
記住我


A total of 403 patients with clinical stage IA IMA were met our inclusion criteria. Among them, 316 patients (78.4%, 316/403) underwent lobectomy, and 87 patients (21.6%, 87/403) were treated by limited resection. Among limited resection group, 28 patients underwent segmentectomy and 59 patients underwent wedge resection. Patients were classified into two groups according to surgical types and the clinicopathological characteristics were summarized and compared in Table 1. There are no significant differences between patients in limited resection group and lobectomy group in terms of age (p = 0.156), sex (p = 0.149), smoking status (p = 0.626), CEA (p = 0.432), %predicted forced expiratory volume in 1 s (FEV 1) (p = 0.103), cardiovascular disease (p = 0.083), diabetes mellitus (p = 0.103). Patients in the limited resection group had smaller tumor size than those in the lobectomy group. The median follow-up time was 46 months (range, 24 to 82 months) and 43 months (range, 21 to 80 months) in lobectomy and limited resection groups, respectively.
Table 1 Baseline Characteristics of Patients with Stage IA Invasive Mucinous Adenocarcinoma of Shanghai Pulmonary Hospital Cohort374 (92.8%, 374/403) tumors were pure IMA, and 29 tumors (7.2%, 29/403) were mixed mucinous/nonmucinous ADC: 15 (51.7%,15/29) tumors with acinar pattern, 8 (27.6%, 8/29) tumors with papillary pattern, and 6 (20.7%, 6/29) tumors with acinar and papillary pattern (Supplementary Fig. 1).
Outcomes of patients with clinical stage IA invasive lung mucinous adenocarcinomasThe survival analysis by Log-rank test showed that patients who underwent lobectomy had a similar RFS (5-year RFS: 82.6% versus. 79.3%; p = 0.116) and OS (5-year OS: 88.3% versus. 86.2%; p = 0.235) than those who underwent limited resection (Fig. 1A, B). Patients with IMA > 2.1 to 3 cm had worse RFS (5-year RFS: 73.7% versus. 86.1%; p = 0.007) than those with IMA ≤ 2 cm, whereas similar OS was observed between the two groups (5-year OS: 83.9% versus. 89.8%; p = 0.105) (Fig. 1C, D).
Fig. 1
Recurrence-free survival (RFS) and overall survival (OS) in patients with clinical stage IA lung IMA stratified by surgical procedures and tumor size. (A) RFS by surgical procedures in patients with clinical stage IA lung IMA. (B) OS by surgical procedures in patients with clinical stage IA lung IMA. (C) RFS by tumor size for patients with clinical stage IA lung IMA. (D) OS by tumor size for patients with clinical stage IA lung IMA
Lob, lobectomy; Lim, limited resection
In further multivariable Cox analysis, lymph node metastasis (hazard ratio [HR], 4.204; 95% confidence interval [CI], 2.126–8.315; p < 0.001) and IMA > 2.1 to 3 cm (HR, 1.286; 95% CI, 1.019–1.621; p = 0.033) were independent risk factors of worse RFS. In terms of OS, lymph node metastasis (HR, 4.497; 95% CI, 2.106–9.603; p < 0.001) was the only independent risk factor (Table 2).
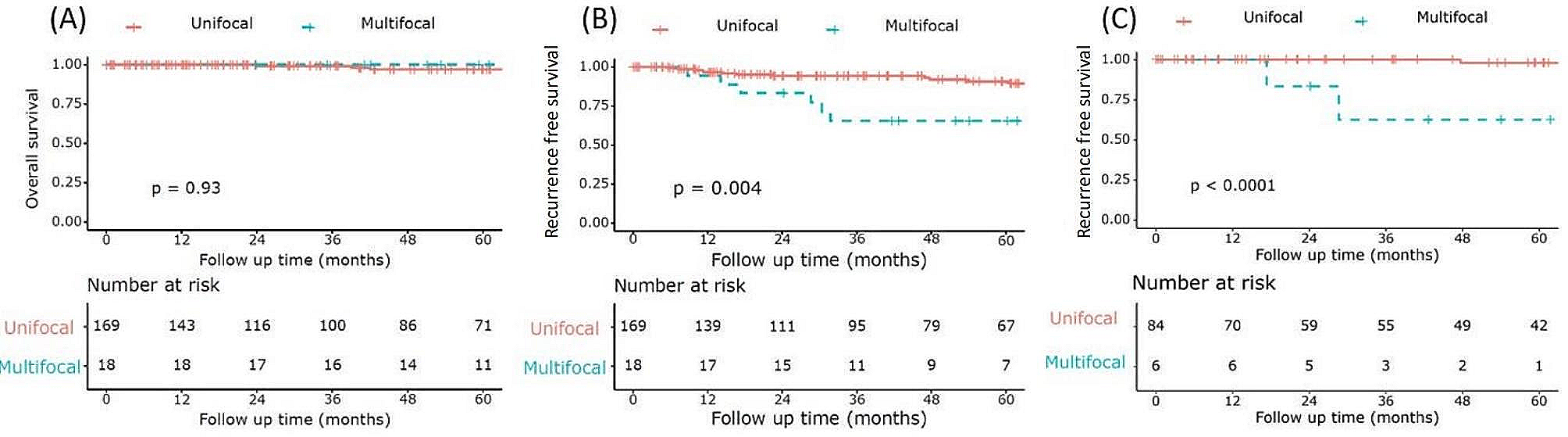
Table 2 Cox Proportional-hazards Regression Model for Recurrence-free Survival and Overall Survival in Patients with IMA ≤ 3 cm of Shanghai Pulmonary Hospital Cohort (n = 403)Outcomes of patients with clinical stage IA invasive lung mucinous adenocarcinomas ≤ 2 cmThere were 266 patients in the subgroup of IMA ≤ 2 cm, including 67 patients who underwent limited resection and 199 patients who underwent lobectomy. The survival analysis by Log-rank test showed that patients undergoing lobectomy had a similar RFS (5-year RFS: 88.1% versus. 85.4%; p = 0.953) and OS (5-year OS: 89.9% versus. 89.6%; p = 0.552) than those who underwent limited resection. (Fig. 2A, B) Multivariable Cox proportional hazards regression model showed that lymph node metastasis was the independent risk factor of worse RFS (HR, 6.981; 95% CI, 2.433–20.034; p < 0.001) and OS (HR, 4.296; 95% CI, 1.291–14.297; p = 0.020) (Table 3).
Fig. 2
Recurrence-free survival (RFS) and overall survival (OS) in patients with clinical stage IA lung IMA stratified by surgical procedures and tumor size. (A) RFS by surgical procedures in patients with clinical stage IA lung IMA ≤ 2 cm. (B) OS by surgical procedures in patients with clinical stage IA lung IMA ≤ 2 cm. (C) RFS by surgical procedures for patients with clinical stage IA lung IMA > 2 to 3 cm. (D) OS by surgical procedures for patients with clinical stage IA lung IMA > 2 to 3 cm
Lob, lobectomy; Lim, limited resection
Table 3 Cox Proportional-hazards Regression Model for Recurrence-free Survival and Overall Survival in Patients with IMA ≤ 2 cm (n = 266) and > 2 to 3 cm of Shanghai Pulmonary Hospital Cohort (n = 137)Outcomes of patients with clinical stage IA invasive lung mucinous adenocarcinomas 2–3 cm137 patients were included in the subgroup of IMA > 2.1–3 cm, which 20 patients underwent limited resection and 117 patients underwent lobectomy. There was a significant difference in RFS between lobectomy and limited resection (5-year RFS: 77.8% versus. 50.0%; p = 0.007) in the group with IMA > 2.1–3 cm, however, similar OS were observed (5-year OS: 85.5% versus. 75.0%; p = 0.112) (Fig. 2C, D). The multivariable Cox proportional hazards regression model reveals limited resection (HR, 2.417; 95% CI, 1.157–5.049; p = 0.019) and lymph node metastasis (HR, 3.444; 95% CI, 1.492–7.949; p = 0.004) were the independent risk of worse RFS. Lymph node metastasis (HR, 4.059; 95% CI, 1.495–11.025; p = 0.005) was the only independent risk of worse OS (Table 3).
The SEER cohortPatient characteristicsWe identified 480 patients from the SEER database who had stage T1 disease with invasive mucinous adenocarcinoma 403 (403/480 84.0%) or mucinous bronchiolo-alveolar carcinoma 68 (68/480 14.1%) or mixed mucinous and non-mucinous bronchiolo-alveolar carcinoma 9 (9/480 1.9%). Among them, 376 (376/480 78.3%) were underwent lobectomy, and 104 (104/480 21.7%) were treated by limited resection. Clinicopathological characteristics of the patients are summarized in Table 4. There are no significant differences between patients in limited resection group and lobectomy group in terms of sex (p = 0.741), age (p = 0.116), race/ethnicity (p = 0.965), tumor location (p = 0.331), and histology (p = 0.712). Patients in the limited resection group had smaller tumor size (p = 0.002) and fewer lymph nodes involvement (p = 0.005) than those in the lobectomy group.
Table 4 Baseline Characteristics of Patients with Stage IA Invasive Mucinous Adenocarcinoma of Seer Cohort(n = 480)Outcomes of patients with invasive lung mucinous adenocarcinomas ≤ 2 cmThe survival analysis by log-rank test showed that patients undergoing lobectomy had a similar LCSS (5-year LCSS: 91.0% versus 91.1%; p = 0.703) and OS (5-year OS: 88.3% versus 84.8%; p = 0.830) than those who underwent limited resection. (Fig. 3A, B) Multivariable Cox proportional hazards regression model showed that lymph node metastasis (HR, 8.234; 95% CI, 3.586–18.904; p < 0.001) was the independent risk factor of worse LCSS. And lymph node metastasis (HR, 7.778; 95% CI, 3.730-16.217; p < 0.001) was an independent predictive factor of worse OS.
Fig. 3
Lung cancer–specific survival (LCSS) and overall survival (OS) in patients with stage T1 lung IMA stratified by surgical procedures and tumor size. (A) LCSS by surgical procedures in patients with clinical stage T1 lung IMA ≤ 2 cm. (B) OS by surgical procedures in patients with clinical stage T1 lung IMA ≤ 2 cm. (C) LCSS by surgical procedures for patients with clinical stage T1 lung IMA > 2 to 3 cm. (D) OS by surgical procedures for patients with clinical stage T1 lung IMA > 2 to 3 cm
Lob, lobectomy; Lim, limited resection
Outcomes of patients with invasive lung mucinous adenocarcinomas 2–3 cmIn the group with IMA > 2–3 cm, there was a significant difference in LCSS between lobectomy and limited resection (5-year LCSS: 92.8% versus 64.0%; p < 0.001), and similar OS were observed (5-year OS: 90.2% versus 60.0%; p < 0.001) (Fig. 3C, D). The multivariable Cox proportional hazards regression model reveals limited resection (HR, 10.066; 95% CI, 3.571–28.376; p < 0.001) and lymph node metastasis (HR, 14.346; 95% CI, 4.962–41.476; p < 0.001) were the independent risk of worse LCSS. Limited resection (HR, 8.527; 95% CI, 3.355–21.676; p < 0.001) and lymph node metastasis (HR, 11.199; 95% CI, 4.188–29.950; p < 0.001) were independent risk of worse OS (Table 5).
Table 5 Cox Proportional-hazards Regression Model for Recurrence-free Survival and Overall Survival in Patients with IMA ≤ 2 cm (n = 302) and > 2 to 3 cm of SEER Cohort (n = 178)
留言 (0)