The landscape of decision-making in contemporary pediatric critical care is extraordinarily complex, yet decision-making is a ubiquitous component of clinical practice (1). Confounding the difficulties inherent in time-sensitive crises surrounding the life and death of a child, medical and technological advances have widened therapeutic options. With prognostic uncertainty common and a paucity of quality evidence directly applicable in many clinical scenarios, ethical tensions may become amplified (1). Media, social media, and other online resources offer varying degrees of information/misinformation. Additionally, social stressors are often heightened in the context of critical illness and impact both families and clinicians (2). The locus of decision-making has also shifted over several decades from a physician-centered approach toward patients and families having greater expectations of participating in their care. Recent expert consensus statements endorse shared decision-making (SDM) as the recommended model in pediatrics (3–5). SDM promotes recognition that a child’s interests as well as a family’s values, preferences, and goals are of critical relevance in making decisions that impact their lives. Equally vital is clinicians’ active participation in SDM (6). SDM requires a partnership, an exchange of information, medical contextualization to inform understanding, and discussion as well as building of values along the illness trajectory to allow clinicians to make goal-concordant recommendations where necessary (6–8).
With this background, in the issue of Pediatric Critical Care Medicine, the article by Olive et al (9) assesses one way that clinicians can influence decision outputs in PICU family meetings by describing the concept of nudging. Nudging is a form of choice architecture in which how options are presented predictably increases the likelihood of a specific decision outcome, with the intention to influence but not coerce (10). The use of nudging as a technique in decision-making with adult patients has been more robustly studied, however, given the substantial differences in decision-making between adults and pediatrics, translatability from the adult context is limited (10). Existing pediatric literature on nudging is restricted to discussions of applications in the Neonatal ICU for framing tracheostomy decisions (11), with no data examining the use of this technique in PICU environments. As a result, this study by Olive et al (9) represents a novel analysis and characterization of the role of nudging in pediatric critical care decision-making.
Olive et al (9) used a unique data set of transcribed care conferences to characterize the use of 17 specific types of nudging in 11 categories of decision-making, ranging from discussions of laboratory tests and procedures to goals of care and candidacy for extracorporeal support. Nudging was used frequently across a spectrum of decision types by clinicians, with a median of 8 (interquartile range, 6–10) nudging types per conference. While these were PICU meetings, attending intensivists were the specialty who employed nudging the most; in more than 90% of the conferences attended. Certain types of nudging were more common, with framing of outcomes using positive and negative language the most common type. Interestingly, nudging types described by the authors range substantially in both “avoidability” and subtlety. Framing, for example, contains subcategories of gain, loss, and mixed types so presentation of data related to predicted mortality outcomes will unavoidably fall into one of these categories (60% survival vs. 40% mortality vs. both); a frameless presentation of the data is impossible by this definition. This is likely an explanation for the overall high frequency of nudging techniques observed in the PICU context. Simultaneously, framing is both an unavoidable form of nudging and one of the most subtle—the choice impact of this most frequently used nudging technique is likely imperceptible to the listener. In comparison, other nudging techniques such as recommendations by directive counseling or overt omission are more explicit in their choice architecture. As such, while all forms of nudging may be justified in different circumstances, the ethical implications vary between types, and so utilization of this strategy warrants deeper consideration.
IMPLICATIONS
Influences on decision-making are omnipresent and frequently unrecognized, from media advertising to how grocery stores display goods. Human beings use similar techniques in all forms of communication, including with our colleagues and loved ones, and thus nudging in some form is likely used subconsciously by the vast majority of practicing pediatric critical care clinicians in communication with families (10). Study findings illuminate key practice implications to fulfill our professional responsibilities as clinicians and ensure ethically supported decisions are made. Methodological limitations highlight the need for caution in indiscriminate application of techniques like nudging, or at minimum for clinicians to be cognizant of the drawbacks. This is particularly important as clinicians are human with our own values, implicit biases, and differential communication skills.
SDM approaches vary based on geographical location, clinical scenario, age, and family preferences, however, they are also substantially influenced by clinician perceptions and values (6–8). As the authors recognize, their analysis is unable to determine “intentionality” in the observed nudging and one may consider this to be a critical component in the ethical analysis of such conversations and choice architecture. Given clinicians own values and past experiences, there is likely no feasible means for clinical communication to be “nudge-less.” However, the mindful use or avoidance of nudging that stems from personal rather than professional values or reflects implicit bias is crucial. Nudging is most likely to be both effective and ethically permissible if clinicians first establish a therapeutic relationship and build trust. Patient and/or family goals should be explored and understood before it is possible to provide value-based recommendations and guide a decision (8). The medical profession needs to be cautious to avoid value imposition, that is to not impose liberal individual values on an exceptionally values-pluralistic society which risks exacerbation of existing deep divisions (12). With moral differences being inherent to population diversity, families may have different values from their medical team (12). Influencing without first listening for, and respecting values is not nudging (10). The “outlier conference” described by Olive et al (9), highlights this point. This single care conference had an astounding 57 instances of nudging in a discussion involving just two decision categories. The outcome of this conference is not presented, nor is information regarding parental perceptions of the communication episode and their satisfaction or regret with their ultimate decision. However, the question is raised—when does a nudge become a shove? Where is the line between reasonable, informed persuasion and coercion? (10)
Bias is pervasive in clinical practice so it should be noted that the study sample size was small and highly restrictive. Only English-speaking families were included. Nudging requires nuance and precision with language, including body language and word choice, which may be lost through use of translation services. Despite this, clinicians must attempt to bridge cultural and communication divides. In the parent study from which the audio transcripts were recorded (13), several families declined participation because they felt “emotionally overwhelmed.” An additional subset of parents were not approached for consent due to concerns for psychological instability and legal involvement. Although not included in the study, critical care clinicians must still engage with families managing such stressors during periods of crisis. Families with less resources and advocacy skills are often the most susceptible to undue influence. It is the clinician’s responsibility to recognize contexts when nudging should be used with restraint to avoid manipulation and coercion, with balancing parameters needed to protect more vulnerable families from bias and value imposition (10,12,14).
At the same time, transparency and honesty in conversations are essential, and clinicians must always actively participate in SDM (6,7). SDM exists on a spectrum—for some decisions, complete deference is afforded to parents after appropriate medical contextualization, whereas for others more directive medical recommendations are ethically justified and preferable (7,8). Parent surveys support this, valuing equal clinician input in SDM across a range of different decisions (6). A recent observational study analyzing decisional preferences found the characteristics associated with families favoring greater weight of clinician influence on decision-making to be increased perceived medical expertise needed, urgency, and clinical benefit (6). The specific approach must be tailored to the unique context of each decision, though there is disappointingly limited practical, implementation-level guidance for ethically supported decision-making for critically ill children (1,3,4). Ethically permissible nudging is nuanced (10) and high-quality communication must be a core competency for pediatric critical care clinicians. These are techniques and skills to be learned and practiced. Nudging is just one tool available in our communication armamentarium for effective participation in SDM.
FUTURE DIRECTIONS
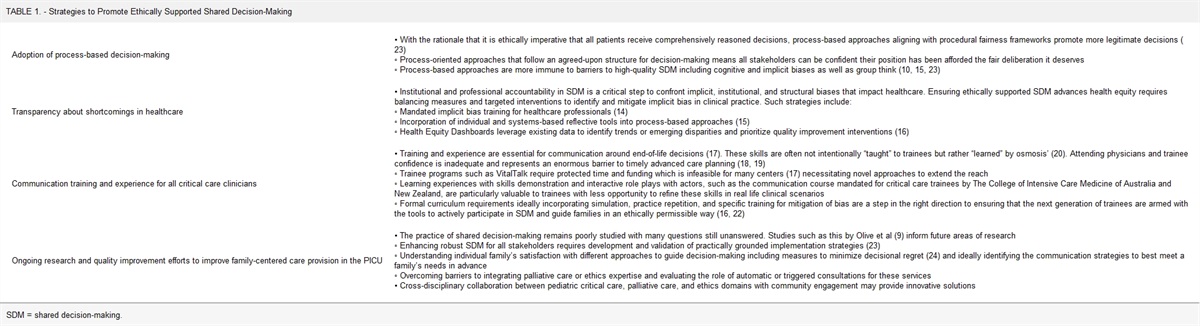
Looking forward to potential solutions requires clinicians to acknowledge our human vulnerabilities, gain insights into them, and institute measures to protect against them. These are key steps to making ethically supported decisions and improving societal trust in medical decision-making. Some strategies to encourage robust decision-making as described in the literature are shown (Table 1). These include implementing process-based approaches to decision-making, increasing transparency about shortcomings in healthcare with health equity dashboards, mandatory implicit bias as well as communication skills training, efforts to improve family-centered care provision in PICUs, and ongoing research including efforts to enhance practical implementation of SDM at the bedside (14–24).
TABLE 1. -
Strategies to Promote Ethically Supported Shared Decision-Making
Adoption of process-based decision-making
• With the rationale that it is ethically imperative that all patients receive comprehensively reasoned decisions, process-based approaches aligning with procedural fairness frameworks promote more legitimate decisions (
23)
◦ Process-oriented approaches that follow an agreed-upon structure for decision-making means all stakeholders can be confident their position has been afforded the fair deliberation it deserves
◦ Process-based approaches are more immune to barriers to high-quality SDM including cognitive and implicit biases as well as group think (
10,
15,
23)
Transparency about shortcomings in healthcare
• Institutional and professional accountability in SDM is a critical step to confront implicit, institutional, and structural biases that impact healthcare. Ensuring ethically supported SDM advances health equity requires balancing measures and targeted interventions to identify and mitigate implicit bias in clinical practice. Such strategies include:
◦ Mandated implicit bias training for healthcare professionals (
14)
◦ Incorporation of individual and systems-based reflective tools into process-based approaches (
15)
◦ Health Equity Dashboards leverage existing data to identify trends or emerging disparities and prioritize quality improvement interventions (
16)
Communication training and experience for all critical care clinicians
• Training and experience are essential for communication around end-of-life decisions (
17). These skills are often not intentionally “taught” to trainees but rather “learned” by osmosis’ (
20). Attending physicians and trainee confidence is inadequate and represents an enormous barrier to timely advanced care planning (
18,
19)
◦ Trainee programs such as VitalTalk require protected time and funding which is infeasible for many centers (
17) necessitating novel approaches to extend the reach
◦ Learning experiences with skills demonstration and interactive role plays with actors, such as the communication course mandated for critical care trainees by The College of Intensive Care Medicine of Australia and New Zealand, are particularly valuable to trainees with less opportunity to refine these skills in real life clinical scenarios
◦ Formal curriculum requirements ideally incorporating simulation, practice repetition, and specific training for mitigation of bias are a step in the right direction to ensuring that the next generation of trainees are armed with the tools to actively participate in SDM and guide families in an ethically permissible way (
16,
22)
Ongoing research and quality improvement efforts to improve family-centered care provision in the PICU
• The practice of shared decision-making remains poorly studied with many questions still unanswered. Studies such as this by Olive et al (
9) inform future areas of research
◦ Enhancing robust SDM for all stakeholders requires development and validation of practically grounded implementation strategies (
23)
◦ Understanding individual family’s satisfaction with different approaches to guide decision-making including measures to minimize decisional regret (
24) and ideally identifying the communication strategies to best meet a family’s needs in advance
◦ Overcoming barriers to integrating palliative care or ethics expertise and evaluating the role of automatic or triggered consultations for these services
• Cross-disciplinary collaboration between pediatric critical care, palliative care, and ethics domains with community engagement may provide innovative solutions
SDM = shared decision-making.
REFERENCES
1. Moynihan KM, Clark JD, Dorste A, et al.: Ethical guidance for extracorporeal and paracorporeal device use in children: A systematic review. Intensive Care Med Paediatr Neonatal 2024 Jan 18. [online ahead of print]
2. Basu S, Preisz A: Family conflict and aggression in the paediatric intensive care unit: Responding to challenges in practice. Clinical Ethics. 2022; 18:410–417
3. Eaton SM, Clark JD, Cummings CL, et al.: Pediatric shared decision-making for simple and complex decisions: Findings from a delphi panel. Pediatrics. 2022; 150:e2022057978
4. Salter EK, Hester DM, Vinarcsik L, et al.: Pediatric decision making: Consensus recommendations. Pediatrics. 2023; 152:e2023061832
5. Kon AA, Davidson JE, Morrison W, et al.; American College of Critical Care Medicine: Shared decision making in ICUs: An American College of Critical Care Medicine and American Thoracic Society Policy Statement. Crit Care Med. 2016; 44:188–201
6. Tadros HJ, Saidi A, Rawlinson AR, et al.: Assessment of parental decision making in congenital heart disease, cardiomyopathy and heart transplantation: An observational study analysing decisional characteristics and preferences. Arch Dis Child. 2023; 108:641–646
7. Morrison W, Clark JD, Lewis-Newby M, et al.: Titrating clinician directiveness in serious pediatric illness. Pediatrics. 2018; 142:S178–S186
8. Moynihan KM, Jansen MA, Liaw SN, et al.: An ethical claim for providing medical recommendations in pediatric intensive care. Pediatr Crit Care Med. 2018; 19:e433–e437
9. Olive AM, Wagner AF, Munhall DT, et al.: Nudging During Pediatric Intensive Care Conferences With Family Members: Retrospective Analysis of Transcripts From a Single-Center, 2015-2019. Pediatr Crit Care Med. 2024; 25:407–415
10. Blumenthal-Barby J, Opel DJ: Nudge or grudge? Choice architecture and parental decision-making. Hastings Cent Rep. 2018; 48:33–39
11. Blumenthal-Barby JS, Loftis L, Cummings CL, et al.: Should neonatologists give opinions withdrawing life-sustaining treatment? Pediatrics. 2016; 138:e20162585
12. Fiester A: Reducing moral distress by teaching healthcare providers the concepts of values pluralism and values imposition. J Clin Ethics. 2023; 34:296–306
13. October TW, Dizon ZB, Arnold RM, et al.: Characteristics of physician empathetic statements during pediatric intensive care conferences with family members: A qualitative Study. JAMA Netw Open. 2018; 1:e180351
14. Cooper LA, Saha S, Van Ryn M: Mandated implicit bias training for health professionals—a step toward equity in health care. JAMA Health Forum. 2022; 3:e223250
15. Kirby L, Basu S, Close E, et al.: Rationing in the pediatric intensive care unit—ethical or unethical? Transl Pediatr. 2021; 10:2836–2844
16. Hester G, Nickel AJ, Griffin KH: Accountability through measurement: Using a dashboard to address pediatric health disparities. Pediatrics. 2020; 146:e2020024448
17. VitalTalk.org. Vital Talk Resources: Learn skills that matter.
18. Sulmasy DP, Sood JR, Ury WA: Physicians’ confidence in discussing do not resuscitate orders with patients and surrogates. J Med Ethics. 2008; 34:96–101
19. Durall A, Zurakowski D, Wolfe J: Barriers to conducting advance care discussions for children with life-threatening conditions. Pediatrics. 2012; 129:e975–e982
20. Carey EC, Paniagua M, Morrison LJ, et al.: Palliative care competencies and readiness for independent practice: A report on the American Academy of Hospice and Palliative Medicine review of the US medical licensing step examinations. J Pain Symptom Manage. 2018; 56:371–378
21. Brock KE, Cohen HJ, Sourkes BM, et al.: Training pediatric fellows in palliative care: A pilot comparison of simulation training and didactic education. J Palliat Med. 2017; 20:1074–1084
22. Moynihan KM, Jansen M, Siegel BD, et al.: Extracorporeal membrane oxygenation candidacy decisions: An argument for a process-based longitudinal approach. Pediatr Crit Care Med. 2022; 23:e434–e439
23. Opel DJ, Vo HH, Dundas N, et al.: Validation of a process for shared decision-making in pediatrics. Acad Pediatr. 2023; 23:1588–1597
24. October TW, Jones AH, Greenlick Michals H, et al.: Parental conflict, regret, and short-term impact on quality of life in tracheostomy decision-making. Pediatr Crit Care Med. 2020; 21:136–142




留言 (0)