructed to take sirolimus at fixed times, either with or without food. It was also important to avoid consuming grapefruit or grapefruit juice during dosing as it can interfere with the drug's metabolism.
All patients included in the study were required to continue taking sirolimus for a minimum of 3 months, provided they were tolerating the drug well. If no improvements were observed after 3 months, the drug was gradually discontinued. Patients who showed a response to sirolimus continued the treatment for more than 6 months to 1 year.
Evaluation of responseThe evaluation criteria used in this study, based on the ITP International Working Group standard, are as follows: complete response (CR) represents a platelet count (PLT) higher than 100 × 109/l without bleeding after treatment; response (R) signifies a PLT exceeding 30 × 109/l and at least two times the baseline count without bleeding; no response (NR) indicates a PLT below 30 × 109/l, an increase of less than twice the baseline count, or the presence of bleeding after treatment. Relapse is defined by a drop in platelet counts or the return of bleeding symptoms in patients with CR or R. Overall response (OR) encompasses both CR and R. The time from treatment initiation to CR or R is considered the response time, and sufficient platelet count tests must be conducted for defining CR or R. Recurrence is determined by at least two tests with a minimum of 1-day interval in between.
Toxicity monitoringThe evaluation criteria refer to Common Terminology Criteria for Adverse Events (CTCAE)5.0, published by the American Cancer Society. Patients with severe adverse reactions should be withdrawn from the study immediately and given appropriate treatment. After treatment, all patients were followed up for 1 month for safety, whether effective or not.
Examination of regulatory T cellsTreg cells were detected using flow cytometry to measure the percentage of CD4+CD25highCD127low/CD4+T cells. Peripheral blood samples were collected before and 3 months after sirolimus treatment.
Statistical analysisSPSS 25.0 statistical software was used for data analysis. Shapiro–Wilk test was used to check whether the data met the normal distribution. The mean value of measurement data conforming to the normal distribution was expressed as mean ± SD, whereas the mean value of disobedience was expressed as median, and the count data was expressed as a percentage. Univariate ANOVA analysis of variance was used to compare the differences between groups for measurement data conforming to normal distribution; Friedman nonparametric test was used for multiple relevant samples for data disconforming to normal distribution or uneven variance, and P less than 0.05 was considered statistically significant. The risk factors influencing the curative effect were analyzed by binary logistic regression.
Results Patient characteristicsA total of 20 patients diagnosed with ITP were included in this study, with 6 men and 14 women. The median age of the patients was 51 years, ranging from 13 to 83 years. Among them, 2 patients were children, aged 13 and 14 years. All patients initially received glucocorticoid therapy upon diagnosis, with an early treatment effectiveness rate of 60%. Out of the total, three cases (15%) were administered IVIG at the onset of the disease. For patients who did not respond to or relapsed after hormonal therapy, alternative treatments were used: four cases (20%) were given cyclosporine A, five cases (25%) received TPO-RAs (thrombopoietin receptor agonists), four cases (20%) were treated with eltrombopag, two cases (10%) received azathioprine, and three cases (15%) utilized traditional Chinese medicine. However, these treatments showed poor efficacy or failed to maintain stable platelet counts. The median time from diagnosis to sirolimus initiation for all enrolled patients was 18.5 months, ranging from 1.5 to 294 months. Prior to commencing sirolimus treatment, all patients had discontinued their previous second-line treatment regimen for at least 1 month. In six patients, hormone reduction was in progress during sirolimus introduction. Rapid hormone reduction was achieved within 4–6 weeks of sirolimus application, followed by maintenance treatment with sirolimus alone (Table 1).
Table 1 - Clinical characteristics of immune thrombocytopenia patients Cases (n) Percentage (%) Age ≤40 6 30 >40 14 70 Gender Male 6 30 Female 14 70 Efficacy of early hormone therapy Effective 12 60 Ineffective 8 40 First-line treatment Glucocorticoids 20 100 IVIG 3 15 Second-line treatment CSA 4 20 TPO 5 25 Eltrombopag 4 20 Azathioprine 2 10 Chinese traditional medicine 3 15After 3 months of sirolimus treatment, 6 out of 20 ITP patients (30%) achieved a CR, whereas another 6 patients (30%) achieved a response (R), resulting in an overall effective rate of 60% (12/20). These 12 patients continued to receive sirolimus and were regularly monitored during follow-up. Patients who did not experience any relief from sirolimus gradually stopped using the medication and were withdrawn from clinical observation.
The median response time for the 12 patients who responded to treatment was 2 weeks, ranging from 1 to 4 weeks. Patients who achieved a CR maintained a stable curative effect after 6 months of medication. Among the patients with an initial response (R), two patients experienced disease recurrence after 6 months of medication and eventually discontinued sirolimus because of a lack of significant improvement. However, according to the previous efficacy evaluation criteria, one out of the remaining four patients still demonstrated an R response as their platelet counts measured 100 × 109/l at 4 months, 97 × 109/l at 5 months, and 99 × 109/l at 6 months.
During the follow-up period, the median duration of sirolimus use for these patients was 17 months, ranging from 8 to 36 months. Sirolimus therapy was interrupted in one patient because of disease recurrence at 8 months of treatment, whereas the CR/R patients maintained stable platelet counts (Tables 2 and 3 and Figs. 1 and 2)
Table 2 - Efficacy evaluation of immune thrombocytopenia patients treated with sirolimus Cases of response during medication (n) Duration of medication Cases (n) NR R CR Effective rate (%) <1 week 20 18 2 0 10 2 weeks 20 13 6 1 35 3 weeks 20 10 9 1 50 1 months 20 9 7 4 55 3 months 20 8 6 6 60 6 months 12 2 4 6 50 χ 2 29.005 P value <0.001aCR indicates complete response; R, response; NR, no response.
aP < 0.05 was considered significant (analyzed by Fisher's exact test).
aData are presented as median.
∗P < 0.05 was considered significant (analyzed by nonparametric test).
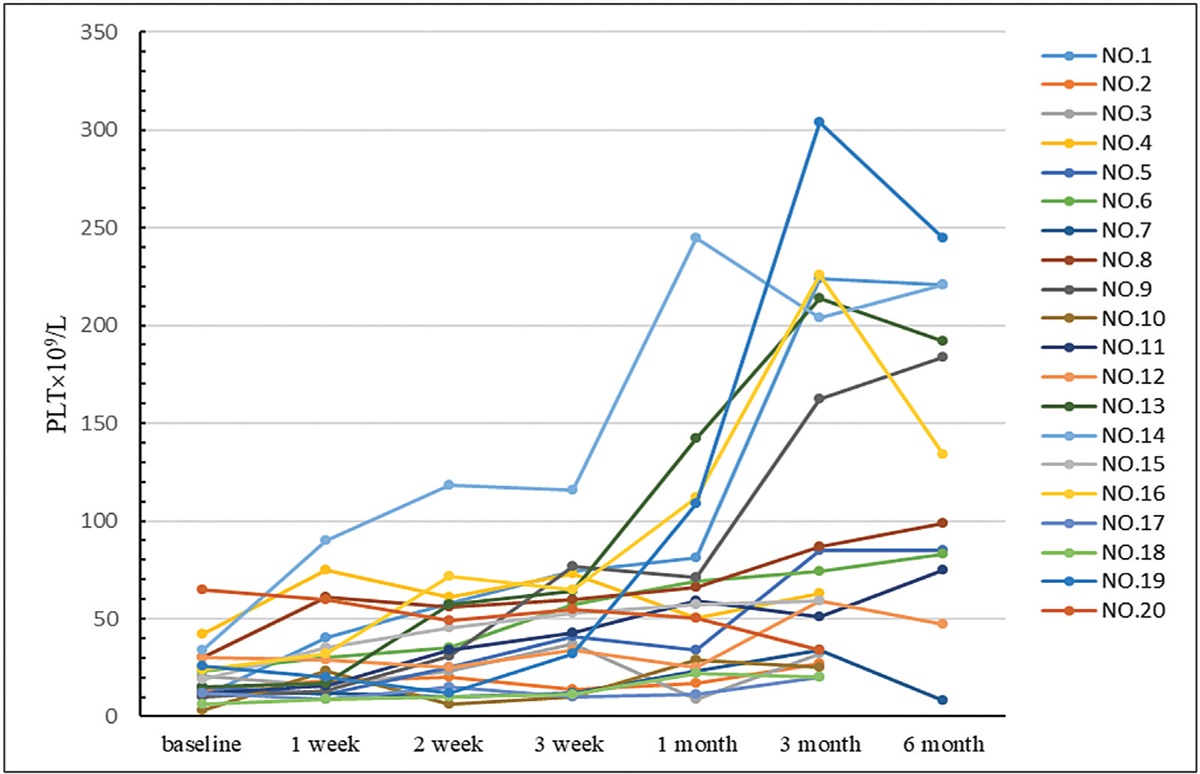
 Fig. 1:
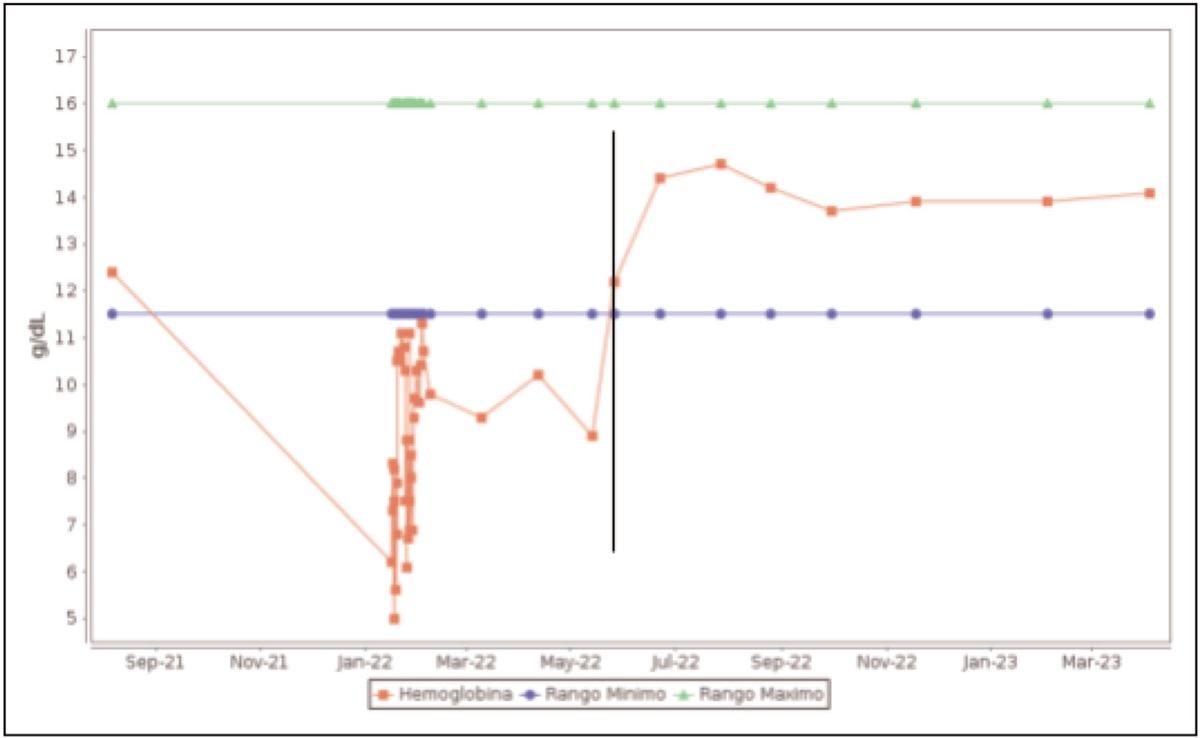
Fig. 1: Platelet values of 20 patients with immune thrombocytopenia treated with sirolimus.
 Fig. 2:
Fig. 2: Changes of platelet levels in immune thrombocytopenia patients during sirolimus treatment.
In order to assess the true efficacy of sirolimus treatment for ITP, we analyzed the impact of various factors including gender, age, duration of diagnosis, and initial platelet count on treatment effectiveness. However, our analysis revealed that none of these factors were found to be associated with the efficacy of sirolimus treatment. This suggests that sirolimus may be effective regardless of these demographic and clinical variables in treating ITP. Further studies may be needed to explore other potential factors that could influence the response to sirolimus therapy in ITP patients (Table 4).
Table 4 - Correlation analysis of factors affecting the efficacy of sirolimus OR value with 95% confidence interval Factor Regression coefficient b Significance (P value) OR value Lower limit Upper limit Gender 1.621 0.161 5.060 0.524 48.888 Age 1.357 0.303 3.883 0.293 51.412 Duration of diagnosis −0.004 0.566 0.996 0.983 1.010 Initial PLT value −0.017 0.695 0.984 0.906 1.068OR, overall response; PLT, platelet count.
To assess the impact of sirolimus treatment on Treg levels in ITP patients, we compared the proportion of Treg cells before and after 3 months of sirolimus therapy in 20 ITP patients, as well as in a control group of 20 healthy individuals.
Before therapy, the proportion of Treg cells in the ITP patients was not significantly different from that of the normal control group (P = 0.648), as determined by a single-factor ANOVA test. However, after medication, there was a significant difference in the proportion of Treg cells compared with the normal control group (P = 0.004). Nevertheless, there was no significant difference in the proportion of Treg cells before and after sirolimus treatment (P = 0.067).
These results indicate that sirolimus treatment, when combined with the rank mean, significantly enhanced the proportion of Treg cells in all three states. The increase in Treg cells induced by sirolimus may contribute to the treatment of ITP (Table 5).
Table 5 - Treg/CD4+ T-cell levels in normal subjects and immune thrombocytopenia patients before and after treatment Total variation Multiple comparisons Cases (n)x¯
± s F P value Sample-sample P value Contrast 20 5.22 ± 0.18a 7.403 0.001∗ Control – before medication 0.648 Premedication 20 5.81 ± 0.52 Control – after medication 0.004∗ After medication 20 7.91 ± 0.71 Before medication – after medication 0.067aData are presented as mean ± SD.
∗P < 0.05 was considered significant (analyzed by repeated measure ANOVA).
All patients in the study received sirolimus treatment without experiencing any grade 3 or higher adverse effects. Adverse reactions that occurred were generally mild and included acne in one instance, diarrhea in two cases, rash in two cases, and increased transaminase in one case. These adverse reactions were effectively managed through drug dose reduction or symptomatic therapy, and they resolved over time. It is worth noting that the adverse reactions typically occurred 3 months after starting the medication.
During the course of treatment, none of the patients reported any discomfort, and treatment was not discontinued because negative drug effects. Additionally, not all patients experienced oral ulcers, elevated bilirubin levels, raised blood lipids, infections, or joint pain.
The blood concentration of sirolimus was initially higher than 15 ng/ml in two patients (27.7 and 19.5 ng/ml, respectively). However, after reducing the dosage, the blood concentration returned to the normal range. The remaining patients maintained a steady drug concentration, and there were no changes in the drug dosage because of concerns about drug concentration throughout the treatment period.
DiscussionOver the past decade, the field of ITP research has witnessed rapid advancements, leading to the emergence of new therapeutic agents and clinical trial findings. Glucocorticoids are commonly used as the first-line treatment for ITP, but their long-term efficacy is limited, with high relapse rates and various side effects such as osteoporosis and high blood pressure [2]. Intravenous immunoglobulin (IVIG) is used in emergencies or when platelet count decreases significantly, but its effects are short-lived [8]. Rituximab, recombinant human thrombopoietin (rhTPO), heteromethylated nucleic acid (hetrombopag), and eltrombopag are considered second-line or third-line therapies for ITP, but their efficacy varies and they come with certain limitations such as an increased risk of infection or the need for limited duration of use [9,10].
In this context, our center conducted a single-center study since January 2020 with the aim of exploring the clinical efficacy of sirolimus in the treatment of ITP. Sirolimus, an mTOR inhibitor, has been found to restore immune homeostasis by inhibiting the differentiation of T lymphocytes into pro-inflammatory cells, such as Th17 and Th1 cells, thereby inhibiting platelet antibody production and reducing immune response. Additionally, sirolimus promotes the differentiation of functional regulatory T cells (Tregs), which play a crucial role in maintaining immune balance [3,4]. Our study results revealed that sirolimus demonstrated a beneficial effect in a subset of ITP patients, with an overall response rate (ORR) of 55% at 1 month and 60% at 3 months, consistent with previous findings [11,12]. Although the 3-month ORR observed in our study was lower compared with a study by Feng et al.[3], which reported an ORR of 85% for sirolimus treatment in ITP, it should be noted that their study included a larger sample size. Further research is warranted to confirm and elucidate the efficacy of sirolimus in the management of ITP. Notably, the majority of international sirolimus treatments for ITP are focused on pediatric patients, and our study had a limited sample size of only adults, with comparable ORRs observed at 3 months (56%) and 6 months (44%) to those reported in pediatric studies [4,6,7].
Sirolimus demonstrated favorable clinical efficacy and was well tolerated in our study, with adverse effects such as generalized rash, facial acne, diarrhea, elevated transaminases, and hyperlipidemia being transient and resolving spontaneously or with symptomatic treatment. Importantly, sirolimus is considered a safer alternative to other second-line therapies and is suitable for long-term use because of its immunosuppressive effects and potential upregulation of Tregs.
Despite these promising findings, our study had limitations. Some patients in our study were receiving glucocorticoid adjuvant therapy concurrently with sirolimus, which may have influenced the early efficacy statistics. Additionally, the limited number of ITP cases restricted our ability to perform correlation analysis and predict long-term clinical outcomes with a larger sample size. Future research should aim to address these limitations and provide further insights into the clinical use of sirolimus in ITP management.
ConclusionIn conclusion, sirolimus holds promise as an effective and well tolerated treatment option for ITP. Its immunosuppressive properties and potential modulation of Tregs make it a valuable second-line therapy, especially for patients who do not respond well to glucocorticoids or other standard treatments. Future studies with larger sample sizes and comprehensive correlation analyses are needed to validate and expand upon our findings.
AcknowledgementsThe authors would like to thank the Third People's Hospital of Datong.
We acknowledge all the workers involved in study searching, data extraction, statistical analysis and writing.
Funding: this work was supported by Key Research and development Project of Datong (Grant Number 2020064).
Conflicts of interestThere are no conflicts of interest.
References 1. Cooper N, Ghanima W. Immune thrombocytopenia. New Engl J Med 2019; 381:945–955. 2. Kochhar M, Neunert C. Immune thrombocytopenia: a review of upfront treatment strategies. Blood Rev 2021; 49:100822. 3. Feng Y, Xiao Y, Yan H, Wang P, Zhu W, Cassady K, et al. Sirolimus as rescue therapy for refractory/relapsed immune thrombocytopenia: results of a single-center, prospective, single-arm study. Front Med 2020; 7:110. 4. Mousavi-Hasanzadeh M, Bagheri B, Mehrabi S, Eghbali A, Eghbali A. Sirolimus versus cyclosporine for the treatment of pediatric chronic immune thrombocytopenia: a randomized blinded trial. Int Immunopharmacol 2020; 88:106895. 5. Li P, Huang P, Yang Y, Hao M, Peng H, Li F. Updated understanding of autoimmune lymphoproliferative syndrome (ALPS). Clin Rev Allergy Immunol 2016; 50:55–63. 6. Bride KL, Vincent T, Smith-Whitley K, Lambert MP, Bleesing JJ, Seif AE, et al. Sirolimus is effective in relapsed/refractory autoimmune cytopenias: results of a prospective multiinstitutional trial. Blood 2016; 127:17–28. 7. Jasinski S, Weinblatt ME, Glasser CL. Sirolimus as an effective agent in the treatment of immune thrombocytopenia (ITP) and Evans syndrome (ES): a single institution's experience. J Pediatr Hematol Oncol 2017; 39:420–424. 8. Khellaf M, Michel M, Schaeffer A, Bierling P, Godeau B. Assessment of a therapeutic strategy for adults with severe autoimmune thrombocytopenic purpura based on a bleeding score rather than platelet count. Haematologica 2005; 90:829–832. 9. Bolton-Maggs PHB, George JN. Immune thrombocytopenia treatment. New Engl J Med 2021; 385:948–950. 10. Freites-Martinez A, Santana N, Arias-Santiago S, Viera A. Using the Common Terminology Criteria for Adverse Events (CTCAE - Version 5.0) to evaluate the severity of adverse events of anticancer therapies. Actas Dermosifiliogr 2021; 112:90–92. 11. Li H, Ji J, Du Y, Huang Y, Gu H, Chen M, et al. Sirolimus is effective for primary relapsed/refractory autoimmune cytopenia: a multicenter study. Exp Hematol 2020; 89:87–95. 12. Miano M, Rotulo GA, Palmisani E, Giaimo M, Fioredda F, Pierri F, et al. Sirolimus as a rescue therapy in children with immune thrombocytopenia refractory to mycophenolate mofetil. Am J Hematol 2018; 93:E175–e177.
留言 (0)