
記住我


In this population-based cohort study, we obtained data from the Korean National Health Insurance Service (NHIS) database. Since the implementation of universal health coverage in 1989, all South Korean citizens have been obliged to subscribe to the NHIS, and approximately 98% of the entire population has been enrolled. The NHIS database includes the International Classification of Diseases 10th revision (ICD-10) diagnostic codes, prescriptions for medications, length of hospital stay, medical expenses, and information regarding healthcare provisions [13].
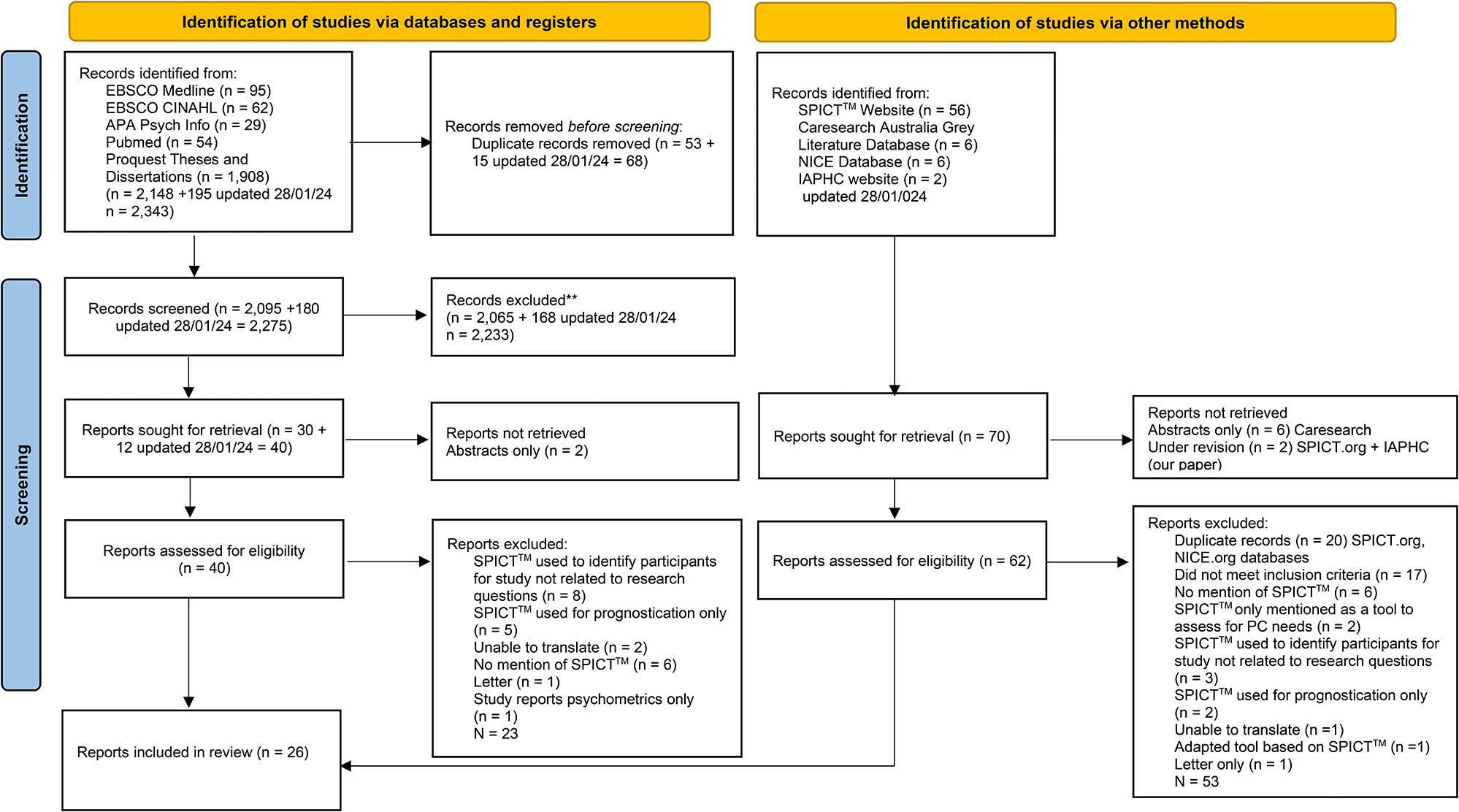
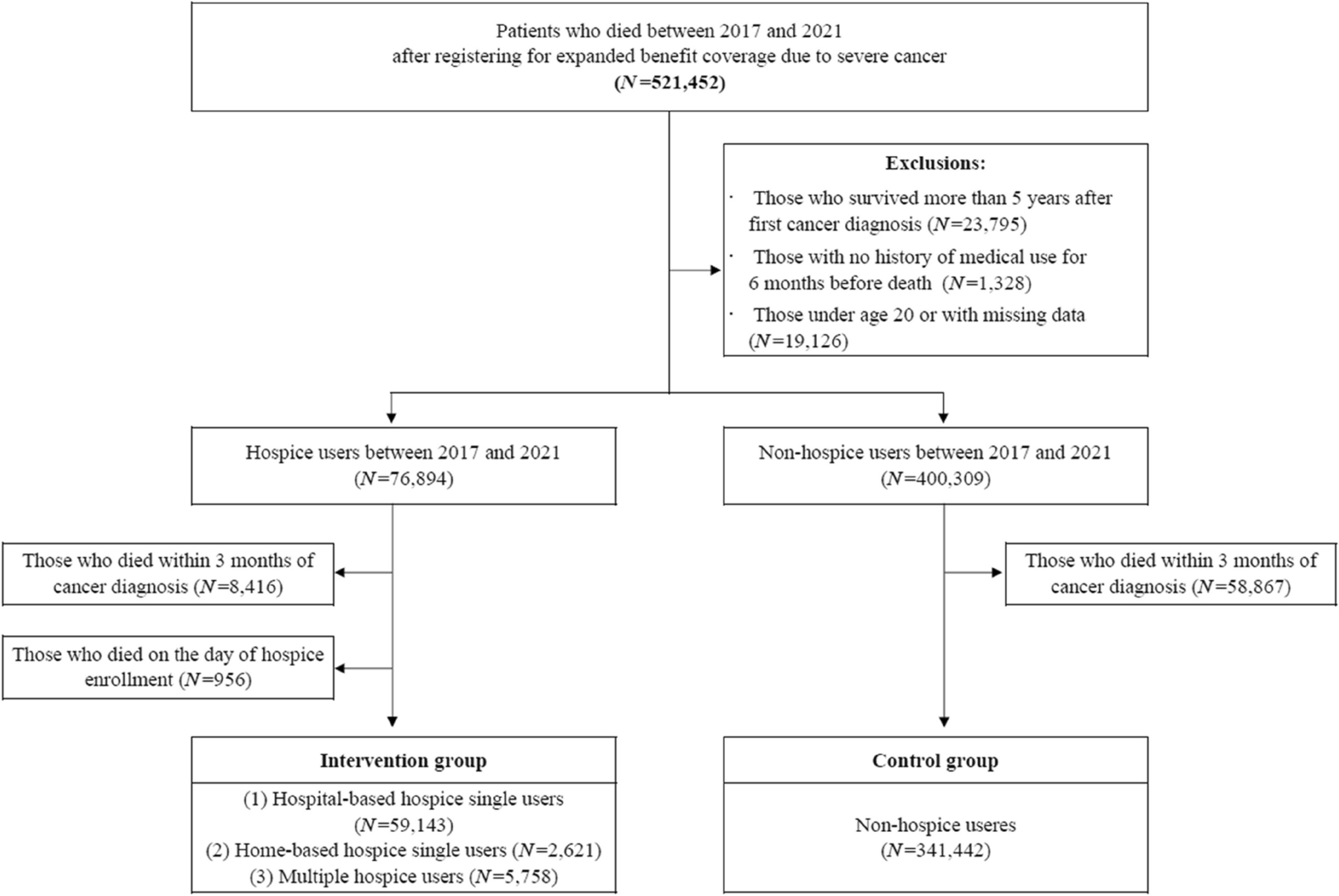
To explore the impact of the type of hospice used on cancer patients’ EoL care patterns, we included cancer patients who died after registering for expanded benefit coverage due to severe cancer (claim code: “V193”). Subsequently, we obtained the NHIS cohort data of all 521,452 registered cancer patients who died between January 1, 2017 and December 31, 2021. We excluded those who survived > 5 years after their first cancer diagnosis, had no medical records for 6 months before death, and aged < 20 years or had missing data were sequentially excluded, resulting in a total of 477,203 participants. Among them, 76,894 individuals had used hospice care within 6 months before death, whereas 400,309 did not. Because we aimed to investigate care patterns and expenditures 1 and 3 months before death based on hospice care use, we excluded patients who died within 3 months of their cancer diagnosis. As determining patients who died on the day of hospice enrollment in the intervention group, we also excluded such patients (n = 956). Finally, 408,964 individuals were eligible for analysis, of which 67,522 and 341,422 individuals were in the intervention and control groups, respectively. A flowchart of the study sample selection process is shown in Fig. 1.
Fig. 1
Flow chart of study population selection
VariablesThe dependent variables were the patterns of care, which were divided into intense and supportive care. Intense care refers to aggressive treatment to prolong the life of cancer patients [14]; in this study, it was specifically defined as intubation and ventilator use, cardiopulmonary resuscitation, hemodialysis, care in the intensive care unit (ICU), or computed tomography (CT) use. Supportive care refers to pain control and psychological relief management that can significantly impact the cancer patients’ QoL [15,16,17,18] and was defined as a prescription of narcotic analgesics and visits to psychiatry and family medicine clinics (Supplementary Table 1). For these outcomes, whether the patient received care in the last 30 and 90 days of life was identified as a binary variable, and the total amount of care was identified as a count variable.
The type of hospice used in the 6 months before death was classified into four categories as follows: those who have (1) never used hospice (reference group); (2) only used hospital-based hospice (claim codes: “WJ-,” “WK-,” “WL-,” “WM-,” “WN-,” “WO-,” “WG-,” “WH-”); (3) only used home-based hospice (claim codes: “AP-”); and (4) used both hospital- and home-based hospice within 6 months before death.
We included 10 variables in the analysis as covariates. First, as sociodemographic factors, sex (males and females), age (range: < 30, 30–39, 40–49, 50–59, 60–69, and ≥ 70 years), region (Seoul and metropolitan cities, small cities, and rural area), income level (low [quintile, 1–6], middle [7–13], high [14–20]) and type of health insurance subscription (regionally-insured, workplace-insured, and Medicaid) were included in the analysis. Second, as factors related health status, we adjusted for the Charlson comorbidity index (CCI) score (range: 0–1 and ≥ 2), primary cancer type (lung, liver, colorectal, gastric, pancreatic, gallbladder/bile duct, breast, and prostate cancer, non-Hodgkin's lymphoma, leukemia, and other types), survival time after cancer diagnosis (90–365 days, 366–730 days, 731–1,095 days, and ≥ 1,096 days), and the year of death.
Statistical analysisWe used the chi-squared test to examine the distribution of general characteristics of the study population in the year of death. General characteristics are presented as frequencies (n) and percentages (%), whereas descriptive statistics for all dependent variables are reported as means and standard deviations. To identify differences in care patterns between hospice types, a generalized linear model with a zero-inflated negative binomial (ZINB) distribution was applied. Count data containing a large number of zeros are commonly observed across various fields, such as medicine and public health [19, 20]. Zero inflation, which often signifies overdispersion, indicates that the frequency of zero counts exceeds expectations. When the overdispersion in raw data is due to zero inflation, the zero-inflated Poisson (ZIP) model serves as a standard framework for fitting the data [21]. After factoring in zero inflation and if the data persistently indicate further overdispersion, the ZINB model should be considered [22]. This model combines a distribution degenerate at zero with a baseline negative binomial distribution as an alternative to the ZIP model [23, 24]. As a result, the ZINB model had two components [25, 26]: First, we estimated the odds ratios (OR) from a logistic regression model (zero component). Second, we estimated the risk ratio (RR) using the results of the negative binomial regression model (count component). In this study, the zero component was modeled to estimate the probability that an excess zero will not occur, that is, a non-zero probability.
All statistical analyses were conducted using the SAS version 9.4 software (SAS Institute Inc., Cary, NC, USA). Statistical significance was set at p < 0.05.
留言 (0)