
記住我
Factor V acts as a cofactor for the anticoagulant factor protein C and is central to reducing thrombin formation by controlling anticoagulant action [1]. Moreover, it is a pivotal protein in hemostasis; its deficiency can lead to thrombosis development [2]. Since 2004, age- and sex-standardized annual incidence rates of venous thromboembolism in the Korean population have been increasing. Venous thromboembolism is a condition characterized by abnormal blood clot formation in the pulmonary arteries and the deep venous vasculature. It is often serious and sometimes even fatal if not promptly and appropriately treated [3]. In addition, factor V acts as a promoter for amplifying coagulation reactions [4]. Considering its dual role in blood clotting, factor V deficiency leads to bleeding or thrombotic tendencies [5]. Furthermore, a high level of this factor is a major risk factor for thrombosis [6].
Protein C, a vitamin K-dependent protein, exhibits anticoagulant effects by regulating the activation of Factors VIIIa and Va [7]. Venous thrombosis and pulmonary embolism can occur in protein C deficiency. The risk of venous and arterial thrombosis increases sevenfold in patients with heterozygous deficiency [8].
Both factor V and protein C are essential in blood coagulation. Therefore, clinicians should evaluate the risks and prevent thrombosis through early diagnosis. For this reason, thrombosis screening tests are conducted. Blood coagulation tests are performed for screening before surgery, identifying the cause of hemorrhagic diseases and thrombosis, or monitoring anticoagulant treatment. In thrombosis, clots form within the blood vessels and interfere with the blood flow, causing serious complications, such as heart attack, stroke, and pulmonary embolism. Thrombosis involves the formation of blood clots that can obstruct blood vessels, potentially leading to life-threatening complications such as cardiac arrest and stroke, thereby posing a serious risk to patients’ lives and health. In Korea, the incidence of thrombosis is increasing every year because of an increase in the number of older adults and changes in lifestyle [9,10]. In modern society, thrombosis has emerged as a major health problem, warranting early prevention and diagnosis. However, people have limited access to the diagnosis and management of thrombosis because of its insufficient evaluation in Korea. Thrombosis is associated with abnormalities in blood clotting function caused by factor V and protein C abnormalities [11,12].
Predicting the risk of bleeding and thrombosis using common coagulation tests is not effective. Routine coagulation tests, such as prothrombin time (PT) and activated partial thromboplastin time (aPTT), are primarily designed to monitor anticoagulants such as warfarin and heparin, respectively [13]. Blood coagulation function can be determined only by measuring the blood coagulation factors [14]. Moreover, no studies have reported on the influence of sex and age on the relationship between factor V and protein C abnormalities and the onset of thrombotic diseases in Koreans. Notably, previous research indicates that the incidence of thrombosis varies by age and sex [15]. Therefore, we aimed to retrospectively analyze the correlation of thrombotic disease with the distribution of sex and age in 1386 individuals for whom factor V and protein C tests were simultaneously requested to be conducted by entrusted Korean inspection institutions. These institutions conduct large-scale tests according to age group and sex. Furthermore, we intended to determine whether these factors could be used as an auxiliary test for diagnosing thrombosis.
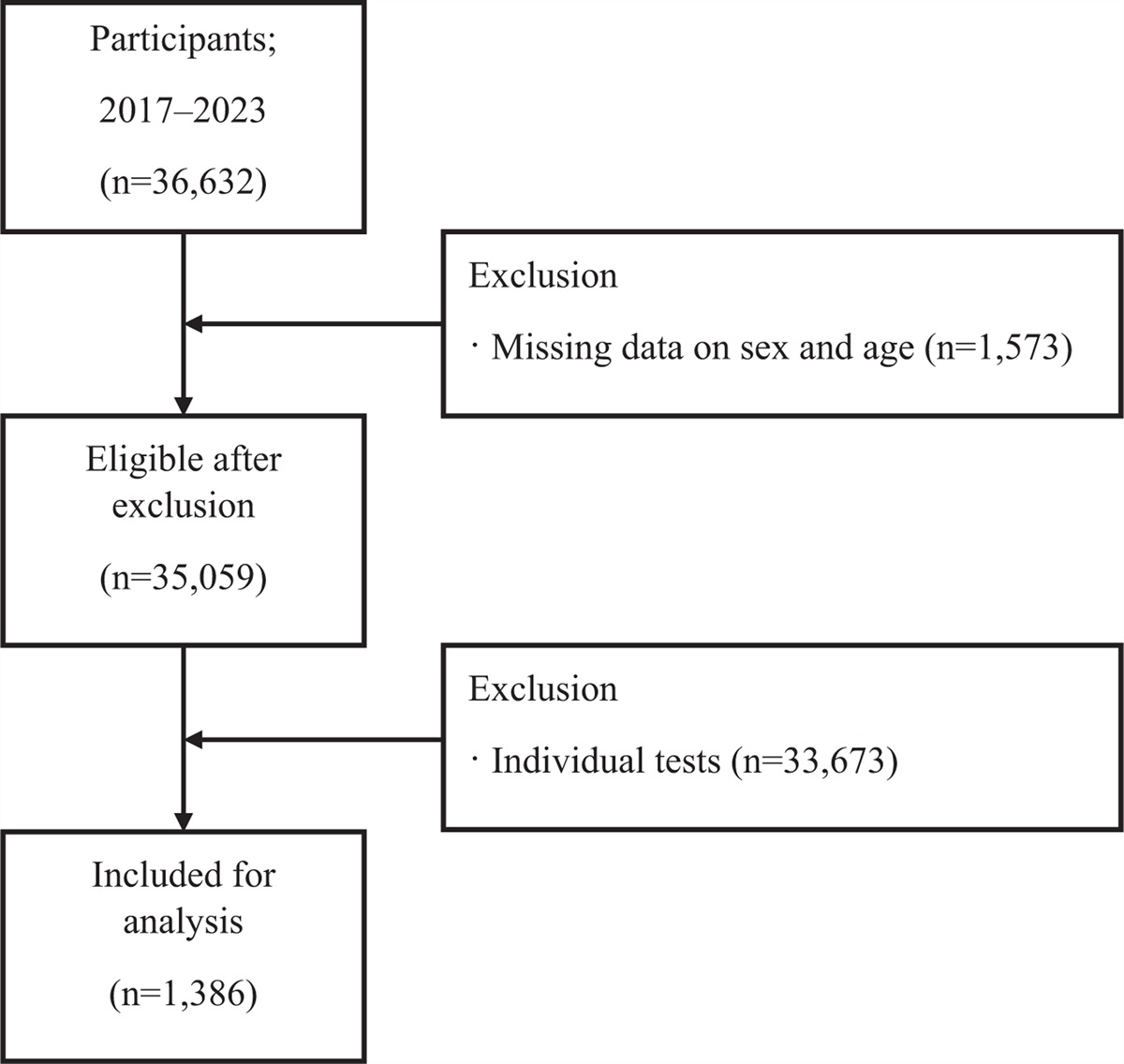
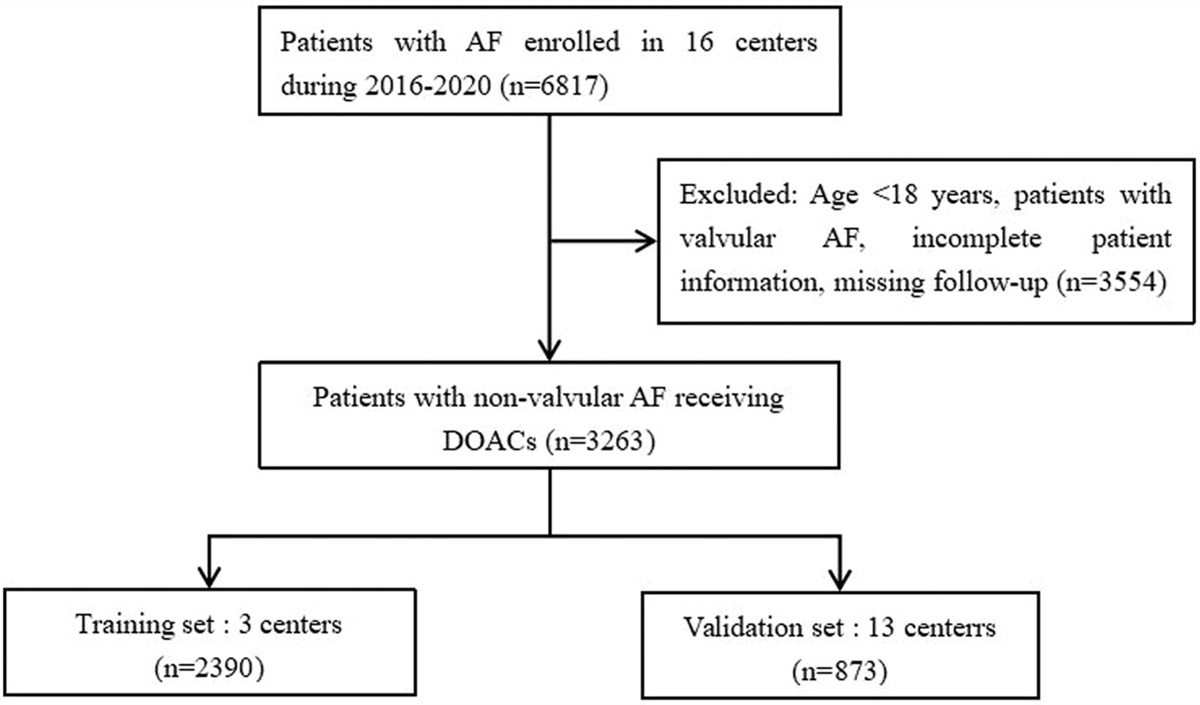
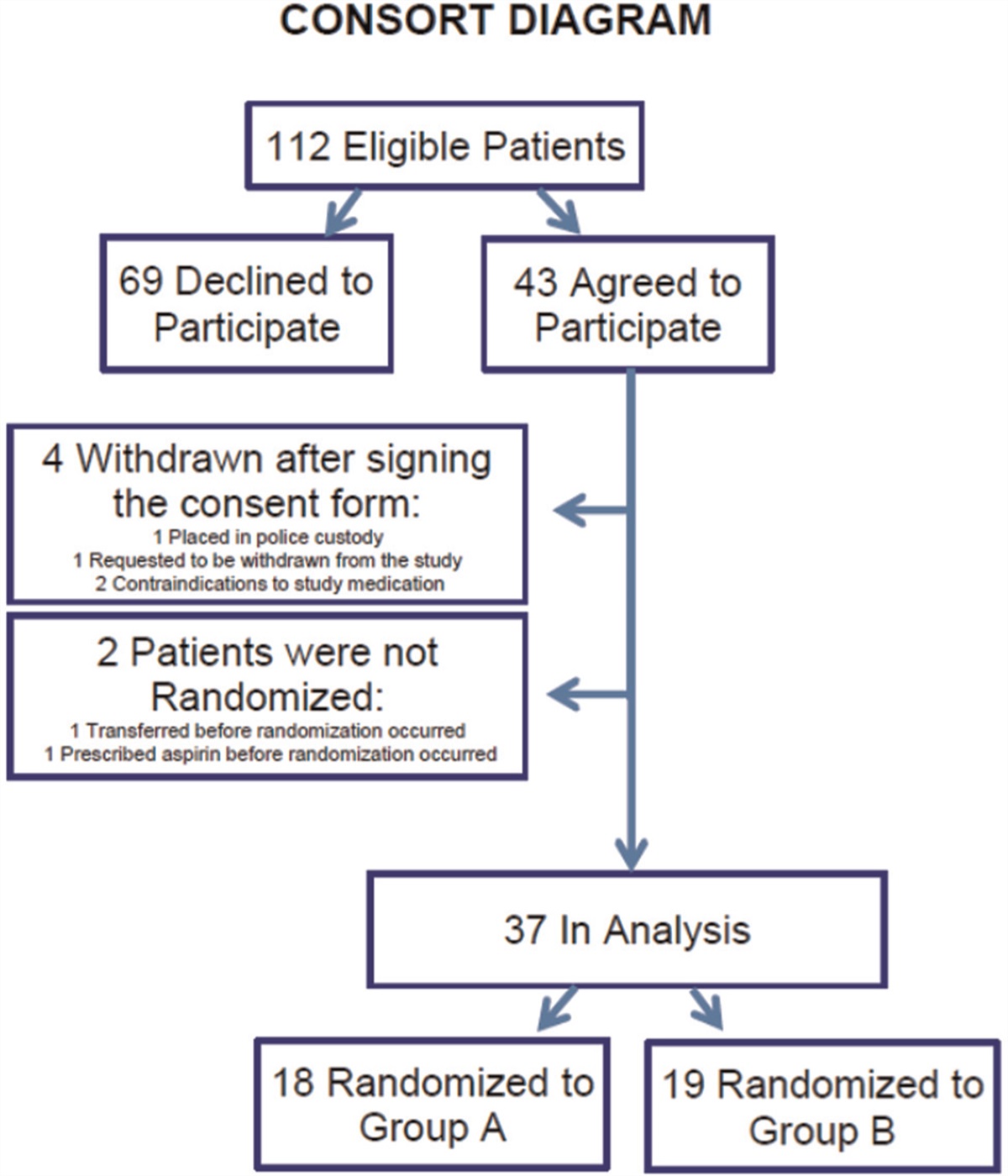
Methods Target population and data collectionSamples for testing originating from hospitals across the country were sent to EONE Laboratories (Incheon-si in Korea), which were equipped for testing. From January 2017 to July 2023, the EONE Laboratories performed 3111 factor V tests and 33 521 protein C tests, resulting in a total of 36 632 test results. We excluded 930 and 643 individuals who underwent the factor V and protein C tests, respectively, because of missing information on sex and age. We also excluded individuals who underwent only the factor V or protein C test (n = 33 673). We retrospectively compared and analyzed 1386 individuals (416 men and 970 women) who underwent both tests simultaneously. The study sample comprised 416 men and 970 women. We did not consider overlapping individuals in the dataset. We received data from EONE Laboratories and analyzed them retrospectively. In addition, the correlation between the results of simultaneous factor V and protein C tests was evaluated by analyzing the annual test trend, sex, and age (Fig. 1).
 Fig. 1:
Fig. 1: Study sample enrollment process. n, number of individuals assessed.
MaterialsA tube comprising 0.3 ml of 3.2% sodium citrate (BD Vacutainer, Becton Dickinson, Franklin Lakes, NJ, USA) was used as an anticoagulant. Venous blood was collected using a ratio of 1 volume of 0.109 mol/l citrate to 9 volumes of blood. It was then centrifuged at a rate of 2500g for 15 min. Subsequently, the plasma was separated for examination.
AnalysesSTA-Deficient V (Diagnostica Stago, Asnieres, France) was used as the reagent, and STA R MAX (Diagnostica Stago, Asnieres, France) was used as the equipment for the factor V test. The test was performed using the coagulation method. We measured the activity of factor V in plasma using the factor V-deficient plasma of the reagent.
STA – Stachrome protein C (Diagnostica Stago, Asnieres, France) was used as the reagent, and STAR MAX (Diagnostica Stago, Asnieres, France) was used as the equipment for the protein C test. Both tests were commercialized. STA – Unical Corrector (Diagnostica Stago, Asnieres, France) activated using the correction curve was expressed as the functional protein C level, using the calibration curve % material.
Quality control was performed using the commercially available STA – System Control N+P (Diagnostica Stago, Asnieres, France) substance for each test. All tests were performed according to the manufacturer's instructions, and the results were analyzed retrospectively.
Statistical analysisAnalysis was performed using the average values of factor V and protein C test results. The collected data were computerized and statistically analyzed using Microsoft Excel 2010 (Microsoft, USA) program. All statistical analyses were performed using jamovi (version 2.4.11, jamovi, Sydney, Australia). An independent t-test was used to determine the correlation among the multiple assays. Statistical significance was set at P < 0.05.
Results Annual testing frequencyThe number of tests performed for both factor V and protein C increased gradually from 2017 (n = 110) to 2022 (n = 249). The tests conducted in 2023 (n = 143) only included those from January to July for the analysis (Table 1).
Table 1 - Annual testing frequency Year 2017 2018 2019 2020 2021 2022 2023 Total N 110 176 219 243 246 249 143 1386N, number of individuals assessed.
In the studied cohort of 1386 participants, the tests were predominantly performed in women, that is, in 416 (30.0%) men and 970 (70.0%) women. The mean age of the men was 59.3 years, ranging from a minimum of 8 to a maximum of 96 years. Conversely, the mean age of the women was 45.1 years, with ages spanning from 12 to 99 years. The test frequency was 95 (22.8%), 100 (24.0%), and 70 (16.8%) in men aged from 50 to 59 years, 60 to 69 years, and 70 to 79 years, respectively. The highest test frequency was 472 (48.7%) in women aged 30–39 years, followed by 207 (21.3%) in those aged 40–49 years. Unlike those in men, the testing rates increased noticeably in women aged 30–39 years and 40–49 years (Table 2).
Table 2 - Number of tests conducted in men and women stratified by age Men Women Age (years) n % n % <20 3 0.7 3 0.3 20–29 21 5.0 54 5.6 30–39 34 8.2 472 48.7 40–49 44 10.6 207 21.3 50–59 95 22.8 39 4.0 60–69 100 24.0 50 5.2 70–79 70 16.8 61 6.3 ≥80 49 11.8 84 8.7 Total 416 100.0 970 100.0n, number of individuals assessed.
In men, the number of tests increased for those over 20 years old and decreased for those aged 50–59 years. The lowest factor V concentrations were recorded in men aged <20 years (71.3%); the highest concentrations were recorded in men aged 50–59 years (85.1%). In women, the number of tests decreased with age >20 years and increased after 30–39 years. Factor V concentrations were 59.0%, 52.5%, and 60.6% in women aged 20–29 years, 30–39 years, and 40–49 years, respectively. A t-test was conducted to evaluate the significance of factor V test results based on age and gender, as the results indicated lower levels in women compared to men in the childbearing age group (Fig. 2). Specifically, the t-test results for factor V, segregated by gender, revealed statistically significant differences between women and men within the fertile age ranges of 20–29 years (P = 0.036), 30–39 years (P<0.001), and 40–49 years (P < 0.001) (Table 3).
 Fig. 2:
Fig. 2: Mean plasma factor V concentrations according to 10-year age groups.
Table 3 - t-Test for average values of factor V according to age and sex Factor V Statistics df P <20 Student's t −2.517 4.00 0.967 20–29 Student's t 1.83 a 73.0 0.036 30–39 Student's t 5.31 504 <0.001 40–49 Student's t 3.56 249 <0.001 50–59 Student's t 0.116 132 0.454 60–69 Student's t 0.00528 a 148 0.498 70–79 Student's t −0.256 129 0.601 ≤80 Student's t −1.14 131 0.872The mean values between men and women aged 20–49 years denoted a significant difference (P < 0.05).
The average value of protein C decreased with an increase in age from 50–59 years and 60–69 years in men and women, respectively. Individuals aged 20–29 years (94.5% in men and 113.4% in women), 30–39 years (107.4% in men and 117.0% in women), and 40–49 years (104.5% in men and 119.0% in women) demonstrated higher protein C concentrations than did those of childbearing age (Fig. 3). A t-test was conducted to assess the significance of the protein C test results based on age and gender, given that these results were higher in women than in men, particularly in the childbearing age group. For protein C outcomes, the t-test analysis revealed statistically significant differences by gender in the fertile age group at 20–29 years (P = 0.006), 30–39 years (P < 0.023), and 40–49 years (P = 0.001) (Table 4).
 Fig. 3:
Fig. 3: Mean plasma protein C concentration according to 10-year age groups.
Table 4 - t-Test for average values of protein C according to age and sex Protein C Statistics df P <20 Student's t 0.188 4.00 0.570 20–29 Student's t −2.57 73.0 0.006 30–39 Student's t −2.00 504 0.023 40–49 Student's t −3.06 249 0.001 50–59 Student's t 0.907 132 0.817 60–69 Student's t −1.74051 148 0.042 70–79 Student's t −1.463 129 0.073 ≤80 Student's t −3.27 131 <.001The mean values between men and women aged 20–49 years denoted a significant difference (P < 0.05).
Results of the factor V and protein C tests were analyzed at a consignment agency in Korea. The factor V and protein C test numbers increased every year. Women underwent more tests than men did. The number of tests tended to decrease after 60 years of age. Particularly, women of childbearing age (20–49 years) reported low average factor V and high average protein C concentrations. The incidence of venous thromboembolism across the United States increased by 33.1% from 2002 to 2006 (from 317 to 422) [16]. Furthermore, the annual prevalence of venous thromboembolism across East Asia increased gradually [17]. The incidence of thrombotic diseases in Koreans has been increasing steadily every year [18,19], which will likely cause an increase in factor V and protein C testing among Koreans.
The incidence of thrombosis is higher in women than in men, and it increases with age [9,15]. In this study, 416 (30.0%) men and 970 (70.0%) women underwent factor V and protein C tests. Because the incidence of thrombosis was higher in women than in men, the number of women who underwent the tests was higher than that of men.
In the case of factor V deficiency, clotting inhibition may be affected beyond the factor V molecules, causing blood clots. The individuals may undergo factor V Leiden mutation tests [5,20]. However, the condition has been excluded as a rare coagulopathy in Asians. In this study, factor V test frequency in men increased with age >20 years and decreased after 50–59 years. In addition, younger women reported a lower average factor V concentration; however, it increased gradually in women aged 30–39 years. Factor V concentrations increase with age in healthy people [21]. Moreover, the concentrations increase [22] or do not change significantly in pregnant women [23]. Thus, our results differ from the average results reported for women of childbearing age [24]. The use of oral contraceptives increased the coagulation factors and decreased factor V concentration [25]. In this study, factor V concentrations demonstrated a particularly low average value in young women. The estrogen component of oral contraceptives is closely related to thrombosis development [26]. Furthermore, women report a higher incidence of thrombosis than men do because of oral contraceptive consumption and hormonal changes caused by pregnancy [24,27].
Protein C controls and prevents blood clot formation by inactivating factors V and VIII, activated by vitamin K-dependent proteins [28]. Patients with thrombotic disease demonstrate reduced concentrations of protein C [29]. The risk of venous blood clots is 8–10 times higher in individuals with protein C deficiency than in those with normal protein C levels [12]. During pregnancy, hormonal changes alter the production of coagulation proteins; the risk of thrombosis increases by 4–5 times during and by 20–80 times after pregnancy [30]. Protein C concentrations increase to maintain normal pregnancy and to inhibit thrombogenesis [31]. A study in Iran evaluated the effects of sex and age and reported that the use of oral contraceptives was associated with an increase in protein C concentrations [32]. In a study in Italy evaluating outcomes by sex and age, protein C concentrations were high in women who used oral contraceptives [33]. Furthermore, women aged 35–44 years report high protein C concentrations [34]. In this study, women aged 20–49 years reported higher protein C concentrations than did men. These results are attributed to pregnancy and oral contraceptive use. In a study in Thailand, postmenopausal women reported higher protein C values than men [35]. In this study, the average protein C concentration was higher in women than in men; both men and women demonstrated a decreasing concentration trend with age. Protein C concentrations decrease with age, which may be attributed to changes in the blood coagulation system. Factors such as changes in the blood vessel wall with aging and decreased blood circulation can affect the level of blood coagulation protein.
In this retrospective study, we assessed the results of both factor V and protein C laboratory tests to gain insights into the occurrence, prevention, and treatment of thrombotic diseases. We excluded the influence of physiological factors that may affect thrombosis. Our study included only the results of factor V and protein C tests; therefore, these tests alone cannot confirm thrombosis. One limitation was that we did not evaluate patient information, such as the presence of the disease being assessed, treatment status, and medication information. Thus, prospective studies that include pregnancy status and contraceptive use are required to resolve these issues.
In conclusion, no previous study has reported on thrombosis in Korean men and women according to their life cycle. In this study, we analyzed the distribution by sex and age and the results of only factor V and protein C tests. The results of this study have significant implications in the field of women's health and reproductive medicine, particularly in understanding their impact on the risk of thrombotic disorders in women. Research that focuses on the prevention of thrombotic disorders related to pregnancy is of utmost importance. The findings can contribute to a deeper understanding of the functionality and regulation of the blood coagulation system. This knowledge can help us better comprehend the mechanisms underlying various coagulation disorders and may provide insights for the development of novel treatment approaches.
AcknowledgementsThe data used in this study were obtained from EONE Laboratories (https://www.eonelab.co.kr/). Owing to the company policy, the data cannot be disclosed. Data can be accessed from the corresponding author upon reasonable request.
Patient consent: The need for patient consent was waived in this study.
Ethics approval: This study was approved by the Clinical Trials Ethics Committee of Dankook University (institutional review board number: 2023-11-017-001). It adhered to the tenets of the Declaration of Helsinki. This study analyzed the existing test results retrospectively without including any personal patient information. Thus, obtaining consent was deemed unnecessary.
Author contributions: Min Ji Na: Made substantial contributions to the conception or design of the study and the acquisition and analysis of data.
Jae Kyung Kim: Made substantial contributions to the acquisition and analysis of data.
Funding: The study did not receive specific grants from funding agencies in the public, commercial, or nonprofit sectors.
Availability of data and materials: Information evaluated during the study can be accessed from the corresponding author upon request.
Conflicts of interestConflicts of interest and source of funding: The authors have no financial conflicts of interest to declare. All authors approved the final article.
References 1. Kamphuisen PW, Rosendaal FR, Eikenboom JC, Bos R, Bertina RM. Factor V antigen levels and venous thrombosis: risk profile, interaction with factor V leiden, and relation with factor VIII antigen levels. Arterioscler Thromb Vasc Biol 2000; 20:1382–1386. 2. Suehisa E, Kawasaki T, Toku M, Hidaka Y. Low level of factor V is associated with development of deep-vein thrombosis in Japanese patients. Thromb Res 2010; 125:128–133. 3. Hong J, Ahn SY, Lee YJ, Lee JH, Han JW, Kim KH, et al. Updated recommendations for the treatment of venous thromboembolism. Blood Res 2021; 56:6–16. 4. Ruben EA, Rau MJ, Fitzpatrick JA, Di Cera E. Cryo-EM structures of human coagulation factors V and Va. Blood 2021; 137:3137–3144. 5. Asselta R, Peyvandi F. Factor V deficiency. Semin Thromb Hemost 2009; 35:382–389. 6. Peyvandi F, Palla R, Menegatti M, Siboni SM, Halimeh S, Faeser B, et al. Coagulation factor activity and clinical bleeding severity in rare bleeding disorders: results from the European Network of Rare Bleeding Disorders. J Thromb Haemost 2012; 10:615–621. 7. Dahlbäck B, Villoutreix BO. The anticoagulant protein C pathway. FEBS Lett 2005; 579:3310–3316. 8. Roshan TM, Stein N, Jiang XY. Comparison of clot-based and chromogenic assay for the determination of protein c activity. Blood Coagul Fibrinolysis 2019; 30:156–160. 9. Bang SM, Jang MJ, Oh D, Kim YK, Kim IH, Yoon SS, et al. Korean guidelines for the prevention of venous thromboembolism. J Korean Med Sci 2010; 25:1553–1559. 10. Kim HY, Chang SA, Kim KH, Kim JY, Seo WK, Kim H, et al. Epidemiology of venous thromboembolism and treatment pattern of oral anticoagulation in Korea, 2009–2016: a nationwide study based on the national health insurance service database. J Cardiovasc Imaging 2021; 29:265–278. 11. Segers K, Dahlbäck B, Nicolaes GA. Coagulation factor V and thrombophilia: background and mechanisms. Thromb Haemost 2007; 98:530–542. 12. Lee JW, Jung HI, Kim HJ, Choi WI, Lee JW, Jung HI, et al. Alteration of factors associated with coagulation in provoked pulmonary embolism. Clin Exp Thromb Hemost 2014; 1:5–9. 13. Lim HY, O’Malley C, Donnan G, Nandurkar H, Ho P. A review of global coagulation assays—is there a role in thrombosis risk prediction? Thromb Res 2019; 179:45–55. 14. Go GH, Lee SK, Son JS. The thromboelastographic evaluation of coagulation profiles in term pregnant women after cesarean section delivery. Korean J Anesthesiol 2003; 45:352–358. 15. Naess IA, Christiansen SC, Romundstad P, Cannegieter SC, Rosendaal FR, Hammerstrøm J. Incidence and mortality of venous thrombosis: a population-based study. J Thromb Haemost 2007; 5:692–699. 16. Deitelzweig SB, Johnson BH, Lin J, Schulman KL. Prevalence of clinical venous thromboembolism in the USA: current trends and future projections. Am J Hematol 2011; 86:217–220. 17. Lee LH, Gallus A, Jindal R, Wang C, Wu CC. Incidence of venous thromboembolism in Asian populations: a systematic review. Thromb Haemost 2017; 117:2243–2260. 18. Hong J, Lee JH, Yhim HY, Choi WI, Bang SM, Lee H, et al. Incidence of venous thromboembolism in Korea from 2009 to 2013. PLoS One 2018; 13:e0191897. 19. Heit JA, Spencer FA, White RH. The epidemiology of venous thromboembolism. J Thromb Thrombolysis 2016; 41:3–14. 20. Huang JN, Koerper MA. Factor V deficiency: a concise review. Haemophilia 2008; 14:1164–1169. 21. Palta S, Saroa R, Palta A. Overview of the coagulation system. Indian J Anaesth 2014; 58:515–523. 22. Brenner B. Haemostatic changes in pregnancy. Thromb Res 2004; 114:409–414. 23. Katz D, Beilin Y. Disorders of coagulation in pregnancy. Br J Anaesth 2015; 115: (Suppl 2): ii75–ii88. 24. Nimjee SM, Akhter AS, Zakeri A, Herson PS. Sex differences in thrombosis as it affects acute ischemic stroke. Neurobiol Dis 2022; 165:105647. 25. Middeldorp S, Meijers JC, van den Ende AE, van Enk A, Bouma BN, Tans G, et al. Effects on coagulation of levonorgestrel- and desogestrel-containing low dose oral contraceptives: a cross-over study. Thromb Haemost 2000; 84:4–8. 26. Im JA, Kim SH, Lee DC. Effects of long term hormone therapy on platelet activation in postmenopausal women. Korean J Fam Med 2004; 25:754–759. 27. Christiansen SC, Lijfering WM, Helmerhorst FM, Rosendaal FR, Cannegieter SC. Sex difference in risk of recurrent venous thrombosis and the risk profile for a second event. J Thromb Haemost 2010; 8:2159–2168. 28. Dielis AW, Castoldi E, Spronk HM, Van Oerle R, Hamulyak K, Ten Cate H, et al. Coagulation factors and the protein C system as determinants of thrombin generation in a normal population. J Thromb Haemost 2008; 6:125–131. 29. Khan S, Dickerman JD. Hereditary thrombophilia. Thromb J 2006; 4:1–17. 30. Konkle BA. Diagnosis and management of thrombosis in pregnancy. Birth Defects Res C Embryo Today 2015; 105:185–189. 31. Fu M, Liu J, Xing J, Dai Y, Ding Y, Dong K, et al. Reference intervals for coagulation parameters in nonpregnant and pregnant women. Sci Rep 2022; 12:1519. 32. Tabibian S, Khoshmirsafa M, Paridar M, Motevalian A, Shekarabi M, Safa M. Reference interval of antithrombin, protein C, and protein S activities in healthy adults in Iran, the effect of age, sex, oral contraceptive intake, and menopause. Int J Lab Hematol 2022; 44:626–634. 33. Franchi F, Biguzzi E, Martinelli I, Bucciarelli P, Palmucci C, D’Agostino S, et al. Normal reference ranges of antithrombin, protein C and protein S: effect of sex, age and hormonal status. Thromb Res 2013; 132:e152–e157. 34. Dolan G, Neal K, Cooper P, Brown P, Preston FE. Protein C, antithrombin III and plasminogen: effect of age, sex and blood group. Br J Haematol 1994; 86:798–803. 35. Rojnuckarin P, Settapiboon R, Akkawat B, Teocharoen S, Suksusut A, Uaprasert N. Natural anticoagulant deficiencies in Thais: a population-based study. Thromb Res 2019; 178:7–11.
留言 (0)