
記住我
Venous thromboembolism (VTE) is a complication with a high incidence after major orthopaedic surgeries such as total hip arthroplasty (THA) and total knee arthroplasty (TKA), and is also an important cause of perioperative death and in-hospital unintended death [1]. In the absence of thrombosis prevention, the incidence of deep vein thrombosis after THA and TKA can be as high as 42–57 and 40–80%, respectively, and the risk of fatal PE is 0.1–2 and 0.2–0.7%, so the occurrence of VTE after orthopaedic surgery should be taken seriously [2–4].
The American College of Chest Physicians (ACCP) and the American Academy of Orthopaedic Surgeons (AAOS) guidelines also state that if not contraindicated, pharmacologic or physical methods should be used to prevent VTE after orthopaedic arthroplasty [5,6]. Low-molecular-weight heparin (LMWH), which acts by enhancing the affinity of antithrombin-III to thrombin, owns the advantage of high bioavailability and no monitoring, and was considered the drug of choice for the prevention of VTE after orthopaedic surgery. Aspirin (also known as acetylsalicylic acid), which exerts its antithrombotic effect mainly by inhibiting platelet aggregation, several studies in recent years have confirmed that aspirin is also well tolerated and effective in reducing the incidence of VTE after orthopaedic surgery [7,8]. The AAOS suggested in the 2012 Evidence-Based Guidelines for Antithrombotic and Thrombolytic Medicine, 9th edition and beyond, that aspirin can also be used for postoperative antithrombotic therapy after major orthopaedic surgery (class 1B) [6]. As the most commonly used thromboprophylactic agents, there are many clinical studies comparing the efficacy and safety of LMWH and aspirin, but their conclusions lack consistency.
Several meta-analyses have summarized and reviewed the published related articles, but the opposite results have been obtained [9,10]. These articles still have defects such as small sample sizes or inclusion of retrospective studies, so the reliability of the results is questionable. In the last 2 years, new large randomized controlled trials have been performed with the use of aspirin and LMWH [11,12]. Whether aspirin or LMWH is the best treatment option for thromboprophylaxis after orthopaedic surgery remains unclear. Therefore, this meta-analysis was conducted to determine current rates of deep venous thrombosis(DVT)/Pulmonary embolism(PE) events, major bleeding events, wound complications, wound infection and death from randomized trials of aspirin and LMWH use in patients after orthopaedic surgery.
Materials and methods Literature searchIn accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines [13], a systematic literature search was performed using PubMed, Embase, and Cochrane Library to identify eligible studies. The authors used following keywords with the Boolean operators ‘AND’ or ‘OR’ for the online search: ‘aspirin’, ‘Low-Molecular-Weight Heparin’, ‘venous thromboembolism’, ‘orthopaedic surgery’. The complete search strategy of the literature was shown in Supplementary Table 1, https://links.lww.com/BCF/A173. Medical subject heading (MeSH) and full-text word was combined to develop the search strategy. Moreover, reference lists of included articles and reviews were manually searched for additional eligible articles. The final search was performed on 25 April 2023.
Selection criteriaThe following selection criteria were employed to perform the analysis according to Population-Intervention-Comparison-Outcome-Study design (PICOS) principles. Population (P): adult patients who underwent an extremity or pelvis/acetabulum fracture or osteoarthritis that was treated operatively. Intervention (I): receive aspirin for thromboprophylaxis after surgery. Comparison (C): receive LMWH for thromboprophylaxis after surgery. Outcome (O): at least one accurate outcome of DVT events, PE events, major bleeding events, wound complications, wound infection and death was reported. Study design (S): RCTs published in English. Studies enrolling patients less than 18 years old, or lacking sufficient data for extraction were excluded from this meta-analysis.
Quality assessmentThe Cochrane risk bias assessment tool was used to evaluate the quality of the included RCTs. We evaluated each RCT through the following seven aspects: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other biases. The quality of the assessment was divided into ‘low risk’, ‘unclear’ and ‘high risk’.
Data extractionTwo reviewers independently screened the titles and abstracts of relevant studies, and excluded those that did not meet the criteria. The full texts of the selected studies were retrieved to make the terminal decisions. Disagreements between reviewers on issues of research evaluation were resolved through discussion. The extracted data included: the first author, publication year, region, number of patients, time of follow-up, age, basic characteristics of studies, medication regimen of VTE prophylaxis, and major end points. Major end points were encompassed DVT events, PE events, major bleeding events, wound complications, wound infection and death. Major bleeding events included fatal bleeding, symptomatic bleeding into a critical area or organ, or bleeding that caused a 20 g/l decrease or more in haemoglobin level or led to transfusion of two or more units of whole blood or red blood cells, bleeding that led to reoperation. Wound complications included wound drainage, hematoma or seroma of an orthopaedic injury that led to subsequent surgery.
Statistical analysisRevMan5.3 software was used for statistical analysis. Continuous variables were expressed by mean difference or standardized mean difference (SMD) with a 95% CI whereas dichotomous variables were expressed by odds ratio (OR) with a 95% CI for statistical analysis. The overall effects were determined by the z-test and P less than 0.05 was considered statistically significant. The chi-squared test and I2 statistic were used to assess the heterogeneity among the results in this meta-analysis. P less than 0.1 or I2 greater than 50% indicated that the heterogeneity was significant, and the random effects model was used. Otherwise, the fixed effects model was used. In addition, funnel plots were used to estimate possible publication bias.
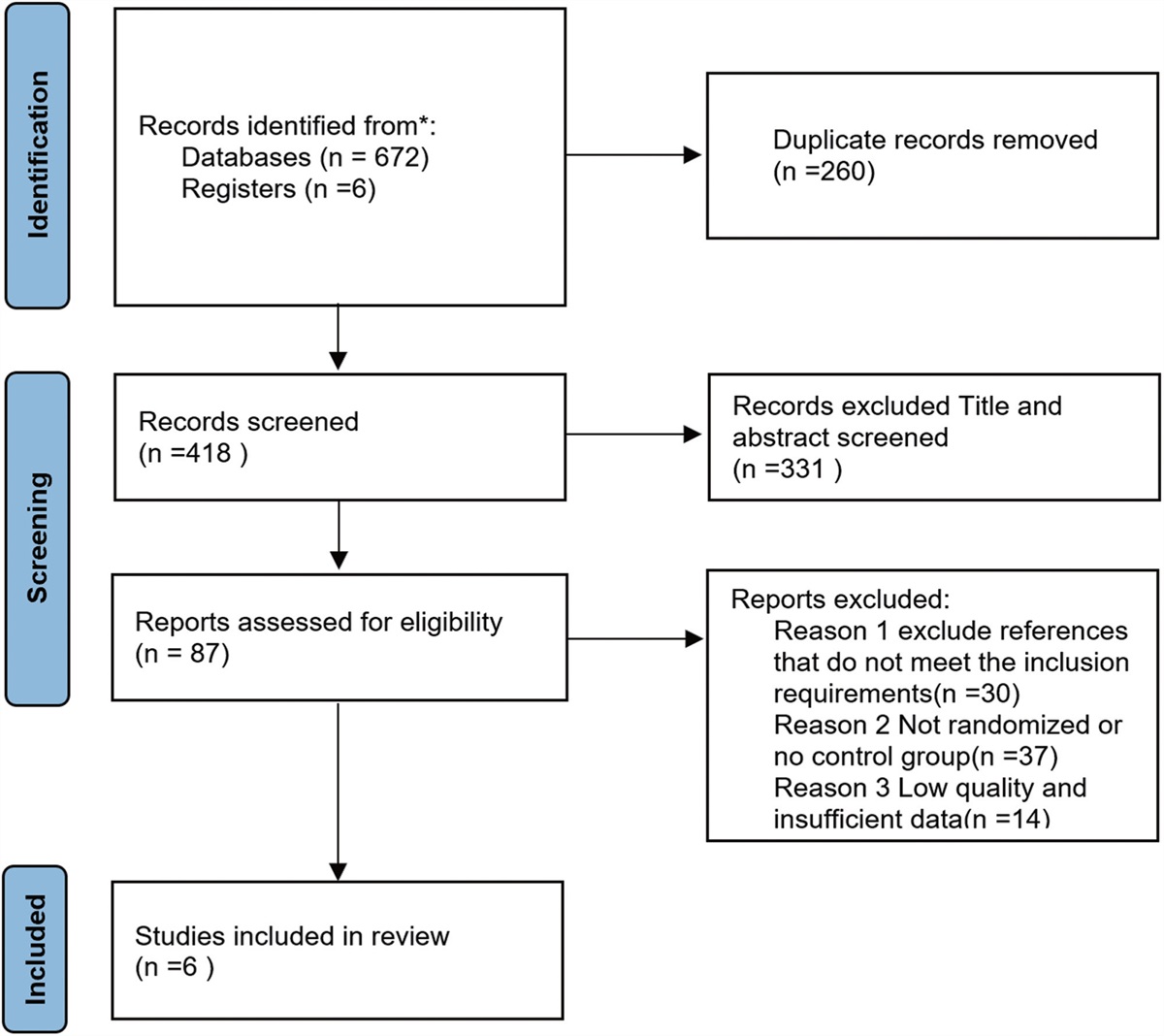
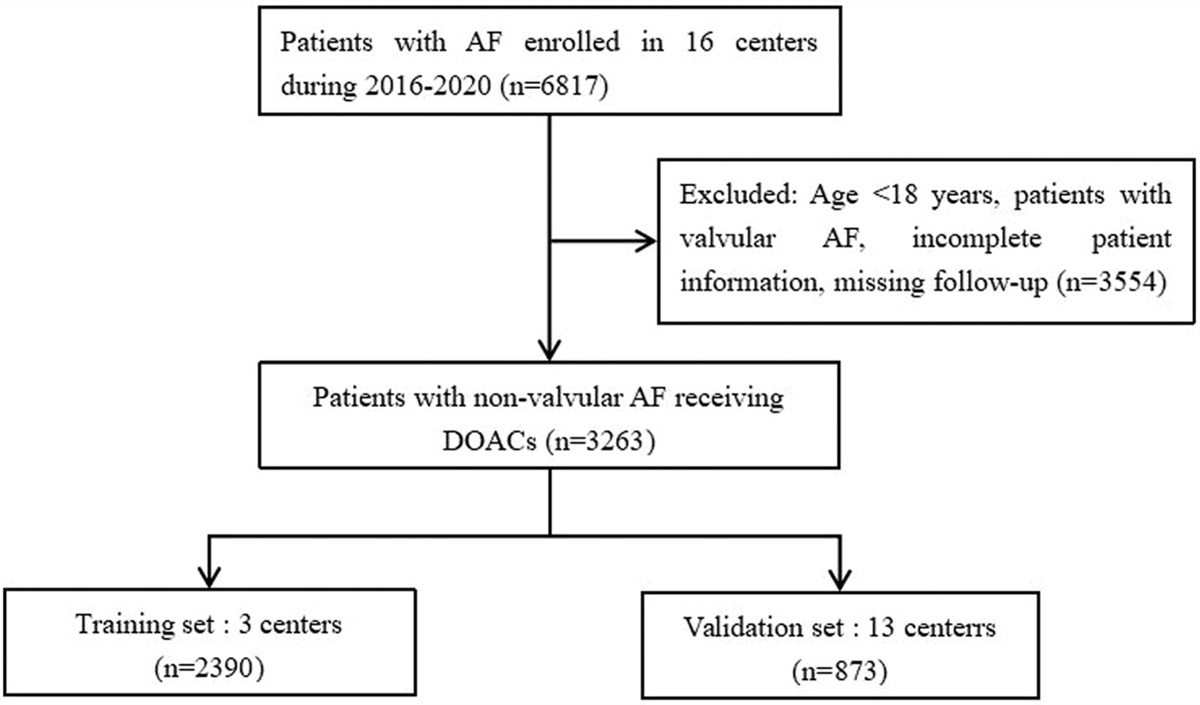
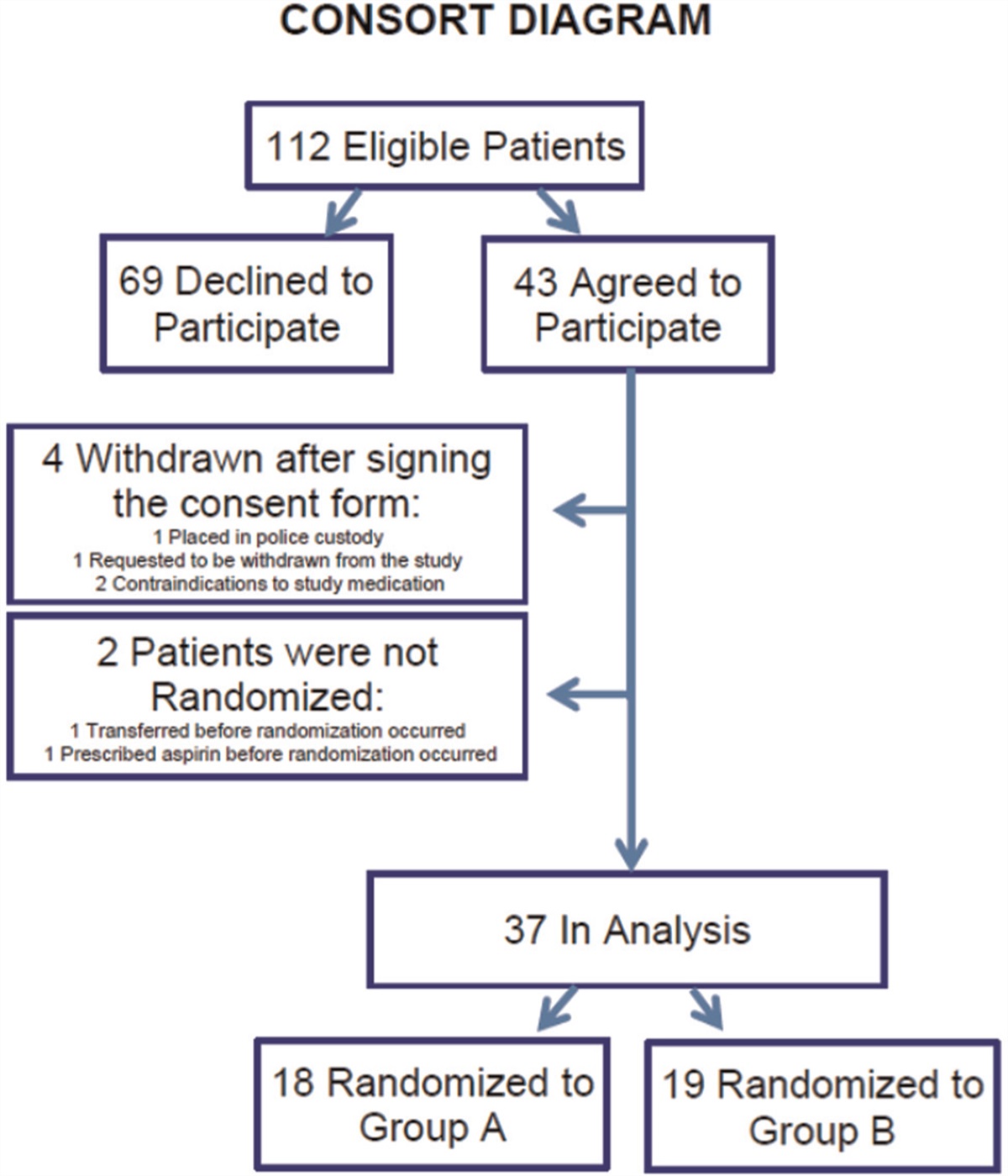
Results Study selection and characteristicsAround 678 records were found through initial searching. Five hundred and ninety-one articles were excluded after removal of duplicates and screening of titles and abstracts according to the inclusion and exclusion criteria. After evaluating the full text, six studies were eventually included in the meta-analysis [11,12,14–17]. The study selection flow chart is shown in Fig. 1.
 Fig. 1:
Fig. 1: Preferred reporting items for systematic reviews and meta-analyses flow chart for article selection.
The basic characteristics of included studies were summarized in Table 1. A total of 23 327 patients were enrolled, including 12 470 in the aspirin group and 10 857 in the LMWH group. Three studies [12,14,15] were from North America, two studies [16,17] were from China and one was from Australia. Three studies [15–17] included patients who underwent TKA only, one study [14] included patients who underwent THA only, and one study [11] included patients who underwent either TKA or THA. Three trials [11,12,15] compared aspirin versus enoxaparin for VTE prophylaxis following orthopaedic surgery, two trials [14,16] compared aspirin versus dalteparin, and one trial [17] did not mention the specific type of LMWH. All studies reported DVT events, and three studies reported PE events. The medication regimen of VTE prophylaxis were shown in Table 2. Aspirin doses ranged from 81 mg once daily to 325 mg twice daily, with duration of treatment ranging from 2 to 5 weeks. LMWH doses ranged from 32 mg once daily to 30 mg twice daily, with duration of treatment ranging from 2 to 5 weeks.
Table 1 - Characteristics of studies Patients Age Studies (first author, year) Year Country Surgical procedure Aspirin LMWH Aspirin LMWH Comparison Follow-up Anderson, 2013 [14] 2013 Canada THA 385 400 57.6 ± 11.9 57.9 ± 12.2 Aspirin vs. dalteparin 90 days Sidhu, 2022 [11] 2022 Australia THA, TKA 5675 4036 67 68 aspirin vs. enoxaparin 90 days O’Toole, 2023 [12] 2023 America, Canada major orthopaedic surgery 6101 6110 44.5 ± 18.0 44.7 ± 17.6 aspirin vs. enoxaparin 90 days Westrich, 2006 [15] 2006 America TKA 139 139 69.0 ± 12.1 68.9 ± 9.6 aspirin vs. enoxaparin 4–6 weeks Zhou, 2023 [16] 2023 China TKA 60 60 66.4 ± 7.6 64.1 ± 6.7 Aspirin vs. dalteparin 90 days Zou, 2014 [17] 2014 China TKA 110 112 62.7 65.7 aspirin vs. LMWH 4 weeksLMWH, low-molecular-weight heparin; THA, total hip arthroplasty; TKA, total knee arthroplasty.
LMWH, low-molecular-weight heparin.
Six of included studies [11,12,14–17] reported VTE events. The rates of VTE events were 459 out of 12 159 (3.8%) in the aspirin group and 288 out of 10 566 (2.7%) in the LMWH group. The pooled result showed that there was a significant difference between the two groups (OR 1.44, 95% CI 1.24–1.68, P < 0.00001, Fig. 2a). the risk of VTE events after orthopaedic surgery in patients receiving aspirin was statistically higher than the risk in patients receiving LMWH. However, given the high heterogeneity of the results, we analysed the two most common thrombotic events, DVT and PE, according to VTE site. There were six [11,12,14–17] and three [11,12,17] of included studies reported DVT and PE events, respectively. The result showed that there was a significant difference between the two groups in DVT events (OR 1.59, 95% CI 1.33–1.91, P < 0.00001, Fig. 2b) while was not in PE events (OR 1.22, 95% CI 0.62–2.40, P = 0.56, Fig. 2c).
 Fig. 2:
Fig. 2: (a) Forest plot of the result comparing aspirin versus low-molecular-weight heparin for venous thromboembolism events. (b) Forest plot of the result comparing aspirin versus low-molecular-weight heparin (LMWH) for DVT events. (c) Forest plot of the result comparing aspirin versus LMWH for PE events. CI, confidence intervals; DVT, deep venous thrombosis; Fixed, a Fixed effects model; M–H, Mantel–Haenszel test; PE, Pulmonary embolism; Random, a random effects model.
Major bleeding eventsFour studies [11,12,14,16] provided data on major bleeding events. There was no significant difference between the aspirin group and the LMWH group (OR 0.95, 95% CI 0.86–1.05, P = 0.33, Fig. 3).
 Fig. 3:
Fig. 3: Forest plot of the result comparing aspirin versus low-molecular-weight heparin for major bleeding events. CI, confidence intervals; Fixed, a Fixed effects model; M–H, Mantel–Haenszel test.
Wound complicationsWound complications were investigated in three studies [12,14,17]. The incidence of wound complications was similar between the groups, and the difference was not statistically significant (OR 0.58, 95% CI 0.28–1.17, P = 0.13, Fig. 4).
 Fig. 4:
Fig. 4: Forest plot of the result comparing aspirin versus low-molecular-weight heparin for wound complications. CI, confidence intervals; Fixed, a Fixed effects model; M–H, Mantel–Haenszel test.
Wound infectionTwo trials [12,14] reported wound infection during the follow-up time. Data from included trials revealed no significant difference between the two groups (OR 1.12, 95% CI 0.86–1.47, P = 0.39, Fig. 5).
 Fig. 5:
Fig. 5: Forest plot of the result comparing aspirin versus low-molecular-weight heparin for wound infection. CI, confidence intervals; M–H, Mantel–Haenszel test; Random, a random effects model.
DeathThree studies [11,12,14] reported the death of patients, and no significant difference was observed between the aspirin group and the LMWH group (OR 1.04, 95% CI 0.70–1.55, P = 0.83, Fig. 6).
 Fig. 6:
Fig. 6: Forest plot of the result comparing aspirin versus low-molecular-weight heparin for death. CI, confidence intervals; Fixed, a Fixed effects model; M–H, Mantel–Haenszel test.
Quality assessmentsThe quality assessment results of RCTs was listed in Fig. 7. Most RCTs had a low risk of bias in seven aspects such as random sequence generation, allocation concealment. Overall, the studies were of intermediate to low risk and of good quality.
 Fig. 7:
Fig. 7: Quality assessment of the included studies.
Sensitivity analysisSensitivity analysis was performed for outcomes with I2 greater than 50%, and after each study was excluded one by one, both I2 and results did not change significantly, suggesting that the meta-analysis was stable and the results were reliable.
Bias analysisFunnel plots of VTE and DVT among the aspirin group and the LMWH group were performed (Supplementary Figure 1, https://links.lww.com/BCF/A172). All studies were included in the funnel plots. Visual inspection of plots for studies of them were symmetrical, which were consistent with Egger regression symmetry tests (VTE: t = −0.59, P = 0.586; DVT: t = −1.21, P = 0.292), demonstrating no statistically significant evidence of publication bias.
DiscussionDue to the damage to the venous blood vessel wall caused by surgical trauma and restrictions of diet and activity, patients who suffered orthopaedic surgery are prone to a hypercoagulable state of blood and eventually DVT events occurred [18,19]. The standardized use of anticoagulants such as aspirin and LMWH can reduce the risk of DVT after surgery, alleviate patients’ pain, and have positive significance in promoting patients’ recovery process and shortening hospitalization time [20–22].
The comparative efficacy of aspirin and LMWH, the two most popular drugs for VTE prevention in recent years, is still controversial. In this study, a meta-analysis of the efficacy of aspirin and LMWH for thromboprophylaxis after orthopaedic surgery was conducted, and the results showed that LMWH was superior to aspirin in preventing VTE, whereas there was no significant difference between them in safety. This result is consistent with the study by Snyder et al.[23]. In addition, we performed a subgroup analysis of VTE events, which showed that compared with aspirin, LMWH was more likely to reduce the incidence of DVT events in orthopaedic surgery patients, whereas there was no advantage in reducing the incidence of PE events.
In this meta-analysis, two important recently published randomized controlled trials [11,12] that included more than 90% of the patients in our systematic evaluation and meta-analysis was included, representing 41.2 and 51.9%, respectively. To date, these two large trials have not been considered in any prior meta and therefore may alter the interpretation of the available data. Notably, the results of them were diametrically opposed. Sidhu et al.[11] observed no difference between aspirin and low-molecular heparin in the prevention of VTE, whereas O’Toole et al.[12] concluded that aspirin was associated with a lower incidence of DVT and PE and a lower 90-day mortality rate. However, regardless of the exclusion of either of these two RCTs, the analysis also demonstrated that there was a statistically significantly difference between LMWH and aspirin, and LMWH owned superiority over aspirin for thromboprophylaxis.
In terms of safety, there were no significant differences in mortality, bleeding events, wound complication and wound infection outcomes between the two drugs, which is similar to the results reported in previous studies [11,12,24–26]. In addition, it has also been shown that aspirin does not increase the risk of transfusion in patients compared with other anticoagulants such as LMWH and rivaroxaban [27].
In the included RCTs, although half of the studies used an aspirin dose of 81 mg twice daily, there were studies that used a nonstandard dose of 100 mg daily and 325 mg twice daily. However, we do not think different doses of aspirin biased our results. In a 3-year retrospective multicentre cohort study by Watts et al.[28], they compared the odds of bleeding and VTE between different aspirin dosages (81, 162, 325, or 650 mg) after lower extremity arthroplasty or revision, and their study showed no significant difference in the rates of bleeding or venous thromboembolism for all aspirin doses. Tang et al.[29] also suggested that the clinical outcomes and safety of the two protocols of aspirin 325 mg twice daily and 81 mg twice daily after knee arthroplasty were similar.
This meta-analysis had several strengths. First of all, this study included several RCTs with larger sample sizes that were never covered by previous studies, thus providing the most comprehensive update on the efficacy and safety of aspirin and LMWH in the prevention of VTE after orthopaedic surgery. Secondly, our article includes only RCT studies, so selection bias was reduced, which made our results more generalizable. Moreover, low or no heterogeneity in the most of the pooled results improved the reliability of our articles.
Of course there were limitations to this article. Due to the limitation of the number of RCTs included, we were unable to perform subgroup analysis on the type of orthopaedic surgery (THR, TKR, etc.), ethnic differences, and type of VTE (symptomatic vs. asymptomatic). In addition, differences in dose and duration of aspirin and LMWH among RCT studies also put the results at risk of bias.
ConclusionThis meta-analysis showed that LMWH was significantly superior to aspirin in thromboprophylaxis after orthopaedic surgery, despite the similar safety profiles. LMWH was still the first-line drug for thrombosis prevention in patients who underwent major orthopaedic surgeries.
AcknowledgementsAvailability of data and materials: all data generated or analysed during this study are included in this published article and its supplementary information files.
Funding: Health Science and Technology Program of Zhejiang Province (2021KY397).
Authors’ contributions: L.Z. and Q.W. collected data, T.W. analysed and interpreted data. H.W. drawn tables and pictures, and was a major contributor in writing the manuscript. S.L. was responsible for revising the article. All authors read and approved the final manuscript.
Conflicts of interestThere are no conflicts of interest.
References 1. Majima T, Oshima Y. Venous thromboembolism in major orthopedic surgery. J Nippon Med School 2021; 88:268–272. 2. Memtsoudis SG, Pumberger M, Ma Y, Chiu YL, Fritsch G, Gerner P, et al. Epidemiology and risk factors for perioperative mortality after total hip and knee arthroplasty. J Orthopaed Res 2012; 30:1811–1821. 3. Simon SJ, Patell R, Zwicker JI, Kazi DS, Hollenbeck BL. Venous Thromboembolism in Total Hip and Total Knee Arthroplasty. JAMA Netw Open 2023; 6:e2345883. 4. Kinov P, Tanchev PP, Ellis M, Volpin G. Antithrombotic prophylaxis in major orthopaedic surgery: an historical overview and update of current recommendations. Int Orthopaed 2014; 38:169–175. 5. Stewart DW, Freshour JE. Aspirin for the prophylaxis of venous thromboembolic events in orthopedic surgery patients: a comparison of the AAOS and ACCP guidelines with review of the evidence. Ann Pharmacother 2013; 47:63–74. 6. Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, et al. Prevention of VTE in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141: (2 Suppl): e278S–e325S. 7. Tang A, Sicat CS, Singh V, Rozell JC, Schwarzkopf R, Long WJ. Aspirin use for venous thromboembolism prevention is safe and effective in overweight and obese patients undergoing revision total hip and knee arthroplasty. J Arthroplasty 2021; 36 (7S):S337–S344. 8. Heckmann ND, Piple AS, Wang JC, Richardson MK, Mayfield CK, Oakes DA, et al. Aspirin for venous thromboembolic prophylaxis following total hip and total knee arthroplasty: an analysis of safety and efficacy accounting for surgeon selection bias. J Arthroplasty 2023. 9. Farey JE, An VVG, Sidhu V, Karunaratne S, Harris IA. Aspirin versus enoxaparin for the initial prevention of venous thromboembolism following elective arthroplasty of the hip or knee: a systematic review and meta-analysis [J]. Orthopaed Traumatol Surg Res 2021; 107:102606. 10. Chen B, Hu N. Low molecular weight heparin and aspirin for prevention of deep vein thrombosisafter orthopaedic surgery: a systematic review and meta-analysis. J Thromb Thrombolysis 2021; 52:553–559. 11. Sidhu VS, Kelly TL, Pratt N, Graves SE, Buchbinder R, Adie S, et al. Effect of aspirin vs enoxaparin on symptomatic venous thromboembolism in patients undergoing hip or knee arthroplasty: the CRISTAL Randomized Trial. JAMA 2022; 328:719–727. 12. O’toole RV, Stein DM, O’hara NN, Frey KP, Taylor TJ, Scharfstein DO, et al. Aspirin or low-molecular-weight heparin for thromboprophylaxis after a fracture. New Engl J Med 2023; 388:203–213. 13. Page MJ, Mckenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372:n71. 14. Anderson DR, Dunbar MJ, Bohm ER, Belzile E, Kahn SR, Zukor D, et al. Aspirin versus low-molecular-weight heparin for extended venous thromboembolism prophylaxis after total hip arthroplasty: a randomized trial. Ann Intern Med 2013; 158:800–806. 15. Westrich GH, Bottner F, Windsor RE, Laskin RS, Haas SB, Sculco TP. VenaFlow plus Lovenox vs VenaFlow plus aspirin for thromboembolic disease prophylaxis in total knee arthroplasty. J Arthroplasty 2006; 21: (6 Suppl 2): 139–143. 16. Zhou LB, Wang CC, Zhang LT, Wu T, Zhang GQ. Effectiveness of different antithrombotic agents in combination with tranexamic acid for venous thromboembolism prophylaxis and blood management after total knee replacement: a prospective randomized study. BMC Musculoskelet Disord 2023; 24:5. 17. Zou Y, Tian S, Wang Y, Sun K. Administering aspirin, rivaroxaban and low-molecular-weight heparin to prevent deep venous thrombosis after total knee arthroplasty. Blood Coagul Fibrinolysis 2014; 25:660–664. 18. Rexiti P, Wutiku M, Wulamu W, Bai F, Cao L. Pulmonary hypertension could be a risk for deep vein thrombosis in lower extremities after joint replacement surgery. Revista da Associacao Medica Brasileira (1992) 2019; 65:946–950. 19. D’astous J, Liederman Z, Douketis JD. Venous thromboembolism prophylaxis in high-risk orthopedic and cancer surgery. Postgrad Med 2021; 133: (Suppl 1): 20–26. 20. Gutiérrez Guisado J. Thromboembolism prophylaxis in orthopaedic surgery and trauma. Revista clinica espanola 2020. 21. Lim PK, Ahn J, Scolaro JA. Venous thromboembolism prophylaxis after pelvic and acetabular fractures: a survey of orthopaedic surgeons’ current practices. J Am Acad Orthopaed Surgeons 2020; 28:750–755. 22. Segon YS, Summey RD, Slawski B, Kaatz S. Surgical venous thromboembolism prophylaxis: clinical practice update. Hospital Pract (1995) 2020; 48:248–257. 23. Snyder MA, Sympson AN, Scheuerman CM, Gregg JL, Hussain LR. Efficacy in deep vein thrombosis prevention with extended mechanical compression device therapy and prophylactic aspirin following total knee arthroplasty: a randomized control trial. J Arthroplasty 2017; 32:1478–1482. 24. Ghosh A, Best AJ, Rudge SJ, Chatterji U. Clinical effectiveness of aspirin as multimodal thromboprophylaxis in primary total hip and knee arthroplasty: a review of 6078 cases. J Arthroplasty 2019; 34:1359–1363. 25. Lindquist DE, Stewart DW, Brewster A, Waldroup C, Odle BL, Burchette JE, El-Bazouni H. Comparison of postoperative bleeding in total hip and knee arthroplasty patients receiving rivaroxaban, enoxaparin, or aspirin for thromboprophylaxis. Clin Applied Thrombosis/Hemostasis 2018; 24:1315–1321. 26. Hovik O, Amlie EJ, Jenssen KK. No Increased risk of venous thromboembolism in high-risk patients continuing their dose of 75 mg aspirin compared to healthier patients given low-molecular-weight heparin. J Arthroplasty 2021; 36:3589–3592. 27. Yhim HY, Lee J, Lee JY, Lee JO, Bang SM. Pharmacological thromboprophylaxis and its impact on venous thromboembolism following total knee and hip arthroplasty in Korea: a nationwide population-based study. PLoS One 2017; 12:e0178214. 28. Watts PJ, Kopstein M, Harkness W, Cornett B, Dziadkowiec O, Jenkins P, et al. A retrospective analysis comparing post-operative bleeding with various doses of aspirin after lower extremity joint arthroplasty or revision. Pharmacotherapy 2021; 41:616–622. 29. Tang A, Zak SG, Waren D, Iorio R, Slover JD, Bosco JA, Schwarzkopf R. Low-dose aspirin is safe and effective for venous thromboembolism prevention in patients undergoing revision total knee arthroplasty: a retrospective cohort Study. J Knee Surg 2022; 35:553–559.
留言 (0)