
記住我





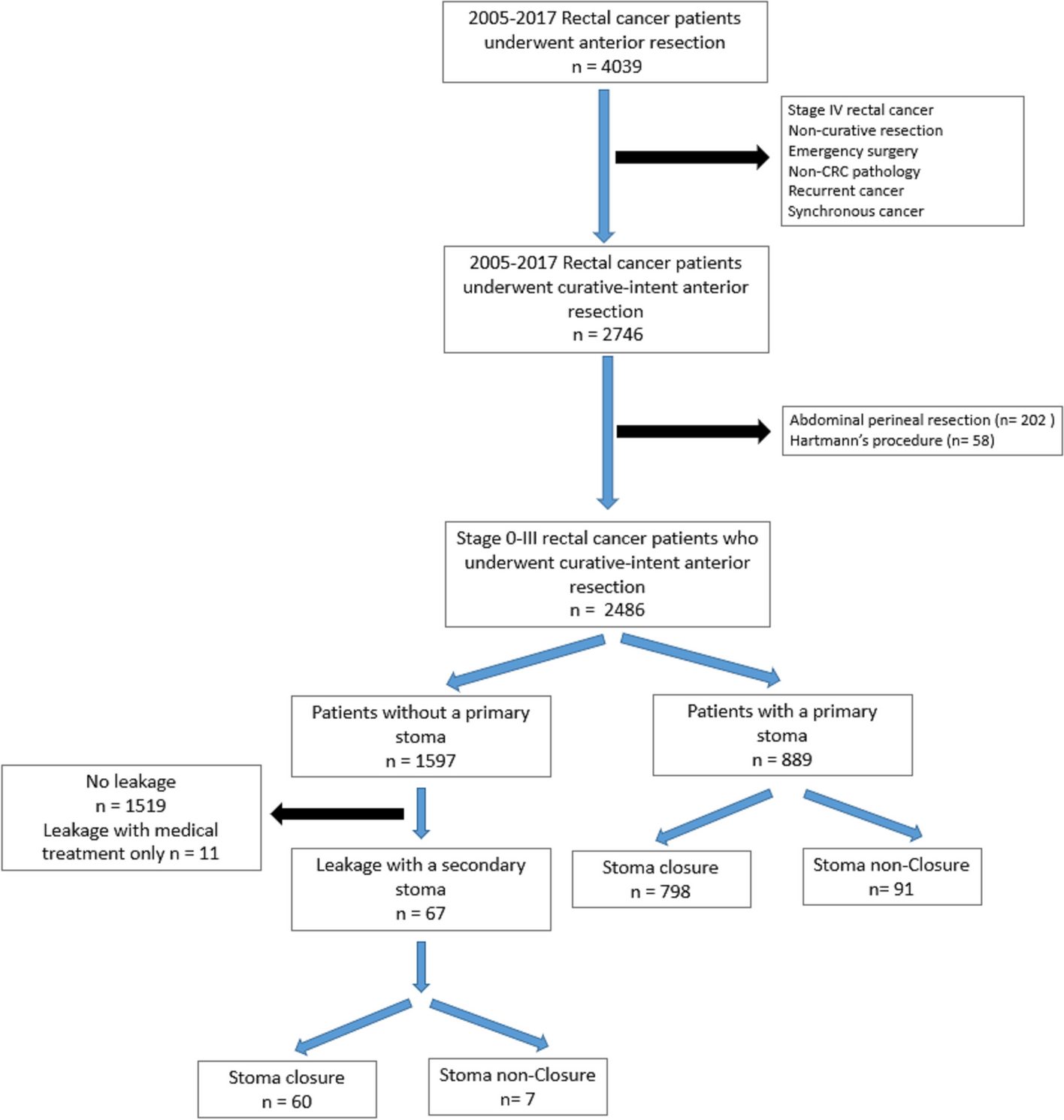
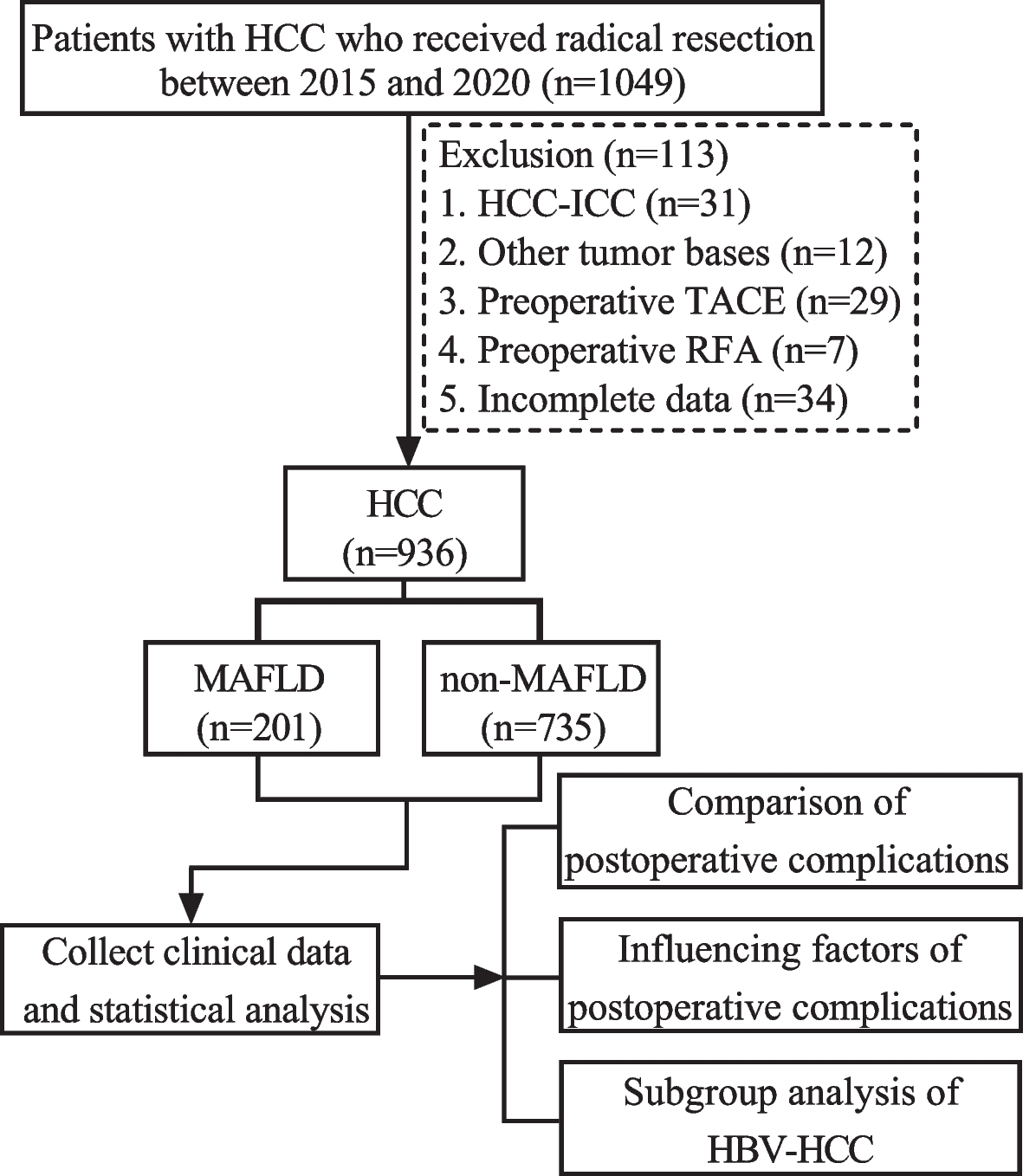
The study cohort was selected and depicted in Fig. 1. A total of 936 HCC patients who underwent radical resection were enrolled in this study, comprising of 764 (81.6%) males and 172 (18.4%) females. Among the study population, the median age of patients was 57 (48.0–64.0) years, BMI ≥ 23 kg/m2 was observed in 477 (51.0%) patients. The prevalence of T2DM, MD, excessive alcohol consumption and HBsAg-positivity were 140 (15.0%), 324 (34.6%), 103 (11.0%), and 853 (91.1%) patients, respectively. Additionally, the median tumor diameter measured 4.0 (2.7–6.4) cm. The majority of these tumors were solitary, accounting for 87.4% (818/936) (Table 1).
Fig. 1
Flow chart for the selection of the study population
Table 1 Baseline characteristics of HCC patientsThe HCC patients were classified into the MAFLD group (201, 21.5%) and the non-MAFLD group (735, 78.5%) based on the presence or absence of MAFLD. In comparison to the non-MAFLD group, the MAFLD group exhibited a higher median BMI (24.2 vs 22.3 kg/m2, P < 0.001) and a greater proportion of patients with combined BMI ≥ 23 kg/m2 (78.6% vs 43.4%, P < 0.001). Moreover, the prevalence rates of T2DM and MD in the MAFLD group were significantly higher compared to the non-MAFLD group (27.9% vs 11.4%, P < 0.001; 50.2% vs 30.4%, P < 0.001; respectively). Additionally, the ALT levels were also significantly higher in the MAFLD group compared to the non-MAFLD group (36.0 vs 32 IU/L, P = 0.012). No significant differences were observed between both groups in terms of other characteristics (all P > 0.05) (Table 1).
Complications after radical resection in HCC patientsThe overall morbidity rate of complications after radical resection in HCC patients was 21.0% (197/936). Classification of postoperative complications according to CCI: CCI (8.7–20.8) 49 (5.2%) patients, CCI (20.9–26.1) 67 (7.2%) patients, CCI (26.2–33.6) 26 (2.7%) patients, CCI (33.7–42.3) 18 (1.9%) patients, CCI (42.4–46.1) 16 (1.7%) patients, and CCI (46.2–100) 22 (2.4%) patients. Additionally, major complications (CCI ≥ 26.2) occurred in 80 (8.5%) patients (Tables 2 and 3).
Table 2 Incidence of postoperative complications in HCC patientsTable 3 CCI classification of postoperative complications in HCC patientsThe overall incidence of postoperative complications in the MAFLD group was higher compared to the non-MAFLD group (27.4% vs 19.3%, P = 0.013). Moreover, the MAFLD group exhibited a higher occurrence of postoperative infectious and major complications (CCI ≥ 26.2) compared to the non-MAFLD group (23.4% vs 13.5%, P = 0.001; 12.4% vs 7.5%, P = 0.026, respectively). Further analysis found that the MAFLD group exhibited a higher incidence of postoperative complications, including pleural effusion, intra-abdominal infection, liver failure, wound infection, and death within 30 days (all P < 0.05). However, there were no statistically significant differences observed in other complications between the two groups (Table 4).
Table 4 Comparison of complications between MAFLD group and non-MAFLD groupInfluencing factors of complications after radical resection in HCC patientsUnivariate logistic regression analysis found that MAFLD was identified as a significant risk factor of complications after radical resection in HCC patients (OR 1.573, 95%CI 1.097–2.255, P = 0.014). Additionally, age ≥ 60 years, male, T2MD, tumor diameter ≥ 5 cm, number of tumors ≥ 2, MVI, Child–Pugh grade B and open surgery were significantly associated with post-hepatectomy complications in HCC patients (all P < 0.05) (Table 5).
Table 5 Univariate and multivariate analysis of complications after radical resection in HCC patientsMultivariate logistic regression analysis revealed that MAFLD was an independent risk factor of complications after radical resection in HCC patients (OR 1.565, 95%CI 1.109–2.343, P = 0.012). Additionally, age ≥ 60 years, number of tumors ≥ 2, MVI, Child–Pugh grade B and open surgery were also identified as significant independent risk factors of post-hepatectomy complications (all P < 0.05) (Table 5).
Influencing factors of infectious complications after radical resection in HCC patientsUnivariate logistic regression analysis found that MAFLD was identified as a risk factor of complications after radical resection in HCC patients (OR 1.961, 95%CI 1.328–2.894, P = 0.001). Additionally, age ≥ 60 years, T2MD, HBV DNA ≥ 500 IU/mL, tumor diameter ≥ 5 cm, tumor number ≥ 2, MVI, Child–Pugh grade B and open surgery were also found to be associated with an increased risk of infectious complications after radical resection in HCC patients (all P < 0.05) (Table 6).
Table 6 Univariate and multivariate analysis of infectious complications after radical resection in HCC patientsMultivariate logistic regression analysis showed that MAFLD was an independent risk factor of infectious complications after radical resection in HCC patients (OR 2.092, 95%CI 1.386–3.156, P < 0.001). The other independent risk factors included: age ≥ 60 years, HBV DNA ≥ 500 IU/mL, tumor diameter ≥ 2, MVI, Child–Pugh grade B and open surgery (all P < 0.05) (Table 6).
Influencing factors of major complications after radical resection in HCC patientsUnivariate logistic regression analysis found that MAFLD was a risk factor of major complications (CCI ≥ 26.2) after radical resection in HCC patients (OR 1.756, 95%CI 1.064–2.898, P = 0.028). Additionally, age ≥ 60 years, BMI ≥ 23 kg/m2, T2DM, tumor diameter ≥ 5 cm, MVI, Child–Pugh grade B and open surgery were also found to be associated with an increased risk of major complications after radical resection in HCC patients (all P < 0.05) (Table 7).
Table 7 Univariate and multivariate analysis of major complications after radical resection in HCC patientsMultivariate logistic regression analysis revealed that MAFLD independently increased the risk of major complications after radical resection in HCC patients (OR 1.859, 95% CI 1.106–3.124, P = 0.019). The other independent risk factors included: age ≥ 60 years, tumor diameter ≥ 5 cm, Child–Pugh grade B and open surgery (all P < 0.05) (Table 7).
Subgroup analysis of HBV-HCCHBV-HCC subgroup was analyzed due to the fact that 91.1% (853/936) HCC were diagnosed with HBV-HCC. The HBV-HCC patients were aged 57 years (49.0–64.0 years), including 698 males (81.8%) and 155 females (18.2%). The proportion of patients with BMI ≥ 23 kg/m2, T2DM, and MD were 51.1% (436), 14.1% (120), and 34.1% (291) respectively. They were divided into two groups based on the presence or absence of MAFLD: 178 (20.9%) patients in the MAFLD group and 675 (79.1%) patients in the non-MAFLD group. The baseline characteristics of patients in the HBV-HCC subgroup and the comparison of baseline characteristics between the MAFLD group and the non-MAFLD group were presented in Table 8.
Table 8 Baseline characteristics of patients with HBV-HCC subgroupComplications after radical resection in the subgroup of HBV-HCC patientsThe overall morbidity rate of complications after radical resection in HBV-HCC patients was 20.9% (178/853). Classification of postoperative complications according to CCI: CCI (8.7–20.8) 44 (5.2%) patients, CCI (20.9–26.1) 63 (7.4%) patients, CCI (26.2–33.6) 21 (2.5%) patients, CCI (33.7–42.3) 15 (1.8%) patients, CCI (42.4–46.1) 15 (1.8%) patients, and CCI (46.2–100) 20 (2.3%) patients. Additionally, major complications (CCI ≥ 26.2) occurred in 69 (8.1%) patients (Tables 9 and 10).
Table 9 Incidence of postoperative complications in HBV-HCC patientsTable 10 CCI classification of postoperative complications in HBV-HCC patientsThe incidence of postoperative complications in the MAFLD group was higher compared to the non-MAFLD group (P = 0.08). Moreover, the MAFLD group also exhibited a higher occurrence of infectious and major complications (CCI ≥ 26.2) compared to the non-MAFLD group (all P < 0.05) (Table 11).
Table 11 Comparison of complications between MAFLD group and non-MAFLD groupIn order to further elucidate the impact of different subtypes of MAFLD on post-hepatectomy complications in patients with HBV-HCC, they were divided into two groups based on their BMI: lean MAFLD group (BMI < 23 kg/m2) (38, 21.3%) and non-lean MAFLD group (BMI ≥ 23 kg/m2) (140, 78.7%). However, the incidence of complications, infectious and major complications did not show any statistically significant difference between these two groups (34.2% vs 26.4%, P = 0.344; 34.2% vs 22.1%, P = 0.126; 15.8% vs 10.7%, P = 0.390; respectively). According to the presence or absence of T2DM, the patients with MAFLD were divided into two groups: T2DM-MAFLD group (46, 25.8%) and non-T2DM-MAFLD group (132, 74.2%). The incidence of complications, infectious and major complications in the T2DM-MAFLD group was significantly higher compared to the non-T2DM-MAFLD group (52.2% vs 19.7%, P < 0.001; 47.8% vs 16.7%, P < 0.001; 26.1% vs 6.8%, P < 0.001; respectively). According to the presence or absence of MD, the patients with MAFLD were divided into two groups: MD-MAFLD group (90, 50.6%) and non-MD-MAFLD group (88, 49.4%). The incidence of complications, including infectious and major complications, appeared to be higher in the MD-MAFLD group compared to the non-MD-MAFLD group, however, these differences did not reach statistical significance (33.3% vs 22.7%, P = 0.115; 30.0% vs 19.3%, P = 0.099; 12.2% vs 11.4%, P = 0. 859; respectively).
Influencing factors of complications after radical resection in the subgroup of HBV-HCC patientsUnivariate logistic regression analysis found that MAFLD was a risk factor for complications after radical resection in HBV-HCC patients ((OR 1.669, 95%CI 1.142–2.439, P = 0.008). Multivariate logistic regression analysis showed that MAFLD was an independent risk factor for complications after radical resection in HBV-HCC patients (OR 1.674, 95%CI 1.127–2.487, P = 0.011) (Fig. 2). In addition, we also analyzed the influencing factors of infectious and major complications after radical resection in HBV-HCC patients. We also found that MAFLD was an independent risk factor for infectious and major complications after radical resection in HBV-HCC patients (OR 2.111, 95%CI 1.375–3.241, P = 0.001; OR 1.770, 95% CI 1.006–3.116, P = 0.048; respectively) (Figs. 3 and 4).
Fig. 2
Influencing factors of complications after HBV-HCC hepatectomy
Fig. 3
Influencing factors of infectious complications after HBV-HCC hepatectomy
Fig. 4
Influencing factors of major complications after HBV-HCC hepatectomy
留言 (0)