This study investigated the diagnostic performance of visual findings and quantitative parameters of [18F]FDG PET/CT for distinguishing between thymic cysts and low-risk thymoma. PET visual grade and PET central metabolic defect were significant visual findings of [18F]FDG PET/CT, but CT shape was not. PET SUVmax, CT diameter, and CT attenuation in HU were significant quantitative parameters of [18F]FDG PET/CT, with PET SUVmax being the parameter with the highest AUC. Visual and quantitative PET findings of [18F]FDG PET/CT were shown to be useful for diagnosing thymic cysts. As far as we are aware, this study is the first to compare [18F]FDG PET/CT findings between thymic cyst and low-risk thymoma. By distinguishing between thymic cysts and low-risk thymomas, we anticipate reducing unnecessary invasive surgeries for patients with thymic cysts.
Previous studies on [18F]FDG PET/CT showed SUVmax to have better diagnostic utility than morphologic features from CT [20,21,22]. However, these previous studies included all types of TETs as a control (low-risk thymoma, high-risk thymoma, and thymic carcinomas), and demonstrated distinctive PET and CT features among the types [20, 23]. Despite its better diagnostic capability, additional work may be needed to facilitate measurement of SUVmax, whereas in contrast, the PET visual grade can be obtained more easily and conveniently than quantitative PET parameters. The PET visual grade system is also used to evaluate treatment effectiveness in a similar manner to Deauville’s score. The Deauville criteria, a reproducible five-point scale, are widely utilized for interpreting interim PET/CT scans in Hodgkin lymphoma and diffuse large B-cell lymphoma [24]. The two primary reference organs in this criteria system are the liver and the mediastinum. Following the model of these five-point criteria, we adopted a comparable methodology for classifying thymic masses, assessing their metabolic activity in relation to organs like the liver and mediastinum. The majority of thymic cysts in our study showed FDG uptake equal to or lower than that of the mediastinum, resulting in a statistically significant difference in comparison with low-risk thymoma, and a PET visual grade cut-off value of two was adopted.
Although thymic cysts typically show water-like attenuation (HU < 20), atypical protein-rich thymic cysts with solid density may be difficult to differentiate from thymomas featuring low vascularity. Hemorrhage or inflammation within the cyst may result in the formation of cyst fluid that is rich in proteins, which may show soft tissue density on chest imaging studies. In our data, the median and cut-off values for CT attenuation for thymic cysts were 22.3 and 31.3 HU, respectively; values that are higher than the attenuation of pure water (0 HU). In certain cases, discriminating cystic lesions from solid masses using only CT values proves to be challenging. Anterior mediastinal masses judged to require surgical resection may exhibit morphologic features on CT that are closer to those of thymoma than thymic cyst, with observation being the general clinical decision for thymic cyst. If anterior mediastinal masses cannot be distinguished from thymomas on the basis of their morphologic features on CT images and have attenuation higher than 20 HU, additional information may be needed to determine the need for surgery, rather than an invasive biopsy. Cyst components usually exhibit a metabolic defect on [18F]FDG PET/CT [25]. Our study revealed that a visual metabolic defect in an anterior mediastinal mass on PET may indicate a thymic cyst. However, when comparing the diagnostic efficacy of central metabolic defect with SUVmax and the visual grade of PET, the presence of a central metabolic defect appears to have limited value in diagnosing thymic cysts.
Recent studies reported that the median SUVmax of thymic cysts was lower than that of thymomas in surgically-resected thymic abnormalities, and that SUVmax demonstrated comparable diagnostic performance to the morphological features observed on CT [22, 23]. In our study, the median SUVmax was significantly lower in thymic cysts that in low-risk thymomas (0.6 vs. 3.3, P < 0.001). Comparisons of the ROC curves of our [18F]FDG PET/CT-based findings demonstrated that SUVmax was more effective for diagnosing thymic cysts than CT diameter and CT HU measurement. Upon reviewing discordant cases between PET SUVmax and CT diameter, we found that all four patients with PET SUVmax equal to or less than 2.1 (suggesting thymic cysts) and CT diameter greater than 3.3 cm (indicating low-risk thymomas) were diagnosed with thymic cysts. Additionally, among nine patients with PET SUVmax greater than 2.1 (suggesting low-risk thymomas) and CT diameter equal to or less than 3.3 cm (indicating thymic cysts), the final diagnoses were all low-risk thymomas.
For small thymic cysts, observation without surgical resection is recommended unless there is evidence of growth or a very large cystic mass. Conversely, when a thymic lesion is definitively diagnosed as thymoma, early surgical resection or minimally invasive surgery are strongly advised. The discrimination between thymic cysts and thymoma is challenging in small thymic abnormalities. In previous studies, nontherapeutic thymectomy rates varied between 22% and 68% [17, 18], and thymic cysts were the most frequent diagnoses in nontherapeutic thymectomies [18]. Because of pseudo-enhancement caused by their proximity to the thoracic aorta and sternum, thymic cysts can be incorrectly diagnosed as small thymoma on CT imaging. Non-invasive thymoma (such as low-risk thymoma) and thymic cyst usually show a well-defined marginal contour and homogenous CT attenuation. In our study, both thymic cysts and low-risk thymomas exhibited a higher frequency of an oval shape on CT images, with no statistically significant difference between them.
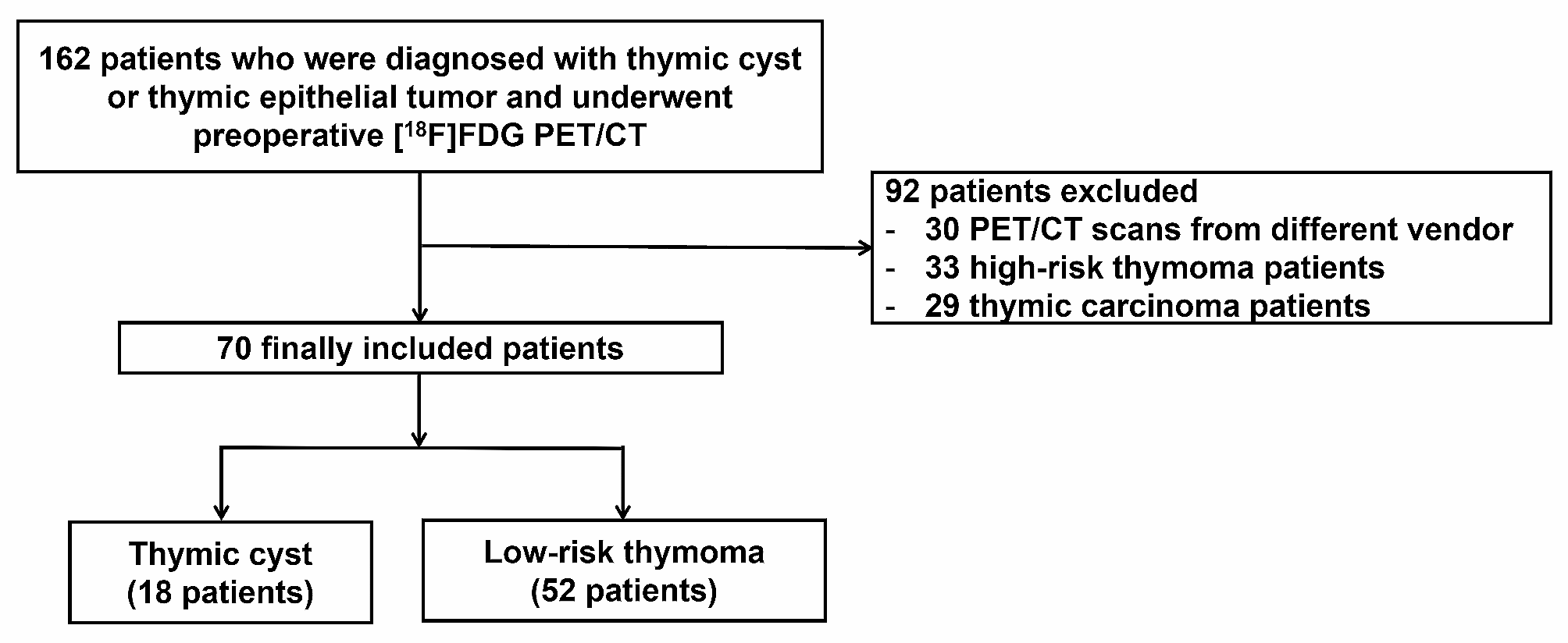
This study has some limitations. As this study was a retrospective single center study, the risk of selection bias exists. Pathology results were unavailable for cases opting for close observation rather than surgery, and therefore only those cases that underwent resection were included in the analysis. In addition, the number of thymic cyst patients was small because thymic cysts are a rare disease and thymic lesions do not commonly undergo preoperative [18F]FDG PET/CT. It is necessary to perform further studies with larger populations and multicentre prospective designs to provide robust confirmation of our findings.







留言 (0)