
記住我



‘The most sophisticated intensive care often becomes unnecessarily expensive terminal care where the pre-ICU system is uncoordinated or undeveloped’ – Peter Safar, 1974
Critical illness refers to life-threatening conditions resulting from an acute disease, injury, adverse environmental influence, poisoning, surgery, or decompensation of a chronic disease. It is an exquisitely time-sensitive condition, and early identification, support, and treatment significantly impact outcome. Pathologies which have the potential to become life-threatening often originate before the patient presents to the hospital, which explains the prevalence of evolving or established critical illness seen in the emergency departments (EDs). The common maxim where ‘prevention is better than cure’ implies that the earlier the treatment the better the outcome in other words, ‘the earlier the better’. It is obvious and advantageous that evidence-based critical care should not be limited to the ICU but rather initiated as early as possible and regardless of the geographical location, whether in the prehospital setting or ED. Peter Safar was the first to indicate that efforts to enhance the chances of survival and organ recovery from critical illness must not only focus on patient management in the ICU, but address the entire patient pathway from the prehospital scene, the ED to the ICU, further including the operating room and general wards [1]. He referred to critical care as the continuum of care the critically ill or injured patient requires to recover.
An USA study reported that the number of ED admissions to an ICU increased by 79% between 2001 and 2009. The time that these critically ill patients spent in the ED also increased in parallel [2]. A systematic review showed that ED boarding of critically ill patients was common, and this specific aspect alone was associated with worse clinical outcomes [3,4]. Gaieski et al. observed an increased delay in critical care as ED occupancy increased, implying that ED overcrowding might affect patient outcome [5]. A 2009 study described low rates of critical care interventions in the ED as a contributing factor to poor outcome [6]. However, more recent publications demonstrate no association between ED boarding and mortality, when appropriate critical care is delivered in the ED [7,8]. Essential critical care interventions such as basic airway management in patients with compromised airways as well as chest compressions and defibrillation in cardiac arrest are known to save lives [9]. Even advanced techniques such as extracorporeal life support further improve the chances of survival in patients with refractory cardiac arrest, when introduced early after collapse or on ED arrival [9–11]. After the initial resuscitation phase, critical care must be continued without interruption to optimally stabilize vital functions, minimize organ damage, and avoid renewed deterioration. Current scientific evidence suggests that early delivery of critical care in the ED can halt and, in some patients, even reverse acute organ dysfunction [12,13], reduce the need for ICU admission, shorten ICU and hospital length of stay, and improve both short-term as well as long-term survival [12–17]. These positive effects on patient outcome further translate into increased ICU bed availability for critically ill patients originating from other hospital areas than the ED (e.g. patients after major elective surgery or those deteriorating on hospital wards). An economic analysis revealed that critical care delivery in the ED is cost-effective [18], a finding that is of particular importance in healthcare systems with payment-per-diagnosis reimbursement.
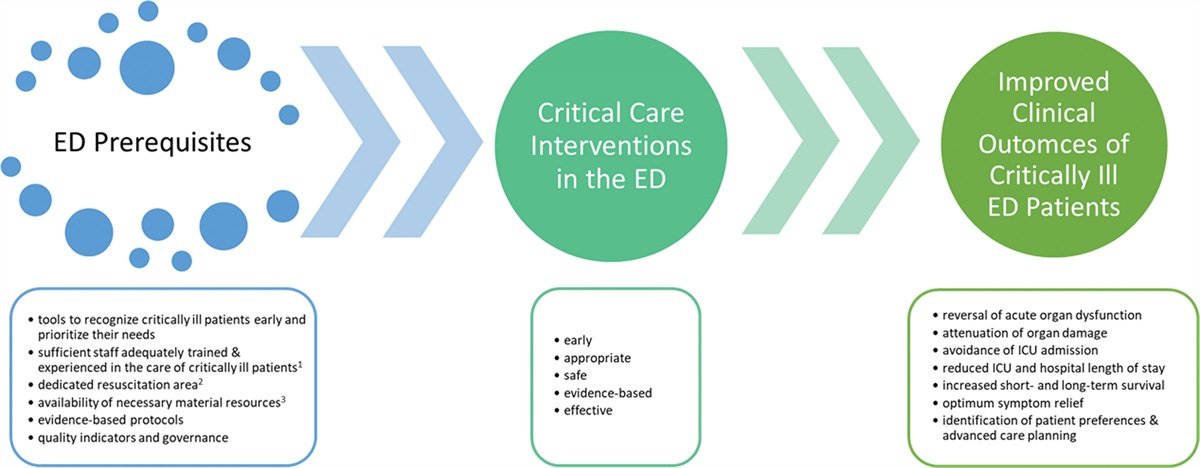
Several models on how to provide critical care in the ED have been published. These critical care delivery solutions vary substantially ranging from the ‘ICU without walls’ model, where ICU staff goes to the ED when needed, to direct ICU or coronary angiography suite admission of selected emergency patients (e.g. those with ST-elevation myocardial infarction), ED-based early intervention teams, telemonitoring solutions, dedicated critical care resuscitation units, and ED-ICUs staffed by emergency physicians [13,14,17,19]. Although scientific data on the comparative effectiveness of the different ED critical care delivery models are lacking, it is unlikely that a single model will be suitable and effective in all settings. Given the substantial differences in ED structures, organization, staffing and processes between hospitals, regions, and countries in Europe [20], it appears that EDs must choose the most feasible and appropriate ED critical care delivery model for their setting. Regardless of the model chosen, the practicability of critical care in the ED hinges on the availability of specific prerequisites (Fig. 1).
 Fig. 1:
Fig. 1: Overview of prerequisites, critical care interventions, and associated effects of critical care provision in the emergency department on patient outcomes. 1, including training and experience in technical and non-technical skills; 2, area where critically ill patients can be resuscitated, stabilized, and monitored until disposition to an ICU, non-ICU ward, or ED discharge; 3, equipment, drugs, and consumables needed for continuous patient monitoring (e.g. end-tidal carbon dioxide, invasive pressure measurement), rapid diagnostic work-up (e.g. point-of-care tests including blood gas analysis and viscoelastic tests, bedside point-of-care ultrasound), and critical care interventions (e.g. rapid sequence induction, noninvasive and invasive mechanical ventilation, continuous infusion of vasodilators, vasopressors or inotropic agents, extracorporeal life support). ED, emergency department.
ED critical care encompasses more than resuscitation, interventions, and continuous patient monitoring. In patients too old, frail, and/or sick to benefit from ICU admissions, effective and timely diagnostics and noninvasive critical care interventions (e.g. noninvasive positive pressure ventilation) can rapidly help to clarify the underlying pathology, relieve symptoms, and may even reverse organ dysfunction. A time-limited trial of noninvasive organ support in the ED facilitates the assessment of physiological reserves contributing to the decision whether to continue with organ support or turn focus to palliative care measures [21]. Another key patient-centred aspect of providing critical care in the ED is the creation of an opportunity to discuss and document patient preferences and advanced care planning before ICU and hospital admission. As a minimum, the first-line, foundational care of critically ill patients, termed Essential Emergency and Critical Care [22], should be provided to all critically ill patients in the ED and throughout the hospital.
A further advantage of the systematic delivery of critical care in the ED is the possibility to harmonize and expand critical care research to early phases of critical illness. Delayed study inclusion (e.g. only after ICU admission) may be one of the reasons why some putatively effective therapies did not translate into improved outcomes [23].
As a European group of emergency and critical care physicians, we would like to emphasize the importance and unquestionable need for timely critical care delivery in the ED. The ED treatment phase is a crucial part of the continuum of care for critically ill patients. Early evidence-based critical care interventions in the ED can effectively attenuate or even reverse organ dysfunction and possibly even improve the chances of survival. Further research will be essential to validate these findings across the various healthcare systems and geographical regions.
AcknowledgementsThe Critical Care in Emergency Medicine Interest Group:
Mo Al-Hadad, MD, Intensive Care Unit, Queen Elizabeth University Hospital, Glasgow, United Kingdom; Raed Arafat, MD, Department of Emergency Situations, Ministry of Internal Affairs, Bucharest, Romania; Tim Baker, MBChB, PhD, Department of Global Public Health, Karolinska Institutet, Stockholm, Sweden; Martin Balik, MD, PhD, Department of Anaesthesiology and Intensive Care, 1st Faculty of Medicine, Charles University and General University Hospital in Prague, Czechia; Wilhelm Behringer, MD, MBA, MSc, Department of Emergency Medicine, Medical University of Vienna, Vienna, Austria; Ruth Brown, MB, BS, FRCEM, FIFEM, Emergency Department, St Mary’s Hospital, Imperial College Healthcare NHS Trust, London, United Kingdom; Luca Carenzo, MD, Department of Anesthesia and Intensive Care Medicine, IRCCS Humanitas Research Hospital, Rozzano, Milan, Italy; Jim Connolly, MD, Accident and Emergency, Great North Trauma and Emergency Care, Newcastle-upon-Tyne, United Kingdom; Daniel Dankl, MD, Department of Anesthesiology, Perioperative and General Intensive Care, Salzburg University Hospital and Paracelsus Private Medical University, Salzburg, Austria; Christoph Dodt, MD, Department of Emergency Medicine, München Klinik, Munich, Germany; Martin W. Dünser, MD, Department of Anaesthesiology and Critical Care Medicine, Kepler University Hospital and Johannes Kepler University Linz, Linz, Austria; Aristomenis Exadaktylos, MD, Department of Emergency Medicine, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland; Tobias Gauss, MD, Anesthesia and Critical Care, Grenoble Alpes, University Hospital, Grenoble, France; Srdjan Gavrilovic, MD, Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia and Institute for Pulmonary Diseases of Vojvodina, Sremska Kamenica, Serbia; Said Hachimi-Idrissi, MD, PhD, Department of Emergency Medicine, Ghent University Hospital, Ghent, Belgium and Faculty of Medicine and Pharmacy, Vrije Universiteit Brussels, Brussels, Belgium; Matthias Haenggi, MD, Institute of Intensive Care Medicine, University Hospital Zürich and University of Zürich, Zürich, Switzerland; Harald Herkner, MD; Michael Joannidis, MD, Division of Intensive Care and Emergency Medicine, Department of Internal Medicine, Medical University Innsbruck, Innsbruck, Austria; Abdo Khoury, MD, PhD, Department of Emergency Medicine and Critical Care, Besançon University Hospital, Besançon, France; Michaela Klinglmair, RN, Department of Anaesthesiology and Critical Care Medicine, Kepler University Hospital and Johannes Kepler University Linz, Linz, Austria; Robert Leach, MD, Department of Emergency Medicine, Centre Hospitalier de Wallonie Picarde, Tournai, Belgium; Marc Leone, MD, Department of Anesthesiology and Intensive Care Unit, North Hospital, Aix Marseille Université, Assistance Publique Hôpitaux Universitaires de Marseille, Marseille, France; David Lockey, MD, University of Bristol, Bristol, United Kingdom; Jens Meier, MD, Department of Anaesthesiology and Critical Care Medicine, Kepler University Hospital and Johannes Kepler University Linz, Linz, Austria; Matthias Noitz, MD, Department of Anaesthesiology and Critical Care Medicine, Kepler University Hospital and Johannes Kepler University Linz, Linz, Austria; Roberta Petrino, MD, Emergency Medicine Unit, Ospedale Regionale di Lugano, EOC, Switzerland; Sirak Petros, MD, Medical ICU, University Hospital of Leipzig, Leipzig, Germany; Patrick Plaisance, MD, PhD, Emergency Department, Hôpital Lariboisière, Paris, France; Jacobus Preller, FRCP, John Farman ICU, Cambridge University Hospital NHS Foundation Trust, Cambridge, United Kingdom; Luis Garcia-Castrillo Riesgo, MD, Emergency Department, Hospital Marqués de Valdecilla, Santander, Spain; Carl Otto Schell, MD, Department of Global Public Health, Karolinska Institutet, Stockholm, Sweden and Centre for Clinical Research, Sörmland, Uppsala University, Uppsala, Sweden; Jana Šeblová, MD, PhD, Paediatric Emergency Department, Motol University Hospital, Prague, Czechia; Christian Sitzwohl, MD, Department of Anaesthesiology and Intensive Care Medicine, St. Josef Hospital Vienna, Vienna, Austria; Christian Baaner Skjaerbaek, MD, Emergency Department, Regionshospitalet Randers, Randers, Denmark; Markus Skrifvars, MD, PhD, Department of Emergency Care and Services, Helsinki University Hospital and University of Helsinki, Helsinki, Finland; Kjetil Sunde, MD, PhD, Department of Anesthesia and Intensive Care Medicine, Oslo University Hospital and Institute of Clinical Medicine, University of Oslo, Oslo, Norway; Tina Tomić Mahečić, MD, PhD, Department of Anesthesiology and Intensive Care Medicine, Clinical Hospital Centre Zagreb, Zagreb, Croatia; Helmut Trimmel, MD, Department of Anesthesiology, Emergency and Critical Care Medicine General Hospital Wiener Neustadt, Wiener Neustadt, Austria; Andreas Valentin, MD, Department of Internal Medicine, Cardiology and Intensive Care Medicine, Klinik Donaustadt, Vienna, Austria; Volker Wenzel, MD, Department of Anesthesiology, Intensive Care Medicine, Pain Therapy and Emergency Medicine, Klinikum Friedrichshafen, Friedrichshafen, Germany and Department of Anesthesiology, University of Florida, Gainesville, Florida, USA
Conflicts of interestThere are no conflicts of interest.
References 1. Safar P. Critical care medicine – quo vadis? Crit Care Med 1974; 2:1–5. 2. Herring AA, Ginde AA, Fahimi J, Alter JH, Maselli JH, Espinola JA, et al. Increasing critical care admissions from US emergency departments, 2001–2009. Crit Care Med 2013; 41:1197–1204. 3. Mohr NM, Wessmann BT, Bassin B, Ellie-Turenne MC, Ellender T, Emlet LL, et al. Boarding of critically ill patients in the emergency department. Crit Care Med 2020; 48:1180–1187. 4. Roussel M, Teissandier D, Yordanov Y, Balen F, Noizet M, Tazarourte K, et al. Overnight stay in the emergency department and mortality in older patients. JAMA Intern Med 2023; 183:1378–1385. 5. Gaieski DF, Agarwal AK, Mikkelsen ME, Brumheller B, Sante SC, Shofer FS, et al. The impact of ED crowding on early interventions and mortality in patients with severe sepsis. Am J Emerg Med 2017; 35:953–960. 6. Green RS, MacIntyre JK. Critical care in the emergency department: an assessment of the length of stay and invasive procedures performed on critically ill ED patients. Scand J Trauma Resusc Emerg Med 2009; 17:47. 7. Agustin M, Price LL, Andoh-Duku A, LaCamera P. Impact of delayed admission to the intensive care unit from the emergency department upon sepsis outcomes and sepsis protocol compliance. Crit Care Res Pract 2017; 2017:9616545. 8. Puls HA, Haas NL, Cranford JA, Medlin RP Jr, Bassin BS. Emergency department length of stay and outcomes of emergency department-based intensive care unit patients. J Am Coll Emerg Physicians Open 2022; 3:e12684. 9. Soar J, Böttiger BW, Carli P, Couper K, Deakin CD, Djärv T, et al. European Resuscitation Council Guidelines 2021: adult advanced life support. Resuscitation 2021; 161:115–151. 10. Low CJW, Ramanathan K, Ling RR, Ho MJC, Chen Y, Lorusso R, et al. Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with cardiac arrest: a comparative meta-analysis and trial sequential analysis. Lancet Respir Med 2023; 11:883–893. 11. Balik M, Porizka M, Matousek V, Brestovansky P, Svobodova E, Flaksa M, et al. Management of accidental hypothermia: an established extracorporeal membrane oxygenation centre experience. Perfusion 2019; 34(1 Suppl):74–81. 12. Giacomini M, Iapichino G, Cigada M, Minuto A, Facchini R, Noto A, et al. Short-term noninvasive pressure support ventilation prevents ICU admittance in patients with acute cardiogenic pulmonary edema. Chest 2003; 123:2057–2061. 13. Gunnerson KJ, Bassin BS, Havey RA, Haas NL, Sozener CB, Medlin RP Jr, et al. Association of an emergency department-based intensive care unit with survival and inpatient intensive care unit admissions. JAMA Netw Open 2019; 2:e197584. 14. Schober A, Sterz F, Herkner H, Locker GJ, Heinz G, Fuhrmann V, et al. Post-resuscitation care at the emergency department with critical care facilities – a length-of-stay analysis. Resuscitation 2011; 82:853–858. 15. Haas NL, Medlin RP Jr, Cranford JA, Boyd C, Havey RA, Losman ED, et al. An emergency department-based intensive care unit is associated with decreased hospital length of stay for upper gastrointestinal bleeding. Am J Emerg Med 2021; 50:173–177. 16. Du J, Gunnerson KJ, Bassin BS, Meldrum C, Hyzy RC. Effect of an emergency department intensive care unit on medical intensive unit admissions and care: a retrospective cohort study. Am J Emerg Med 2021; 46:27–33. 17. Mitarai T, Gordon AJ, Nudelman MJR, Urdaneta AE, Nesbitt JL, Niknam K, et al. Association of an emergency critical care program with survival and early downgrade among critically ill medical patients in the emergency department. Crit Care Med 2023; 51:731–741. 18. Bassin BS, Haas NL, Sefa N, Medlin R, Peterson TA, Gunnerson K, et al. Cost-effectiveness of an emergency department-based intensive care unit. JAMA Netw Open 2022; 5:e2233649. 19. Jayaprakash N, Pflaum-Carlson J, Gardner-Gray J, Hurst G, Coba V, Kinni H, et al. Critical care delivery solutions in the emergency department models in caring for ICU boarders. Ann Emerg Med 2020; 76:709–716. 20. Behringer W, Brown R. Status of the specialty emergency medicine in Europe. Eur J Emerg Med 2023; 30:386–388. 21. Vink EE, Azoulay E, Caplan A, Kompanje EJO, Bakker J. Time-limited trial of intensive care treatment: an overview of current literature. Intensive Care Med 2018; 44:1369–1377. 22. Schell CO, Khalid K, Wharton-Smith A, Oliwa J, Sawe HR, Roy N, et al. Essential emergency and critical care: a consensus among global clinical experts. BMJ Glob Health 2021; 6:e006585. 23. Ospina-Tascón GA, Büchele GL, Vincent JL. Multicenter, randomized, controlled trials evaluating mortality in intensive care: doomed to fail? Crit Care Med 2008; 36:1311–1322.
留言 (0)