
記住我

Scleral buckling (SB) continues to play an important role in the treatment of rhegmatogenous retinal detachment (RRD), especially for young patients and certain types of RRD.1,2 Reports have demonstrated that SB is not inferior to pars plana vitrectomy in the repair of RRD in selected cases.1–4 However, more surgeons prefer pars plana vitrectomy because of the advancement in instrumentation and direct intraoperative visualization. Therefore, some surgeons may have limited opportunities to be exposed to training in SB.5 The complications of SB are another obstacle to surgeons' final decision to use SB on their RRD patients. The main side effects of SB include choroidal hemorrhage when having external subretinal fluid drainage, refractive changes caused by the tightened implants, and subsequent implant extrusion.6–9 To decrease the incidence of complications and surgical difficulty, some modifications have been made in recent years, such as the use of absorbable sutures to tighten bands and wide-angle systems to check retinal breaks and ridges formed by the implants.10,11
However, there are few reports with detailed descriptions of how to have releasable SB with absorbable sutures based on conventional surgical steps. The current article introduces a modified SB technique using a combination of nonabsorbable and absorbable sutures to fix and tighten silicone elements to produce a temporary buckling effect for noncomplex RRD and to investigate the tendency of refractive changes caused by this technique.
Materials and MethodsThe study was approved by the Institutional Review Board of Zhongshan Ophthalmic Center of Sun Yat-sen University (Guangzhou, China) and performed in accordance with the World Medical Association's Declaration of Helsinki. Inclusion criteria of noncomplex RRD include without significant proliferative vitreoretinopathy, fresh RRD with a single break, and/or multiple breaks in a single plane. Exclusion criteria include with significant lens opacification, with PVR ≥ C1, those who decided to accept pars plana vitrectomy as the first option to have RRD repair, and the presence of subretinal bands or membranes that had caused shortening of the retina. All the surgeries were performed by one experienced surgeon (Z.Z.). Age, sex, best-corrected visual acuity (BCVA), intraocular pressure, axial length (AL), spherical diopter (SD), and cylinder diopter (CD) were collected in each patient. Snellen visual acuity was transformed into a logarithm of the minimal angle of resolution score for statistical analysis.
Surgical TechniqueAfter routine procedures of conjunctival peritomy and rectus muscle isolation, corneal paracentesis was performed to soften the eye for retinal break detection. Subretinal fluid drainage was not performed in any of the cases (Lincoff technique). Retinal break detection and cryotherapy were visualized with an indirect ophthalmoscope. A segmental silicone tire (#276) was used to form the ridge. If judged necessary based on the numbers and locations of peripheral retinal pathology, an encircling band (#240) was added.
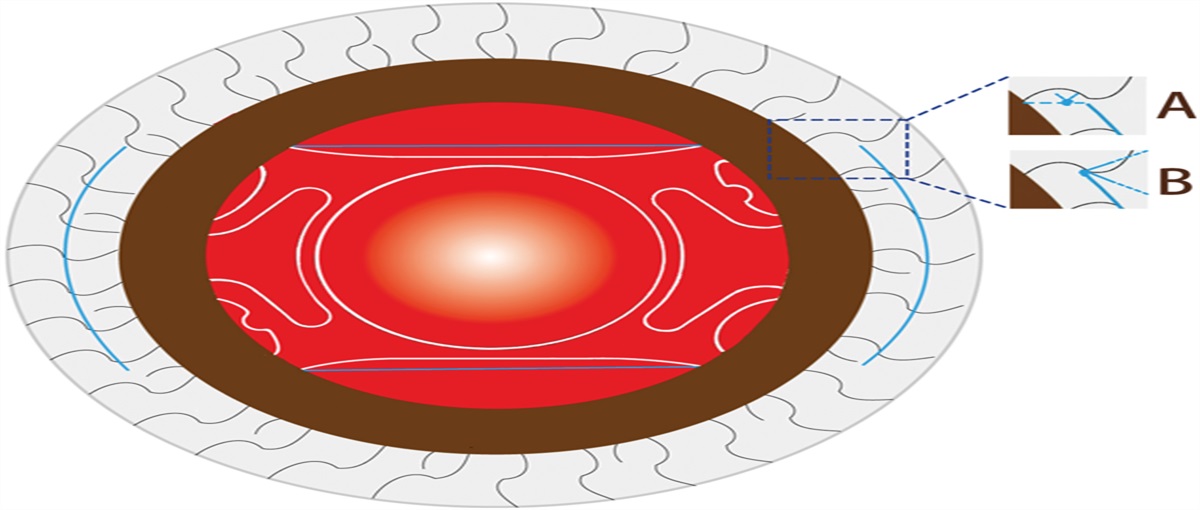
After cryotherapy, the segmental silicone tire was first fixed on the sclera with a 5-0 nonabsorbable suture. The suture passed through the middle of the tire, then the lamellar sclera horizontally, and was subsequently tightened with a square knot on the eyeball surface without any tightening effect on the sclera (Figure 1A). The tire was subsequently tightened to form a ridge with 6-0 absorbable sutures with a 9-mm needle span (Figure 1B). After the ridge formed by the tire was enough to support the break, two ends of the tire were fixed on the eyeball surface with 5-0 nonabsorbable sutures (Figure 1, C and D).
 Fig. 1.:
Fig. 1.: Key steps of the technique using a combination of nonabsorbable and absorbable sutures to produce a temporary buckling effect. A. The segmental silicone tire was fixed on the sclera with 5-0 nonabsorbable suture (green arrow). B. After the knot by 5-0 nonabsorbable suture was performed (green arrow), 6-0 absorbable sutures were added to tighten the silicone tire to form scleral ridge (white arrow). C. One end of the silicone tire was fixed on the sclera with 5-0 nonabsorbable suture (green arrow). D. Another end of the silicone tire was fixed on the sclera with 5-0 nonabsorbable suture (green arrow). E. Using a silicone sleeve (green arrow) to hold two ends of the encircling band and then tighten two ends of the band with 6-0 absorbable suture. F. With a knot by 5-0 nonabsorbable suture to keep the band in place (green arrow), the silicone sleeve had been removed, and the knot by 6-0 absorbable suture was the only factor tightening up two ends of the band.
When the encircling band was added, the band was sutured together with the tire and fixed on the sclera with 5-0 nonabsorbable sutures (Figure 1A). The 6-0 absorbable sutures were then used to tighten the segmental silicone tire and form the ridge. The 5-0 nonabsorbable sutures were added in other quadrants for permanent immobilization of the encircling band. As a routine, a silicone sleeve was used to link two ends of the encircling band and tighten up the band. A nonabsorbable suture was added to fix the band on the sclera to prevent vertical sliding. Subsequently, the 6-0 absorbable suture was used to tie up two ends of the band (Figure 1E). Finally, the silicone sleeve was cutoff (Figure 1F).
The principle for the above suturing technique was permanent immobilization of the silicone elements with 5-0 nonabsorbable sutures and tightening of them to form a temporary ridge with 6-0 absorbable sutures (see Video, Supplemental Digital Content 1, https://links.lww.com/IAE/C159, which demonstrates the modified technique).
Finally, optic disk perfusion was checked with an indirect ophthalmoscope, and corneal paracentesis was performed if necessary. One week and till the final follow-ups after the surgery, retinal laser photocoagulation was performed to further seal the break and other degenerative areas when judged necessary by the surgeon. Indications for postoperative retinal laser photocoagulation included the primary break was found not adequately sealed by cryotherapy; missed degenerative areas found after surgery; and newly occurred degenerative areas found during the follow-ups.
Results General Characteristics and Surgical OutcomesTwenty consecutive patients were prospectively included in this study, including four women (20.0%) and 16 men (80%), with a mean age of 20.0 ± 7.9 (range, 9–38) years. All patients achieved primary retinal reattachment. The mean preoperative BCVA (logarithm of the minimal angle of resolution) was 0.75 ± 0.44 (Snellen range, 20/1,000–20/20), which showed significant improvement to 0.32 ± 0.35 at the 1-month follow-up (P < 0.001). The mean BCVA (logarithm of the minimal angle of resolution) at the 3-month follow-up was 0.21 ± 0.35, exhibiting a significant improvement when compared with the 1-month follow-up (P < 0.05). At the final follow-up, the mean BCVA (logarithm of the minimal angle of resolution) was 0.18 ± 0.30, which had no significant difference with the 3-month follow-up (P = 0.23).
The ridge was well present and in situ in each patient at the 1-month follow-up but disappeared at the 3-month follow-up. Postoperative laser photocoagulation was performed in four patients (20%). Except for transient intraocular pressure elevation after the surgery, no obvious intraoperative and postoperative complications were observed.
Axial Length and Refractive ChangesThe AL before surgery was 24.78 ± 2.14 (range, 21.69–30.01) mm, which significantly increased to 25.22 mm ± 2.11 mm at the 1-month follow-up (P < 0.001). At the 3-month follow-up, the AL decreased significantly to 24.80 mm ± 2.14 mm compared with the 1-month follow-up (P < 0.001). The AL at the final follow-up was 24.83 mm ± 2.13 mm.
The mean SD before surgery was 0.06 ± 3.33 (range, −7.75 to 6.50). At the 1-month follow-up, the mean SD was −4.36 ± 3.20 (range, −10.25 to 0.75). The mean SD at the 3-month and final follow-ups was −3.25 ± 3.18 (range, −9.5 to 1.50) and −3.49 ± 3.19 (range, −9.5 to 1.50), with the difference having statistical significance (P < 0.05).
The mean CD before surgery was −1.99 ± 1.03 (range, −4.5 to 0.25), which significantly increased to −2.95 ± 1.55 at the 1-month follow-up (P < 0.001). At the 3-month follow-up, the CD decreased to −1.98 ± 1.03 (P < 0.001) when compared with the 1-month follow-up. The mean CD at the final follow-up was −1.94 ± 1.07, which had no significant difference preoperatively or at the 3-month follow-up (P = 0.64). The overall preoperative and postoperative AL and refractive data of the patients were listed in Table 1.
Table 1. - Overall Preoperative and Postoperative AL and Refractive Data of the Patients (n = 20) Patient No. Age, Year Sex EB (+/–) AL, mm SD CD Pre- 1 Month 3 Months Final Pre- 1 Month 3 Months Final Pre- 1 Month 3 Months Final 1 14 M – 24.30 24.44 24.33 24.36 −0.75 −2.50 −2.25 −2.75 −1.25 −2.00 −1.00 −1.50 2 20 M + 24.30 25.10 24.32 24.33 −1.75 −4.25 −2.50 −3.25 −4.50 −6.00 −4.50 −4.75 3 19 M – 24.44 24.90 24.49 24.50 0.50 −1.75 −1.75 −2.00 −2.50 −2.25 −2.00 −2.25 4 15 M – 26.01 26.08 26.05 26.03 −1.50 −6.50 −6.00 −6.25 −1.75 −2.25 −1.50 −1.50 5 21 F + 26.07 26.74 26.10 26.15 −3.75 −8.50 −6.25 −6.75 −2.25 −5.00 −2.25 −2.00 6 31 M + 30.01 30.99 30.03 30.01 −1.00 −5.50 −3.00 −3.25 −2.00 −5.00 −2.00 −2.25 7 9 M + 23.56 23.94 23.58 23.63 6.50 −1.25 −0.25 −0.50 −0.75 −2.25 −1.00 −0.75 8 26 M – 28.09 28.25 28.08 28.11 −3.00 −7.50 −7.75 −8.25 −2.75 −2.50 −2.50 −2.50 9 18 M – 25.80 25.77 25.84 25.88 −4.75 −6.25 −5.75 −5.75 −2.25 −2.50 −2.25 −2.00 10 32 M – 26.55 26.69 26.59 26.61 −7.75 −9.00 −8.25 −8.25 −0.25 −0.75 −0.75 −0.50 11 15 M + 23.17 23.85 23.20 23.19 2.25 −5.00 −2.50 −2.50 −1.75 −4.25 −2.00 −1.75 12 14 M + 22.50 23.21 22.52 22.60 1.75 −1.75 −0.50 −0.50 −3.00 −4.25 −2.75 −2.75 13 13 M + 23.58 24.22 23.65 23.70 2.75 −1.25 −0.50 −0.50 −0.75 −1.25 −0.50 −0.25 14 15 M + 22.85 23.12 22.86 22.90 3.25 −2.25 −0.50 −0.50 −3.75 −4.75 −4.00 −3.75 15 25 F – 27.94 27.89 27.91 27.97 2.75 −10.25 −9.50 −9.50 −2.50 −2.00 −2.75 −2.75 16 11 M + 24.01 24.75 24.00 24.10 −0.50 −4.75 −3.50 −3.50 −1.00 −3.50 −0.75 −1.00 17 17 F + 24.59 25.20 24.62 24.65 2.00 −7.75 −5.50 −6.00 −1.75 −3.50 −2.00 −2.00 18 17 M – 21.69 22.00 21.67 21.70 2.25 0.75 1.00 0.00 −2.25 −0.50 −2.25 −2.00 19 9 M + 22.50 23.33 22.50 22.55 3.25 −0.75 1.50 1.50 −1.50 −3.25 −1.25 −1.25 20 38 F – 23.70 23.85 23.74 23.71 −1.25 −1.25 −1.25 −1.25 −1.25 −1.25 −1.50 −1.25 Mean 20.0 24.78 25.22* 24.80*,† 24.83*,† 0.06 −4.36* −3.25*,† −3.49*,† −1.99 −2.95‡ −1.98§ −1.94§*Having statistically significant difference with the mean before surgery (P < 0.001).
†Having statistically significant difference with the mean at 1-month postoperatively (P < 0.001).
‡Having statistically significant difference with the mean before surgery (P < 0.05).
§Having statistically significant difference with the mean at 1-month postoperatively (P < 0.05).
F, female; M, male; 1 month, postoperative 1 month; 3 months, postoperative 3 months; Pre-, preoperative.
A total of 11 patients (55%) underwent encircling and segmental SB (encircling buckling [EB] group), whereas nine patients (45%) underwent only segmental SB (SB group). The two had no significant differences in baseline characteristics, including age, sex, preoperative BCVA, AL, SD, and CD (all P > 0.05).
At the 1-month follow-up, the mean AL elongation in the EB group was significantly larger than that in the SB group (0.66 ± 0.20 mm vs. 0.15 ± 0.16 mm; P < 0.001). However, the AL elongation in both groups showed no significant difference at the 3-month and the final follow-ups. At the 3-month follow-ups, a significantly greater decrease of SD was noted in the EB group compared with the SB group (1.77 ± 0.63 vs. 0.31 ± 0.35).
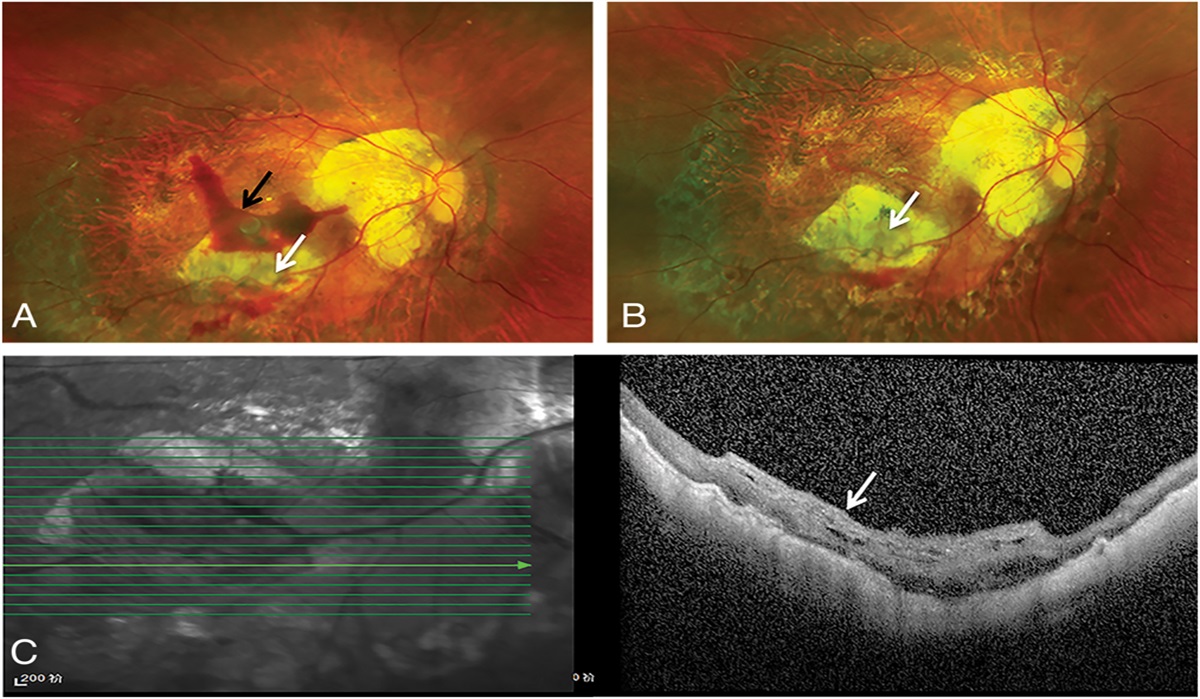
More obvious changes in CD were noted in the EB group during the follow-ups. At the 1-month follow-up, the CD in the EB group showed a significant increase compared with that before surgery (−3.90 ± 1.35 vs. −2.09 ± 1.22; P < 0.001). However, it decreased and became equal to the preoperative one at the 3-month and the final follow-ups (both P > 0.05). In the SB group, no significant change in CD was observed during all the follow-ups (P > 0.05). Two typical cases at different stages are demonstrated in Figures 2 and 3. The detailed refractive changes of the two groups were illustrated in a Supplemental Digital Content 2 (see Table, https://links.lww.com/IAE/C160).
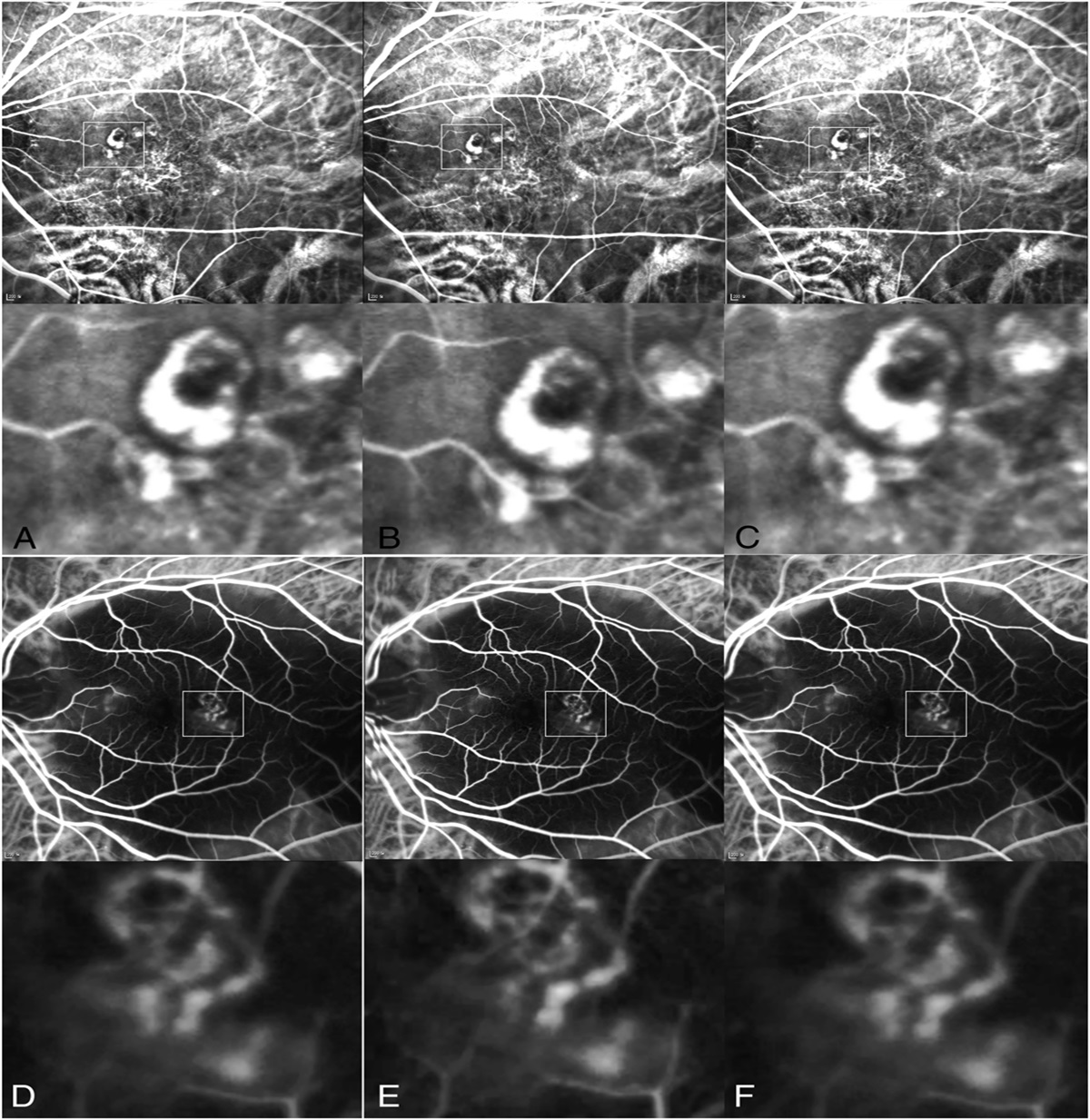
 Fig. 2.:
Fig. 2.: Typical case who underwent the suturing technique with both segmental silicone tire and encircling band. A. Before surgery, a retinal tear (white arrow) and superficial macula-off retinal detachment were observed. B. One day after the surgery, retinal reattached, with an obvious scleral ridge. C. One month after surgery, the ridge was still present and in situ. D. Three months after surgery, the SB effect diminished, and the retina remained reattached.
 Fig. 3.:
Fig. 3.: Typical case who underwent the suturing technique with only segmental silicone tire. A. Before surgery, a small round retinal hole (red arrow) and superficial macula-on retinal detachment were observed. B. One day after the surgery, retinal reattached, with an obvious scleral ridge. C. One month after surgery, the ridge was still present and in situ. D. Three months after surgery, the SB effect diminished, and the retina remained reattached.
DiscussionIn the current article, we introduced a modified SB technique using a combination of permanent and absorbable sutures to produce a temporary SB effect to repair noncomplex RRD. The anatomic and functional outcomes were noninferior to previous reports. The buckling effect was effective at 1 month after surgery that then diminished by 3 months. The retina remained reattached during the whole postoperative follow-ups even after the effect diminished. Refractive changes induced by the buckling effect was also found to be temporary, which decreased to nearly the preoperative level at the 3-month follow-up. The scleral ridge formed by the silicone elements disappeared at the 3-month follow-up, suggesting that all the knots formed by the absorbable sutures lost their tension after the surgery, consistent with previous reports that used absorbable sutures.
One of the concerns with SB is that it would elongate the AL. Smiddy et al7 showed that EB caused an increased AL of 0.99 mm. Wong et al8 also showed an average AL increase of 0.20 mm and 0.42 mm at 1 month and 12 months after SB, respectively. In our study, the AL had an average increase of 0.44 mm 1 month after surgery. Meanwhile, at the 3-month follow-up, the AL had remarkably decreased to be almost equal to the preoperative level. This result could be explained by the fact that the 6-0 absorbable sutures had lost the force to form the ridge that would otherwise elongate the eyeball. At the final follow-up, the AL slightly increased to 24.83 mm ± 2.13 mm from the baseline of 24.78 mm ± 2.14 mm. This might be attributed to the continuing eye growth on the part of the patients because the average age of the patients was only 20 years.12
Consistent with the changes of AL, our study showed a pike of spherical refractive error to −4.36 diopter (D) ± 3.20 D at the 1-month follow-up. The average value of spherical refractive error before surgery was not selected as a reliable control with the ones after surgery because of the detached retina, especially when the macula is involved (macula-off), will cause a false hyperopic shift in the eyes.
The mean SD decreased significantly to −3.25 ± 3.18 and −3.49 ± 3.19 at the 3-month and final follow-up, respectively. It could be believed that the myopic shift caused by SB partly disappeared at the 3-month follow-up because the ridge had also disappeared concomitantly. A mild increase in SD at the final follow-up could also be attributed to eye growth on the part of the patients. An identical change of astigmatism as myopia was also observed in the current study. The cylinder refractive error reached a pike of −2.95 D ± 1.55 D at the 1-month follow-up and decreased to be almost equal to the preoperative one at the 3-month and final follow-ups.
Patients who underwent segmental SB with an additional encircling band (EB group) experienced more remarkable AL elongation 1 month postoperatively compared with those who merely underwent segmental scleral bucking (SB group). This result suggests that EB had a greater effect on inducing AL elongation than segmental buckling. Furthermore, patients in the EB group had a significant increase in astigmatic refractive error at the 1-month follow-up. However, those in the SB group showed no significant change of astigmatic refractive error all through the follow-ups. This result might be attributed to the small sample size of the SB group.
The current study has several limitations. It was not a randomized controlled trial. The sample size was not large enough to show more obvious and accurate changes in AL and refractive errors. The anterior-chamber depth was not included as a parameter. Further studies with larger sample size and longer follow-ups were anticipated to have more in-depth investigation of the technique.
In conclusion, the modified suture technique is safe and effective in treating RRD in selected patients. The technique has minimal effect in inducing long-term AL and refractive status in patients who underwent SB with/out an encircling band. The modified technique may be an ideal option, especially for selected patients with hypermyopia and antimetropia.
References 1. Shu I, Ishikawa H, Nishikawa H, et al. Scleral buckling versus vitrectomy for young Japanese patients with rhegmatogenous retinal detachment in the era of microincision surgery: real-world evidence from a multicentre study in Japan. Acta Ophthalmol 2019;97:e736–e741. 2. Adelman RA, Parnes AJ, Ducournau D, European Vitreo-Retinal Society EVRS Retinal Detachment Study Group. Strategy for the management of uncomplicated retinal detachments: the European vitreo-retinal society retinal detachment study report 1. Ophthalmology 2013;120:1804–1808. 3. Znaor L, Medic A, Binder S, et al. Pars plana vitrectomy versus scleral buckling for repairing simple rhegmatogenous retinal detachments. Cochrane Database Syst Rev 2019;3:CD009562. 4. Koto T, Kawasaki R, Yamakiri K, et al. Six months primary success rate for retinal detachment between vitrectomy and scleral buckling. Retina 2021;41:1164–1173. 5. Adams OE, Culican SM. The dangerous decline in teaching scleral buckling procedures. Clin Exp Ophthalmol 2023;51:511–513. 6. Papakostas TD, Vavvas D. Postoperative complications of scleral buckling. Semin Ophthalmol 2018;33:70–74. 7. Smiddy WE, Loupe DN, Michels RG, et al. Refractive changes after scleral buckling surgery. Arch Ophthalmol 1989;107:1469–1471. 8. Wong CW, Ang M, Tsai A, et al. A prospective study of biometric stability after scleral buckling surgery. Am J Ophthalmol 2016;165:47–53. 9. Cetin E, Ozbek Z, Saatci AO, Durak I. The effect of scleral buckling surgery on corneal astigmatism, corneal thickness, and anterior chamber depth. J Refract Surg 2006;22:494–499. 10. Savastano A, Weinberg T, Faraldi F, et al. Scleral buckling using chandelier and releasable suture: a useful surgical variant. Retina 2023;43:363–366. 11. Sotani Y, Imai H, Iwane Y, et al. Intraoperative optical coherence tomography for real-time visualization of the positional relationship between buckling material and retinal breaks during scleral buckling for rhegmatogenous retinal detachment. Retina 2022;42:2395–2400. 12. Sato T, Kawasaki T, Okuyama M, Ideta H. Refractive changes following scleral buckling surgery in juvenile retinal detachment. Retina 2003;23:629–635.
留言 (0)