BACKGROUND:
Grade II and III hemorrhoids often require a multimodal approach that may ultimately culminate in surgical resection. Age and overall medical conditioning around the time of diagnosis can often impact the decision.
OBJECTIVE:
The objective of this study was to evaluate patients with a diagnosis of symptomatic grade II or grade III hemorrhoids and determine progression to hemorrhoidectomy based on age and the time interval between diagnosis and surgical intervention.
DESIGN:
A retrospective cohort study.
SETTINGS:
Group practice at a single institution.
PATIENTS:
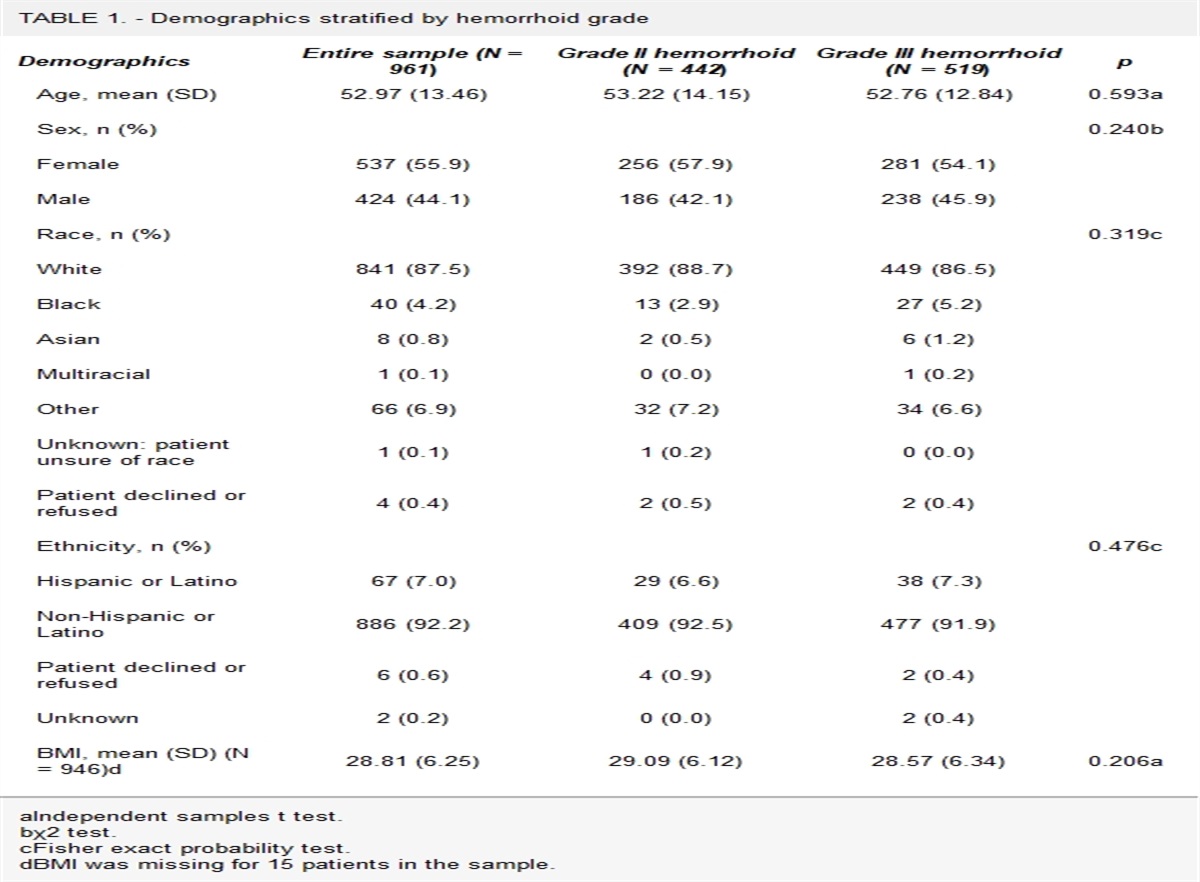
Patients aged 18 to 75 years with grade II or grade III internal hemorrhoids between 2015 and 2020 were included. Patients with thrombosed hemorrhoids or surgical contraindications to hemorrhoidectomy were excluded. A total of 961 patients met inclusion criteria for grade II (n = 442) and III (n = 519) hemorrhoids.
INTERVENTION:
Treatments included hemorrhoidectomy, in-office procedures, and/or medical management.
MAIN OUTCOME MEASURES:
Baseline demographics, treatment choices, and time to hemorrhoidectomy (if applicable) were stratified and analyzed on the basis of hemorrhoid grade (grade II and III) and age groupings that were predetermined by the authors (18–30, 31–50, and 51–75 years).
RESULTS:
Patients with grade III versus grade II hemorrhoids were more likely to choose hemorrhoidectomy as the initial treatment management (27.6% vs 4.1%). Patients in the age groups of 18 to 30 and 30 to 50 years were more likely to choose hemorrhoidectomy as the initial treatment management compared to those in the age group of 51 to 75 years (23.5% and 22% vs 12.8%). In patients who were initially treated with medical management or office-based procedures and then progressed to hemorrhoidectomy, no significant differences in the length of time to hemorrhoidectomy were noted on the basis of hemorrhoid grade or age.
LIMITATIONS:
Data only looked at age groups and their treatment selection. Personal biases of surgeon and patient may alter results.
CONCLUSIONS:
Our study shows that the younger population tends to seek hemorrhoidectomy first over the older population. See Video Abstract.
HEMORROIDECTOMÍA: ¿LA EDAD MARCA LA DIFERENCIA?
ANTECEDENTES:
Las hemorroides de grado II y III a menudo requieren un abordaje multimodal que en última instancia puede culminar en una resección quirúrgica. La edad y el estado médico general en el momento del diagnóstico a menudo pueden afectar la decisión.
OBJETIVO:
El objetivo de este estudio fue evaluar a pacientes con diagnóstico de hemorroides sintomáticas grado II o grado III y determinar la progresión a hemorroidectomía en función de la edad y el intervalo de tiempo entre el diagnóstico y la intervención quirúrgica.
DISEÑO:
Estudio de cohorte retrospectivo.
ESCENARIO:
Práctica grupal en una sola institución.
PACIENTES:
Se incluyó a pacientes de 18 a 75 años con hemorroides internas de grado II o III entre 2015 y 2020. Se excluyeron los pacientes con hemorroides trombosadas o contraindicaciones quirúrgicas para hemorroidectomía. Un total de 961 pacientes cumplieron los criterios de inclusión para hemorroides de Grado II (n=442) y III (n=519).
INTERVENCIÓN:
Los tratamientos incluyeron hemorroidectomía, procedimientos en el consultorio y/o manejo médico.
PRINCIPALES MEDIDAS DE RESULTADO:
Los datos demográficos iniciales, las opciones de tratamiento y el tiempo hasta la hemorroidectomía (si corresponde) se estratificaron y analizaron según el grado de hemorroides (grado II y III) y los grupos de edad predeterminados por los autores (18-30, 31-50). y 51-75).
RESULTADOS:
Los pacientes con hemorroides de Grado III versus Grado II tuvieron más probabilidades de elegir la hemorroidectomía como tratamiento inicial (27,6% versus 4,1%). Los pacientes de los grupos de edad de 18 a 30 y de 30 a 50 años tenían más probabilidades de elegir la hemorroidectomía como tratamiento inicial en comparación con los de 51 a 75 años (23,5% y 22% frente a 12,8%). En los pacientes que inicialmente fueron tratados con manejo médico o procedimientos en el consultorio y luego progresaron a hemorroidectomía, no se observaron diferencias significativas en el tiempo hasta la hemorroidectomía según el grado o la edad de las hemorroides.
LIMITACIONES:
Los datos solo analizan los grupos de edad y su selección de tratamiento. Los sesgos personales del cirujano y del paciente pueden alterar los resultados.
CONCLUSIÓN:
Nuestro estudio muestra que la población más joven tiende a buscar primero la hemorroidectomía que la población de mayor edad. (Traducción—Dr. Felipe Bellolio)


留言 (0)