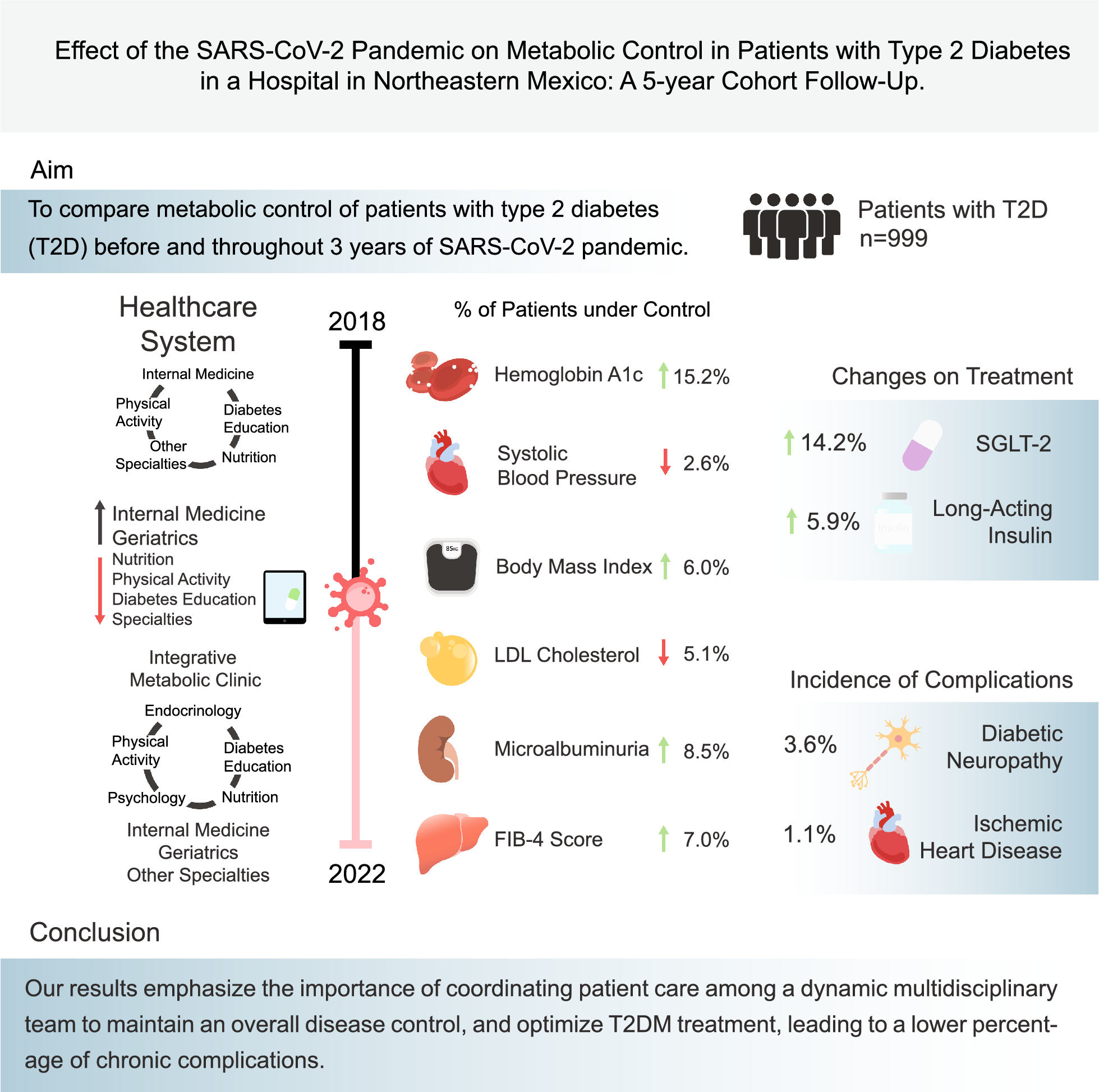
This study focuses on a cohort of 999 patients with T2D patients treated between 2018 and 2022 at a hospital in Northeastern Mexico, where a multidisciplinary team navigated challenges and adaptations during the SARS-CoV-2 pandemic. It was observed that, despite a decrease in in-person consultations and an increase in telemedicine, significant improvements in glycemic control were observed. HbA1c based control proportion was lower before the pandemic and improved in subsequent years. A significant decrease in FG was observed during 2019–2022 compared to 2018, while levels of HbA1c and cholesterol showed no significant changes. The proportion of patients with BMI at goal increased in 2022, and blood pressure control was maintained. The proportion of FIB-4 score 0–1 increased over time. On the other hand, there was a decrease in the proportion of patients with controlled LDL-C during the years in which the pandemic unfolded. Additionally, when the AUC of the metabolic control was compared between subjects that had SARS-CoV-2 infection vs. those that did not, there were higher AUC values in subjects that had SARS-CoV2 in fasting glucose, total cholesterol, LDL-C, triglycerides, diastolic blood pressure, and BMI.
Demographics and proportion of metabolic control parameters
Our population was predominantly male, which aligns with a study of 500,000 patients describing a higher prevalence of type 2 diabetes in male patients of various ethnicities compared to the female population [13]. This predominance of the male population may be related to the diagnosis of diabetes occurring earlier in men than in women, especially between the ages of 35 and 69, consistent with our study’s average age of 60 years [14].
In our population, the proportion of controlled patients based on HbA1c remained in a high range between 53.2 and 73.8%. This contrasts with a study conducted in Mexico City (1998–2005, 2015–2019), which reported a lower proportion with good control between 16 and 37% [15]. Similarly, another study conducted by the National Health and Nutrition Examination Survey from 1999 to 2010 reported a control improvement until early 2010, with a subsequent stall and declination to 50.5% in 2018 [16]. Our controlled proportion was higher and even increased in the following years compared to other populations.
Throughout the study, the proportion of patients with HbA1c levels in control showed an increase and subsequent stabilization in 2020 and 2022 compared to previous years. This contrasts with a meta-analysis from 21 studies, which demonstrated a significant deterioration in HbA1c levels and a decrease in the control proportion during the SARS-COV-2 pandemic compared to previous years [5]. In another study from the U.S. evaluating patients between 1999 and 2018, there was a decrease in the proportion of control, from 57.4 to 50.5% during 2002–2010 [16], even without a pandemic. Our patient’s improvement in control is related to their access to a multidisciplinary team. Despite the reduction of in-person visits to telephone consultations, key diabetes-related specialties remained available for patient care. This is consistent with various studies that state that a multidisciplinary team composed of specialists in the medical field, nutrition, physical activity, and diabetes education has a beneficial effect on reducing HbA1c, FG, and blood pressure levels through constant monitoring, medical guidance, and appropriate treatment, which is consistent with the practices of the metabolic clinic at the hospital [17, 18].
Despite transitioning from traditional in-person consultations to telephonic medical care in 2020, glycemic control improved and stabilized during the pandemic compared to previous years. Similar to our research, a study from Louisiana evaluated the effectiveness of telemedicine in controlling the HbA1c levels during the SARS-COV-2 pandemic, showing a decrease in these levels during the pandemic period [19]. Likewise, a study conducted in Japan in 2019 and 2020, where telemedicine consultations were implemented, found that patients who were within control range prior to the pandemic maintained stable control [20].
A difference in the control proportion of LDL-C levels was observed, with a more significant decrease in 2020. This may correlate with the reduced attendance to nutrition and physical activity consultations due to the prioritization of internal medicine and endocrinology for patient management during the pandemic. Similarly, due to the pandemic and subsequent lockdown, accessibility and availability of food were affected, disrupting the quality of the diet [21], leading to an increase in the consumption of ultra-processed foods and alcohol, and a decreased intake of fruits, vegetables, and whole grains, as well as a decline in physical activity [22, 23].
Analyzing the FIB-4 classification, an increase in patients classified as F0–F1 was observed, with a consequent decrease in those classified as F2. This contrasts with a study that analyzed the trend of hepatic fibrosis in 3 years of 1527 patients with T2D, which showed a decrease in patients with low risk of fibrosis and an increase of intermediate and high-risk patients during the three-year follow-up [24]. This could relate to obesity and high BMI’s association with the development of Metabolic Dysfunction-Associated Liver Disease (MASLD), secondary to the production of proinflammatory cytokines by the adipose tissue that triggers the progression of MASLD [25]. In our population, the higher proportion of low-risk FIB-4 was in 2022, which coincides with the rise of patients with healthy BMI levels in 2022.
SARS-CoV-2 and effects on metabolic control parameters
During the study, we ensured that patient metabolic parameters were not evaluated during acute infection phases. When comparing AUC between subjects with a SARS-CoV-2 infection at any point vs. those without, the former exhibited higher AUC levels of fasting glucose, total cholesterol, LDL-C, diastolic blood pressure, and BMI. This suggests that SARS-CoV-2 could have a deleterious effect on metabolic control for the long term. However, there could also be a bidirectional relation since subjects with poor metabolic control can be more prone to SARS-CoV-2 infection.
In relation to SARS-CoV-2 and glucose metabolism, pre-existing T2D can exacerbate SARS-CoV-2 infection. High glucose promotes SARS-CoV-2 entry by upregulating ACE2 expression. The virus can also impair islet function by directly infecting pancreatic beta cells, restricting insulin secretion, and inducing cell apoptosis. Additionally, SARS-CoV-2 infection can shift glucose metabolism towards aerobic glycolysis through the Warburg effect [26].
Lipid metabolism is indispensable for providing energy, maintaining homeostasis, and regulating the immune response. Lipid droplets have been reported to be associated with antiviral innate immunity. Lipid accumulation has been observed in the lungs of SARS-CoV-2 patients. Furthermore, significant lipidomic alterations have been linked to SARS-CoV-2 severity since fatty acids are essential for SARS-CoV-2 replication [26].
SARS-CoV-2 specifically recognizes and attaches human angiotensin-converting enzyme 2 (ACE2) for entry via the S protein. Different ACE2 polymorphisms, such as rs2074192, have been associated with hypertension in obese males. Additionally, previous studies have shown a higher incidence of hypertension post- SARS-CoV-2 infection [28].
The relation between higher BMI and SARS-CoV-2 infection can be explained through multiple mechanisms, such as altered respiratory anatomy related to fat deposits in the mediastinum and abdomen and reduced chest wall elasticity. Also, obese subjects have an imbalance of coagulant factors, increased leptin resistance, B cell and T cell impairment, complement system overreaction, and poor antibody response. Adipose tissue, serving as a viral reservoir, could prolong virus shedding in obese patients and increase viral replication [29].
Visits to medical specialties
Regarding consultations, all patients are under close monitoring by an internist or geriatrician depending on their age, aiming for adherence to the ADA 2024 guidelines for continuous monitoring of patients with T2D [30]. There was a decrease in the assistance to ophthalmology, diabetes education, nutrition, and physical activity consultations, while endocrinology and cardiology consultations increased. Nephrology and neurology consultations remained unchanged.
There was a decrease in attendance at ophthalmology consultations. According to the ADA 2024 guidelines, it is recommended that all patients with T2D have a comprehensive eye examination by an ophthalmologist at the time of diagnosis and annually if there are signs of retinopathy. However, when there is no evidence of retinopathy in one or more annual eye exams and glucose parameters are under control, screening tests can be conducted every 2 years [31]. Due to the low incidence of diabetic retinopathy in our population compared to others [32, 33] and patients maintaining controlled glucose levels, the less frequent referral to ophthalmology can be justified, leading to a decrease in attendance for these consultations.
The ADA does not provide a specific recommendation for a minimum number of endocrinology consultations for patients with T2D; however, it emphasizes the value of a multidisciplinary team [31]. At the onset of the pandemic, there was an increase in attendance for endocrinology and cardiology consultations, which can be interpreted as an effort to maintain and increase the proportion of patients in control based on HbA1c, FG, and lipid levels, as well as a compensatory response to the decreased attendance in diabetes education, nutrition, and physical activity consultations. Like our population, a study mentions that patients with well-controlled T2D can receive adequate care through an internist, nutritionist, and diabetes educator. It also states that consultations with an endocrinologist are reserved for the care and treatment of more complex patients [34].
There was no significant change in attendance for nephrology and neurology consultations. This is because, referral to these specialties should be considered in specific situations of greater complexity [11]. Diabetic nephropathy and neuropathy are the most common complications in our population over the 5-year period, which explains the consistent attendance for these consultations.
T2D management
Prescription of oral hypoglycemic agents increased between 2019 and 2022, except for sulfonylureas, which decreased in this same period. This finding aligns with a study conducted in Germany that analyzed the change in glucose-lowering regimens during the SARS-CoV-2 pandemic, showing an increased prescription of different oral hypoglycemic agents such as biguanides, DPP-4 inhibitor, SGLT2 inhibitors and GLP-1 analogs between 2019 and 2020 [35], with a higher increase in SGLT2 inhibitors, same as our study. This can be related to its positive outcomes regarding glycemic control and other beneficial effects, such as cardiovascular protection, blood pressure reduction, and improved kidney function, which could have been beneficial during the pandemic as an additional vital organ protection [36].
Between 2018 and 2022, there was an increase in the prescription of oral hypoglycemic agents and insulin and a decrease in sulfonylureas. This coincides with research conducted in Mexico City that analyzed trends in management from 1998 to 2004 and from 2015 to 2019. Said study found a general increase in glucose-lowering medication, a moderate increase in insulin use, and a decrease in sulfonylureas [15]. The increase in the prescription of hypoglycemic agents can be attributed to the progressive nature of type 2 diabetes, necessitating combined therapies for maintaining glycemic targets. The ADA 2024 recommends the prescription of an additional medication to metformin to maintain HbA1c targets [37] which explains the increase of all hypoglycemic agents and long-acting insulin prescription. Conversely, while sulfonylureas persist as one of the most prescribed second-line agents, their usage is diminishing due to the emergence of new, beneficial, and safer treatment options for patients [38].
Incidence of micro and macrovascular complications
Our population showed a low incidence of complications over the 5-year study compared to other populations. A study conducted in India reported that at least 46% of its population had some complication secondary to T2D [39]. Another study in Arabia reported an incidence of 76% of its population with T2D-associated complications [40]. The low occurrence of complications in our population relates to stable levels of HbA1c and FG, as chronic hyperglycemia is a significant factor in the development of microvascular complications, secondary to the impairment of capillary microvasculature by the activity of the polyol pathway [41].
Our study found a higher proportion of microvascular complications compared to macrovascular ones, with diabetic neuropathy being the most frequent complication in our population. This relates to a study conducted in Asia, which identified a higher prevalence of microvascular complications and a greater prevalence of diabetic neuropathy [42]. Similarly, a U.S. study analyzing patients from various ethnic backgrounds reported a higher incidence of diabetic neuropathy, followed by nephropathy, aligning with our results [43]. The higher prevalence of this complication is linked to an increased risk of diabetic neuropathy with advancing age. Age greater than 60 years is associated with a heightened risk of developing diabetic neuropathy due to biological aging processes such as alterations in nerve vasculature, increased advanced glycation end products, and decreased resistance to oxidative stress products [44].
Relevance and limitations
The relevance of this study relies on its tight 5-year follow-up of a cohort of 999 patients from a poorly studied population managed by an adaptative multidisciplinary team. It demonstrated adequate glycemic control, even during the SARS-COV-2 pandemic, along with a low rate of complications compared to other studied populations.
This study has various limitations; the main limitation lies in its retrospective nature, which limits patients who had a follow-up through medical records. The assessment of the cohort was not uniform; due to the nature of the SARS-CoV-2 pandemic, some subjects did not have an evaluation at all time points. Additionally, the sample may not be representative of the general population as it reflects a population managed by a specific healthcare system in a Northeast Mexican region; however, if this health system model is replicated in other regions, it could aid in diabetes control. For future research, it would be relevant to address risk factors influencing patients' metabolic control, such as lifestyle changes and psychosocial factors. This could contribute to the development of strategies for prevention and intervention in future situations like the SARS-COV-2 pandemic.





留言 (0)