P ediatric Critical Care Medicine (PCCM) publishes many Editorials; the median number (interquartile range) per month for 2021 to 2023, was five (4 to 6). These items are written about 3,000-word Clinical Research Articles (1) and 1,500-word Brief Reports (2) and are published because reviewers tell us that the work needs more discussion. So, when does PCCM decide to have an editorial; who is asked to write; and, for future authors, how should an editorial be structured? These questions will be answered in this fifth article in the PCCM’s series called “Writing for PCCM” (1–4).
EDITORIALS
When Does PCCM Seek an Editorial?
The “when” is also a “why” question for the PCCM editorial team. Usually, the reviewer (often an Editorial Board member (5–7)) alerts the team that an article needs some additional clarification for readers. This advice commonly falls into one of five categories (8,9), and for those wanting to learn about writing each of these formats is described here, along with good examples in PCCM.
First, a PCCM reviewer may think that the findings in an article needs more explanation, even to the extent of going beyond the authors’ conclusions. For example, consider the 2022 two-center, retrospective cohort (2010−2018) study about excessive oxygen supplementation in the first day of mechanical ventilation and the observation that this metric was associated with multiple organ dysfunction and death in critically ill children (10). The accompanying editorial provided an explanation for this observation with a Figure showing a possible causal model of oxygen administration and severity of organ failure (11). Additionally, the editorial went beyond the “simple causal path between hyperoxia and poor outcomes via oxidative injury” and described risks and benefits of different levels of oxygenation. In fact, these experts also told readers about their ongoing multicenter randomized controlled trial (RCT) of conservative versus liberal peripheral oxygenation targets. The protocol for the RCT was published later in 2022 (12), and the trial result was presented in the Lancet in January 2024 (13). In summary, this editorial format adds value by not only explaining content, but also giving readers material that extends the content with unique insight or experience.
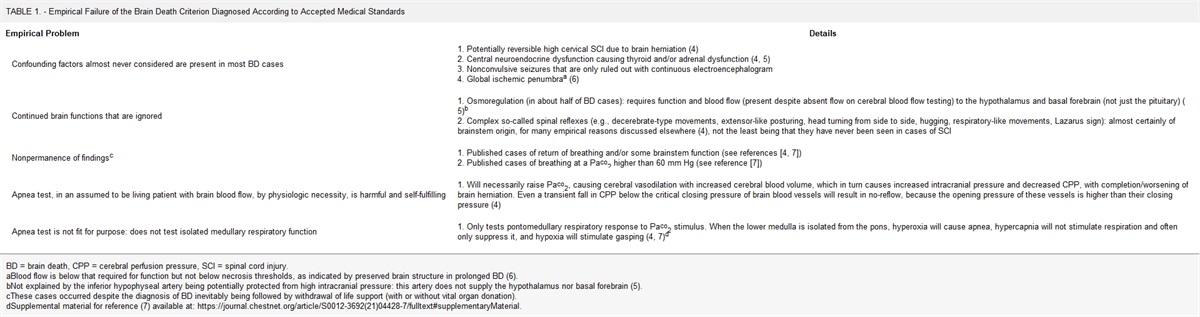
Second, a reviewer may consider that an article warrants a robust critique for readers because their own position–and reason for an editorial–is different to that taken by the authors. As an example, read the 2023 single-center, retrospective cohort (2013−2020) analysis of adverse events during apnea testing for the determination of death using neurologic criteria (14). The authors focused on the overall adverse event rate of 20%, with premature termination of the apnea test in 5%; there was no analysis of consent for such testing, but it was mentioned in the discussion. The accompanying editorial served as a literary vehicle for examining problems with the apnea test (15). It also focused on the issue of consent and made readers think about whether we were “asking the wrong question”; that is, why is there an apnea test in the protocol for determination of death using neurologic criteria? This type of editorial is in the form of a dialectical argument or open debate and, typically, would be written by someone with publications in this area, as is evident with this expert (16–18).
Third, a reviewer may consider that an article needs to be more fully described because the analysis is timely, or highly topical. In 2022, PCCM published a single-center, retrospective cohort (2013−2018) study describing the association between various pulmonary physiologic metrics during mechanical ventilation and outcome of severe pediatric acute respiratory distress syndrome (PARDS) (19). One of these metrics was “mechanical power” (i.e., the theoretical mechanical energy load exerted on lung tissue), which had primarily been validated in adult patients. The editorial provided readers with an expert account and asked, “should we embrace mechanical power…?” (20). The timeliness of the article and editorial was borne out by subsequent articles covering clinician guidance, education, and research about the use of the mechanical power metric in PARDS management (21–23).
Fourth, a reviewer may think it worthwhile to reflect on some newly implemented innovation. In 2023, PCCM published a single-center, mixed-methods quality improvement cohort (2020−2021) study that used an algorithm to evaluate PICU patients with new fever or instability (24). The editorial (25) introduced readers to the interplay between antibiotic and diagnostic stewardship, and asked whether we can “change the culture around fever in the PICU?” Of course, this play on words had more serious intent. In fact, the editorial also supported PCCM’s narrative about network research focused on the fields of quality improvement and implementation science (26–28).
The final category of editorial speaks to PCCM’s mission and vision as an international journal (29): a reviewer may want to comment on applied research in another resource setting. In 2023, PCCM published the findings of a single-center, prospective cohort (2020−2022) study in Pakistan (30). Here, the authors described the prognostic performance of the second version of the Pediatric Sepsis Biomarker Risk Model (PERSEVERE-II) in septic children. The accompanying editorial not only gave readers more insight into PICU practice in Pakistan, but it also highlighted potential scope for international collaboration (31).
Who is Asked to Write an Editorial?
The writers of PCCM’s editorials are experts in the field who have reviewed for the Journal, have demonstrated in-depth knowledge, and are considered thought leaders, as the examples above will attest. Over the three years, 2021−2023, more than 500 individuals have reviewed for PCCM, and the editorial team selected 174 to lead the authorship of an editorial (5–7). Overall, the female-to-male ratio of reviewer’s gender-tagged names was 0.8:1, which was equivalent to the 0.8:1 ratio of PCCM’s lead author editorial writers.
What is the Structure of a PCCM Editorial?
The PCCM editorial should be a concise, engaging, thoughtful, and scholarly portrayal of an argument that uses scientific observation, or interpretation and application, to lead to conclusions that are clinically relevant. Do this in 1,200 to 1,500 words with up to 15 references.
The editorial’s title needs to have an obvious link with the article about which it is written. A common structure is in two parts, each separated by a colon. For example, Topic area <colon> subtitle or question to signal the focus. Try not to use obscurely worded, complicated, or frivolous titles, because one consequence may be that the editorial is not identified as being linked to a particular article in the National Library of Medicine database. That is, the editorial will be separated from the article because it is not added to the “Comment in” section of the article’s PubMed listing. Hence, a bibliographic search may not disclose the existence of that article’s editorial.
The body of the text has four sections (32,33). First, a short introductory paragraph that describes the issue, problem, or topic of the paper. Any comments or statements about background data should cite references.
The second paragraph is where a summary of the article’s findings, and strengths are presented. It is not necessary to praise an article, just focus on the facts in sufficient detail (e.g., design, numbers, and key outcomes) to help readers to understand the editorial without going back to the article. Then, describe any limitations, especially those not mentioned by the authors. Remember to keep your language consistent with the design of the study. Because most of PCCM’s clinical research reports are retrospective accounts, the text will require noncausal language of association (1,2). Also, as recommended by the British Journal of Anaesthesia, write with G-R-A-C-E (33), that is: be Gracious with respect for authors; be Relevant for readers in your opinions about the article; be Accurate in your use of the article and references; be Controversial–meaning provide some thoughtful focus on contemporary debate, or viewpoints; and be Engaging in your writing style.
The third paragraph is where you provide details of the issue that stimulated the editorial (as covered in the section on “When Does PCCM Seek an Editorial?”). Here, identify the point(s) you want to raise in a balanced manner and avoid presenting an idiosyncratic perspective, or anecdotes. Sometimes your argument may need an illustration. See the first example above about providing “more explanation” and the use of a Figure about causal pathways (11). Alternatively, you may have the opportunity to graph original data. For example, PCCM published an article that used the United States Pediatric Health Information System database (2009−2019) to describe rising hospital charges in PICU patients with bronchiolitis (34). The accompanying editorial from Australia included a graph of 2011−2018 and 2020 Australia and New Zealand PICU data that also showed rising costs (35). The illustrations supported a discussion about whether these costs could be attributed to the increasing numbers of PICU admissions using nasal high-flow support.
The last section or paragraph needs a strong, evidence-based conclusion. Point to any next steps in research, or unresolved questions, and make sure that readers have a clear take-home message.
Finally, use references to support your points. In an editorial, these citations should have been published in the last 3 or 4 years. If they are older than that, then rethink whether an editorial is necessary. The point is that the editorial is highlighting a contemporary discussion and narrative for readers of PCCM, and not presenting a review. Incidentally, if you are not engaging in the PCCM narrative, then you may need to check whether you have crafted something that is for another audience, and not PCCM readers (4). However, please do not let these comments deter you from using a wide range of reference material, because we do want PCCM readers to be informed of important, contemporary, and useful content.
COMMENTARIES
Commentaries are a form of editorial writing and PCCM has started to publish these articles. The main purpose of this material is to discuss the implication of research articles that have not been published in the Journal. We may also expand the scope to include items that were previously called PCCM Perspectives.
Everything written about writing an Editorial applies to writing a Commentary, and authors are selected because we want to read their viewpoint. In essence, this material is written like a periodical’s “op-ed” (i.e., item placed on the page opposite the main editorials), and there are various techniques that can be used to interest and engage readers (36).
As an example, consider two RCTs published in the Journal of the American Medical Association, in 2022 (37,38). The First-Line Support for Assistance in Breathing in Children (FIRST-ABC) trials compared high-flow nasal cannula therapy and continuous positive airway pressure support in critically ill children, either in the acute setting (step-up RCT) or in the postextubation setting (step-down RCT). In December 2022, PCCM published two commentaries about these RCTs in a pro et contra (pro vs con) format. One commentary was written by the FIRST-ABC investigators (39), and the Journal asked them “how are you translating the RCT findings to your practice?” The other commentary was written by established PCCM editorialists (40), and the Journal asked them “now that you have the RCTs that you previously called for, what is your view about applying these new data?”
Later this year we will have two more commentaries about the multicenter trial of conservative versus liberal oxygenation targets in critically ill children that was published in the Lancet in January 2024 (12,13).
REFERENCES
1. Tasker RC: Writing for PCCM: The 3,000-word structured clinical research report. Pediatr Crit Care Med. 2021; 22:312–317
2. Tasker RC: PCCM narratives, letters, and correspondence. Pediatr Crit Care Med. 2021; 22:426–427
3. Tasker RC: Writing for PCCM: Instructions for authors. Pediatr Crit Care Med. 2022; 23:651–655
4. Tasker RC: Writing for Pediatric Critical Care Medicine: Engaging with citations to references in the Chatbot Generative Pre-Trained Transformer era. Pediatr Crit Care Med. 2023; 24:862–868
5. Tasker RC: 2021 in review. Pediatr Crit Care Med. 2021; 22:1009–1010
6. Tasker RC: 2022 in review. Pediatr Crit Care Med. 2022; 23:961–963
7. Tasker RC: 2023 in review. Pediatr Crit Care Med. 2023; 24:979–982
8. van Teijlingen ER, Hundley V, Sathian B, et al.: The art of the editorial. Nepal J Epidemiol. 2022; 12:1135–1138
9. Nundy S, Kakar A, Bhutta ZA: How to write an editorial? In: How to practice academic medicine and publish from developing countries? Springer, Singapore, 2022. Available at:
https://doi.org/10.1007/978-981-16-5248-6_26. Accessed February 1, 2024
10. Balcarcel DR, Coates BM, Chong G, et al.: Excessive oxygen supplementation in the first day of mechanical ventilation is associated with multiple organ dysfunction and death in critically ill children. Pediatr Crit Care Med. 2022; 23:89–98
11. Jones GAL, Peters MJ: Towards causality with liberal oxygen use? Pediatr Crit Care Med. 2022; 23:135–137
12. Chang I, Thomas K, O’Neill Gutierrez L, et al.: Protocol for a randomized multiple center trial of conservative versus liberal oxygenation targets in critically ill children (Oxy-PICU): Oxygen in pediatric intensive care. Pediatr Crit Care Med. 2022; 23:736–744
13. Peters MJ, Gould DW, Ray S, et al.; Oxy-PICU Investigators of the Paediatric Critical Care Society Study Group (PCCS-SG): Conservative versus liberal oxygenation targets in critically ill children (Oxy-PICU): A UK multicenter, open, parallel-group, randomised clinical trial. Lancet. 2024; 403:355–364
14. Sveen WN, Matheny Antommaria AH, Gilene SJ, et al.: Adverse events during apnea testing for the determination of death by neurological criteria: A single-center, retrospective pediatric cohort. Pediatr Crit Care Med. 2023; 24:399–405
15. Joffe AR: Consent for the apnea test: Asking the wrong question. Pediatr Crit Care Med. 2023; 24:427–429
16. Joffe AR, Anton R, Duff JP: The apnea test: Rationale, confounders, and criticism. J Child Neurol. 2010; 25:1435–1443
17. Joffe AR: The apnea test: Requiring consent for a test that is a self-fulfilling prophesy, not fit for purpose, and aways confounded? Am J Bioeth. 2020; 20:42–44
18. Joffe AR, Hansen G, Tibballs J: The world brain death project: The more you say it does not make it true. J Clin Ethics. 2021; 32:97–108
19. Proulx F, Emeriaud G, Francois T, et al.: Oxygenation defects, ventilation ratio, and mechanical power during severe pediatric acute respiratory distress syndrome: Longitudinal time sequence analyses in a single-center retrospective cohort. Pediatr Crit Care Med. 2022; 23:22–33
20. Khemani RG: Should we embrace mechanical power to understand the risk of ventilator-induced lung injury in children? Pediatr Crit Care Med. 2022; 23:71–74
21. Fernandez A, Modesto V, Rimensberger PC, et al.; Second Pediatric Acute Lung Injury Consensus Conference (PALICC-2) of the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network: Second Pediatric Acute Lung Injury Consensus Conference (PALICC-2) of the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network: Invasive ventilatory support in patients with pediatric acute respiratory distress syndrome: From the second Pediatric Acute Lung Injury Consensus Conference. Pediatr Crit Care Med. 2023; 24:S61–S75
22. Cruces P: Pediatric acute respiratory distress syndrome: Approaches in mechanical ventilation. Pediatr Crit Care Med. 2023; 24:e104–e114
23. Percy AG, Mai MV, Bhalla AK, et al.: Mechanical power is associated with mortality in pediatric acute respiratory distress syndrome. Pediatr Crit Care Med. 2023; 24:e307–e316
24. Sick-Samuels AC, Booth LD, Milstone AM, et al.: A novel comprehensive algorithm for evaluation of PICU patients with new fever or instability. Pediatr Crit Care Med. 2023; 24:670–680
25. Karube T, Karsies TJ: Can we change the culture around fever in the PICU? Pediatr Crit Care Med. 2023; 24:705–707
26. Randolh AG, Bembea MM, Cheifetz IM, et al.: Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network: Pediatric Acute Lung Injury and Sepsis Investigators (PALISI): Evolution of an investigator-initiated research network. Pediatr Crit Care Med. 2022; 23:1056–1066
27. Bartman T, Brilli RJ: Quality improvement studies in pediatric critical care medicine. Pediatr Crit Care Med. 2021; 22:662–668
28. Woods-Hill CZ, Wolfe H, Malone S, et al.; Excellence in Pediatric Implementation Science (ECLIPSE) for the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network: Implementation science research in pediatric critical care medicine. Pediatr Crit Care Med. 2023; 24:943–951
29. Tasker RC: Pediatric Critical Care Medicine 2021: The five Rs. Pediatr Crit Care Med. 2021; 22:1–2
30. Ishaque S, Famularo ST 3rd, Saleem AF, et al.: Biomarker-based risk stratification in pediatric sepsis from a low-middle income country. Pediatr Crit Care Med. 2023; 24:563–573
31. Mount MC, Remy KE: Help wanted for sepsis: Biomarkers in low- and middle-income countries please apply. Pediatr Crit Care Med. 2023; 24:619–621
32. Fontanarosa PB: Editorial matters: Guidelines for writing effective editorials. JAMA. 2014; 311:2179–2180
33. Leslie K, Hemmings HC Jr: Excellence in editorials: Fulfilling their critical role in the medical literature. Br J Anaesth. 2020; 125:639–641
34. Slain KN, Malay S, Shein SL: Hospital charges associated with critical bronchiolitis from 2009 to 2019. Pediatr Crit Care Med. 2022; 23:171–180
35. Franklin D, Schibler A: Rising intensive care costs in bronchiolitis infants – is nasal high flow the culprit? Pediatr Crit Care Med. 2022; 23:218–222
36. Farid H, Kanjee Z, Huang GC: Writing an Op-Ed for a lay audience: How to captivate readers and change the world. Acad Med. 2023; 98:1231
37. Ramnarayan P, Richards-Belle A, Drikite L, et al.; FIRST-ABC Step-Up RCT Investigators and the Paediatric Critical Care Society Study Group: Effect of high-flow nasal cannula therapy vs continuous positive airway pressure therapy on liberation from respiratory support in acutely ill children admitted to pediatric critical care unites: A randomized clinical trial. JAMA. 2022; 328:162–172
38. Ramnarayan P, Richards-Belle A, Drikite L, et al.; FIRST-ABC Step-Down RCT Investigators and the Paediatric Critical Care Society Study Group: Effect of high-flow nasal cannula therapy vs continuous positive airway pressure following extubation on liberation from respiratory support in critically ill children: A randomized clinical trial. JAMA. 2022; 327:1555–1565
39. Ramnarayan P, Peters MJ: Commentary on the first-line support for assistance in breathing in children trials on noninvasive respiratory support: Taking a closer look. Pediatr Crit Care Med. 2022; 23:1084–1088
40. Shein SL, Kneyber MCJ, Rotta AT: Commentary on high-flow nasal cannula and continuous positive airway pressure practices after the first-line support for assistance in breathing in children trials. Pediatr Crit Care Med. 2022; 23:1076–1083




留言 (0)