
記住我


The randomized (1:1) controlled trial was approved by the ethics committee of the General Hospital of the Aldo Moro University of Bari (approval number 7173 2022 1 22.). The patients signed an informed consent form. The study was performed in accordance with the Helsinki Declaration of 1964, and its later amendments.
Outpatients were randomized in a 1:1 ratio to:
1.A generalized balanced diet adapted to individual body mass index (BMI; NODIET group)
2.A personalized Mediterranean diet (DIET group)
The inclusion criteria were: diagnosis of FM according to the 2016 American College of Rheumatology (ACR) criteria [11], which recommends the use of the widespread pain index (WPI) and the symptoms severity scale (SS); age between 18 and 65 years; and the persistence of diffuse pain and symptoms of FM despite the taking of medication in the 3 months prior to inclusion in the study. In accordance with the routine approach of our center, all patients were prescribed pharmacological treatment with antiepileptic drugs (pregabalin 150–300 mg) and antidepressants (duloxetine 60 mg) [12].
The exclusion criteria were: general medical conditions, including any form of diabetes, and all other neurological disorders that do not meet the FM criteria (including primary headaches and depression).
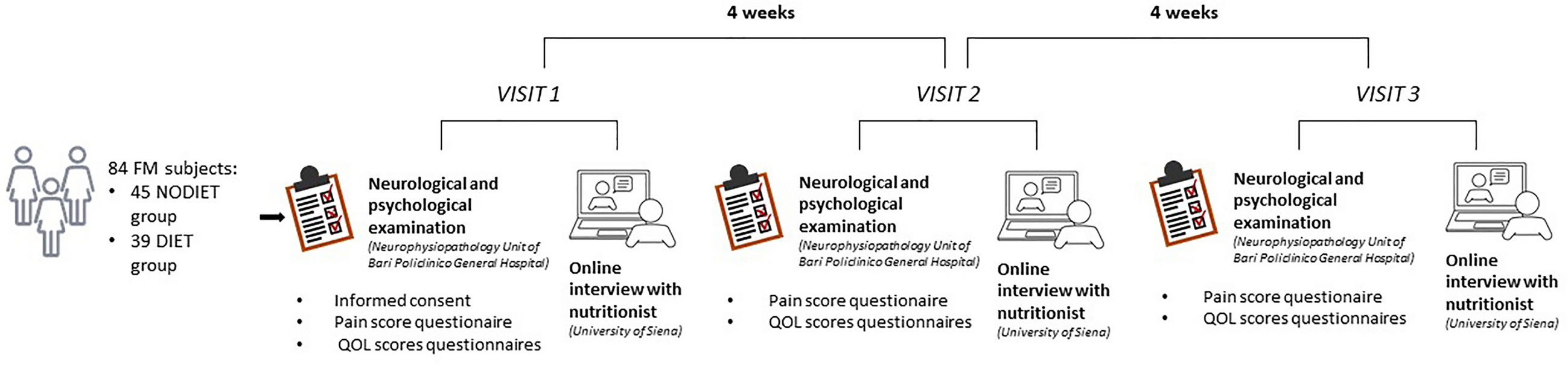
Participants were expected to be met three times: visit 1 (baseline), visit 2 (1-month follow-up), and visit 3 (2-month follow-up). However, since most patients in the NODIET group did not attend the last check-up after 2 months (visit 3), this was restricted to patients in the DIET group.
Personalized Mediterranean DietThe dietary recommendations were drawn up by a team of nutritionists from the University of Siena, who assessed each case and gave each participant individualized dietary recommendations. For all subjects, the diet was assessed according to body mass index (BMI), age, and food allergies (if indicated), as suggested in the Nutrient and Energy Reference Values for the Italian Population (LARN IV Revision) [13]. Calorie intake was planned as follows: 1700 to 1900 kcal/day for patients categorized as normal weight, 1400 to 1600 kcal/day for patients categorized as overweight, and 1100 to 1300 kcal/day for patients categorized as obese.
The proposed diet consisted of five meals a day (breakfast, lunch, dinner, and two snacks) with daily adjustment (from Monday to Sunday) for 4 weeks.
The daily energy intake was divided as follows:
50% from complex carbohydrates with a limit of sugar and sweeteners
30% from fats, with an adequate intake of polyunsaturated fatty acids (PUFA), mainly from extra virgin olive oil, fish and nuts.
20% from proteins, ranging from 0.9 to 1.1 g/kg/die.
In addition, there was a daily intake of fiber ≥ 20 g/die from fruits, vegetables, and starchy foods.
In the DIET group, the daily intake of nutrients was based on the pattern of the Mediterranean diet [14,15,16]. The diet did not include milk and dairy products (the consumption of which is classified as “moderate” in the Mediterranean dietary pattern [17], as the likelihood of lactase enzyme deficiency and associated gastrointestinal problems was considered to be high.
Outcome MeasuresPatients with FM who met the inclusion/exclusion criteria underwent clinical assessment and online contact with the Siena biological team for the diet prescription.
Patients were asked to fill in the following questionnaires:
The eating attitude test (EAT), which indicates the presence of an eating disorder [18], consists of 26 questions to which the respondent can answer: always (3), usually (2), often (1), sometimes (0), rarely (0), or never (0). If the sum is ≥ 20, an eating disorder can be suspected.
The brief pain inventory (BPI) measures both the intensity of pain and how much the pain interferes with the patient’s life. It also asks the patient about pain relief, pain quality and the patient’s perception of the cause of the pain. The BPI uses scales from 0 to 10 to rate the patient [19].
The numeric rating scale (NRS) for pain is a unidimensional measure of pain intensity in adults. The usual format is a horizontal bar or line. The NRS is a single 11-point numeric scale where 0 represents one extreme of pain (e.g., “no pain”) and 10 represents the other extreme of pain (e.g., “worst pain imaginable”).
The self-rating anxiety scale (SAS) introduced by Zung [20] is frequently used in research and clinical practice to assess anxiety. It consists of 20 questions individually scored with 1–4 points, resulting in a raw score of 20–80 points; the standard score is then calculated by int (1.25 raw score) and classified as: 25–49, no anxiety; 50–59, mild anxiety; 60–69, moderate anxiety; and 70–100, severe anxiety.
The self-rating depression scale (SDS) [21] consists of 20 questions individually scored with 1–4 points, resulting in a raw score of 20–80 points; the standard score is then calculated by int (1.25 raw score) and classified as: 25–49, no depression; 50–59, mild depression; 60–69, moderate depression; and 70–100, severe depression.
The multidimensional assessment of fatigue (MAF) scale is a self-administered survey that provides a global fatigue index. It covers four dimensions of fatigue: severity, burden, interference with activities of daily living, and frequency and change over the past week. Overall, 15 questions result in a global value [global fatigue index (GFI)]. The 16th question (“To what extent has your fatigue changed in the last week?”) does not contribute to the GFI. [22]
The fibromyalgia impact questionnaire (FIQ) is a fibromyalgia-specific outcome instrument designed to assess health status, progress and outcomes in patients with fibromyalgia. It contains ten subscales that are combined into a total score. [23].
Body mass index (BMI) was calculated from measurements of weight (using an electronic scale) and height (using a stadiometer) using the Quetelet equation [body mass (kg) / height2 (m2)] (Borga et al. 2018). The BMI data were analyzed as follows: normal weight: BMI 18–25, overweight: BMI 25–30, and obese: BMI 30 + [24].
The experimental design is summarized in Fig. 1.
Fig. 1
Experimental design. DIET, personalized Mediterranean diet; NODIET, general balanced diet; QOL, quality of life
Statistical AnalysisConsidering a 10% change in FIQ score as the primary outcome measure with a 95% confidence interval, a total population of 96 patients was required. The parametric distribution was tested using the Kolmogorov–Smirnov test. As for visit 1 and visit 2, a repeated measures analysis of variance (ANOVA) model with visits as within factor and group as between factor was used to analyze normal data. Visit 3 was not included in this analysis because the control group did not complete visit 3. Hence the DIET group was further analyzed considering the three visits. For this, a one-way repeated measures ANOVA with the factor visit (3 levels: visit 1, visit 2, and visit 3) was used. For the sake of brevity, the data from visit 3 in the DIET group are included in the figures. Statistica® software (StatSoft Inc, Tulsa, USA) was used. The statistical significance was set at p < 0.05.
留言 (0)