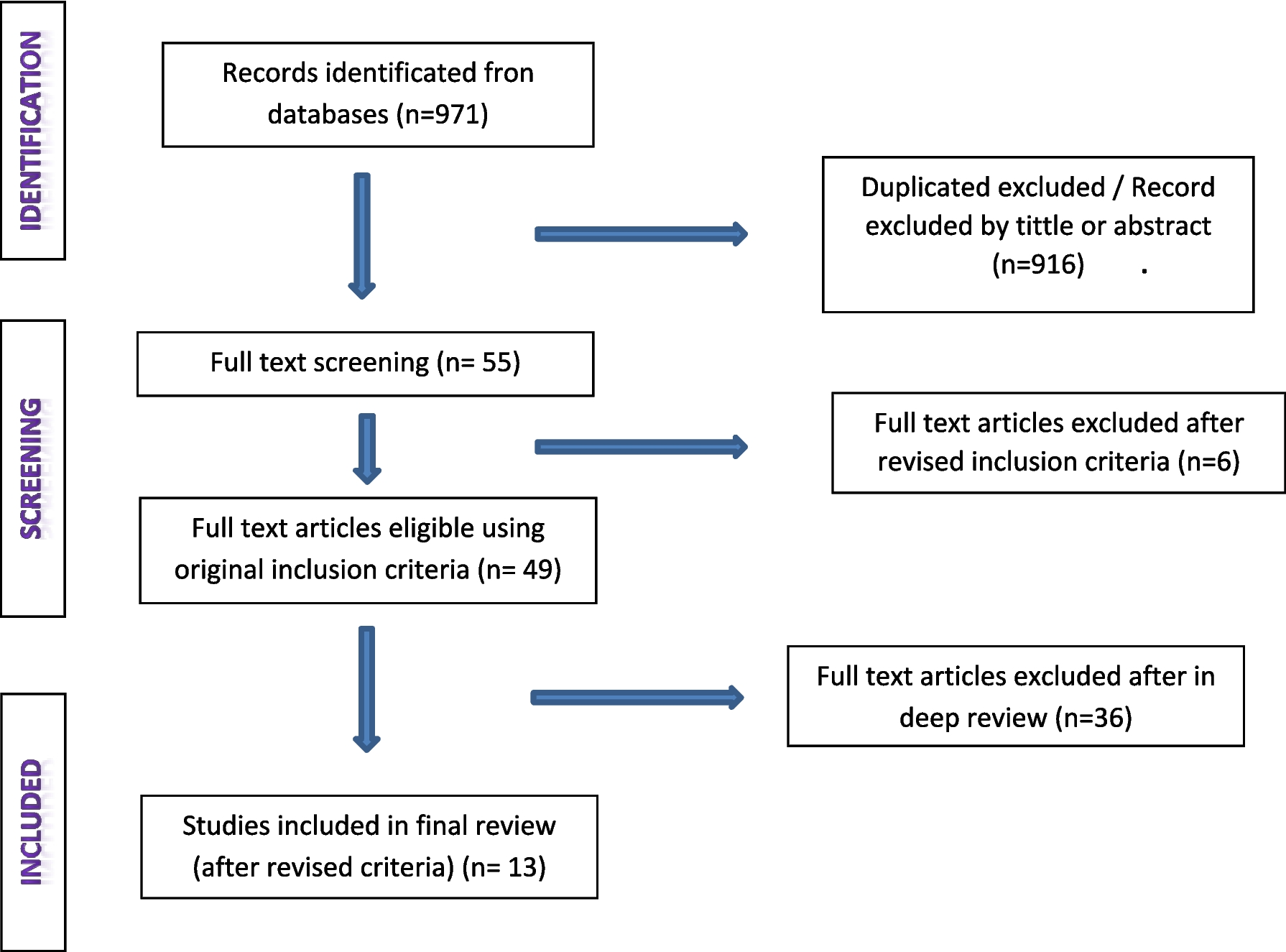
We have aimed to create the Clinical Practice Guideline (CPG) for the management of Palliative patients using the GRADE-ADOLOPMENT process, sourced from the “NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Palliative Care, Version 2.2021” as of December 2, 2020 [7] . Best evidence review, and expert panel input were maximized to develop the CPG and subsequent referral pathways suitable for Pakistan. From the source guidelines, we adopted all the recommendations, except for 15 which were due to repetition and reference to oncological assessment.
WHO recognizes access to palliative care as a fundamental human right [30] . Considering the escalating burden of non-communicable diseases, the need for palliative care cannot be understated anymore. WHO defines palliative care as “specialized medical care for people living with serious illness” which is incurable and/or life-threatening with drastic changes to a patient’s quality of life [31, 32] . Worldwide, a mere 14% of the population who requires palliative care is able to receive it, with most of this care concentrated in high-income countries (HICs) [33]. Concurrently, an estimated 56.8 million people are in need of this service, with the majority residing in low- and middle-income countries (LMICs) which are consequently faced with inadequate access and a high unmet need [33] . As such, it was imperative that LMICs such as Pakistan develop CPGs to implement palliative care holistically within health systems and improve access. Currently, the vast majority of CPGs that form the foundation of palliative care and are recognized have been developed by high-income Western countries. This is primarily due to their well-established practices and existing research infrastructure in palliative care. In a survey conducted by WHO, it was revealed that only 68% of countries had funding available for palliative care, however, the services were reported to reach only half the patients in need in only 40% of the countries [34] . LMICs, including Pakistan, face challenges in terms of financial resources, research capacity, and expertise, which hinder the development of local guidelines that would cater to their unique needs.
Moreover, several studies have shown a preference for at-home care or community-based care of serious patients who require palliative interventions [35] . Most people in the developed world die in an acute care setting, if not at a hospice, which contrasts with the wishes of the patients [36] . Despite the lack of adequate data, it is reasonable to assume that in a country like Pakistan, where the majority of hospital costs are through out-of-pocket financing, there is increased hesitance for inpatient hospital care in serious patients and poorly developed care options in the community which inevitably creates gaps in the continuum of care. Pakistan has a significant influence of culture and religion in our society which also requires our local CPGs to be tailored according to its principles [18] . As such, a shift to primary care pathways is paramount in improving access to quality palliative care, and cost-effectiveness but also is in line with patient preferences for community care. Therefore, the introduction of an integrated clinical guideline such as that we have proposed serves as a system-oriented strategy to enhance patient access to essential treatment, provide relief, and address the existing gap in the provision of care [37] . Thus, we utilized the GRADE-ADOLOPMENT approach to develop a CPG that incorporate the best available evidence and address the specific needs of the local context to improve Pakistan's palliative healthcare system. Not only will this guideline of care provide an objective, algorithmic approach to palliative care within general practitioners, it takes into account the socio-demographic factors of a low-resource region like Pakistan leading to the shift of specialized palliative care treatment towards primary care. [38].
Our CPG for palliative care recommends developing a plan of care that involves an interprofessional team comprising physicians, advanced practice clinicians, nurses, mental health professionals, social workers, chaplains, and other healthcare professionals. A collaborative approach aims to effectively meet the diverse requirements of patients in palliative care [39, 40] . Furthermore, the guidelines also recommend the incorporation of palliative care within general oncology care. This approach intends to improve the quality of life and ultimate survival of patients with cancer [41, 42] . Moreover, symptom and condition-specific sections in our CPG have been developed. They provide information on recommended agents, dosage adjustments based on estimated life expectancy and symptom etiology, route of administration, as well as radiography and surgical indications. Our guidelines recommend a thorough documentation of patient decisions, discussions, and agreements in the medical record. The documentation includes the use of tools such as “POLST (Physician Orders for Life-Sustaining Treatment)” or “MOLST (Medical Orders for Life-Sustaining Treatment)” to safeguard patient autonomy and guide clinical decision-making aligning with any of the patient's expressed preferences. Furthermore, the CPG also addresses mental health considerations, such as persistent complex bereavement disorder. This condition is characterized by a chronically intensified state of mourning which significantly impairs functioning, therefore, our CPG include recommendations on managing and addressing mental health challenges associated with this disorder, for holistic care. Oncology assessments and repeated recommendations were intentionally excluded from the GRADE-ADOLOPMENT process to prevent redundancy and improve clarity of the CPG.
In addition to the CPG, our team created primary care referral pathways in collaboration with local experts. These are essential as they provide a comprehensive outline for managing particular clinical conditions and aim to incorporate the most up-to-date evidence in a systematic manner [31, 43] . Such protocols reduce inter-practitioner variability of practices and improve outcomes, with reduced costs [37, 44] . The creation of algorithms, including the “Liverpool Care Pathway (LCP)” has resulted in widespread adoption and implementation of pathways in HICs such as the United States, China and Australia, showing their importance [45,46,47] . Similar to existing integrated care pathways, we developed primary care referral pathways in collaboration with local experts following the review and consensus on our final CPG. These pathways provide a direct link to the CPG and are an extrapolation of the existing guidelines for ease of understanding of general practitioners and improving access to palliative medicine at the level of primary care. They are user-friendly and optimized to be considerably simple and uncomplicated to comprehend for all practitioners. These pathways are objective algorithms of care for treatment decisions with the aim of improving patient outcomes in countries with low resources such as Pakistan [31, 48, 49].
We faced several challenges in the development of our CPG. With no prior existing infrastructure in palliative medicine in Pakistan outside of newly introduced services in tertiary care centers, it was difficult to establish a comprehensive care pathway which employed a multidisciplinary approach. Limited literature was available specific to our population. Moreover, it was challenging to determine the extent of care that could be provided by general practitioners at the primary care level, considering there is often suboptimal formal training in palliative medicine both in medical school and during training. It was also crucial to consider the substantial variation in the availability of resources among primary care facilities across different regions of Pakistan. Consequently, the primary emphasis was placed on initial assessment, basic management and treatment aimed at symptomatic relief.
Our study has several limitations that should be acknowledged. First, we did not incorporate input from other stakeholders involved in patient care, such as primary care physicians, other healthcare professionals, external organization experts, and policy makers. This decision was due to constraints in funding, potential conflicts of interest, and logistical difficulties. This omission may have limited the comprehensive perspective of our guidelines on palliative care in LMICs. Given that Pakistan has a significant percentage of rural areas, the feasibility of implementing our CPG in these regions may be limited due to inadequate infrastructure, resources, lack of expertise and/or availability of essential medications. Furthermore, our study defined the criteria for improvement based on the subjective judgment of physicians, introducing the potential for bias in clinical decision-making. The ToR (Terms of Reference) review process, carried out by individual experts, also presents inherent subjectivity and the possibility of bias when determining whether to “adopt”, “adapt”, or “create” recommendations. These limitations underscore the practical challenges and potential biases that arise when applying the optimal GRADE-ADOLOPMENT process, particularly in LMICs such as Pakistan. Nonetheless, efforts can be made to address and mitigate these limitations in future endeavours. While our CPG primarily focuses on management of palliative care for cancer patients, the burden of non-malignancy patients is also significant, possibly limiting the generalizability of our guideline. However, the framework laid can be used to emulate management for other non-malignancy related palliative-care situations for similar effective care.


留言 (0)