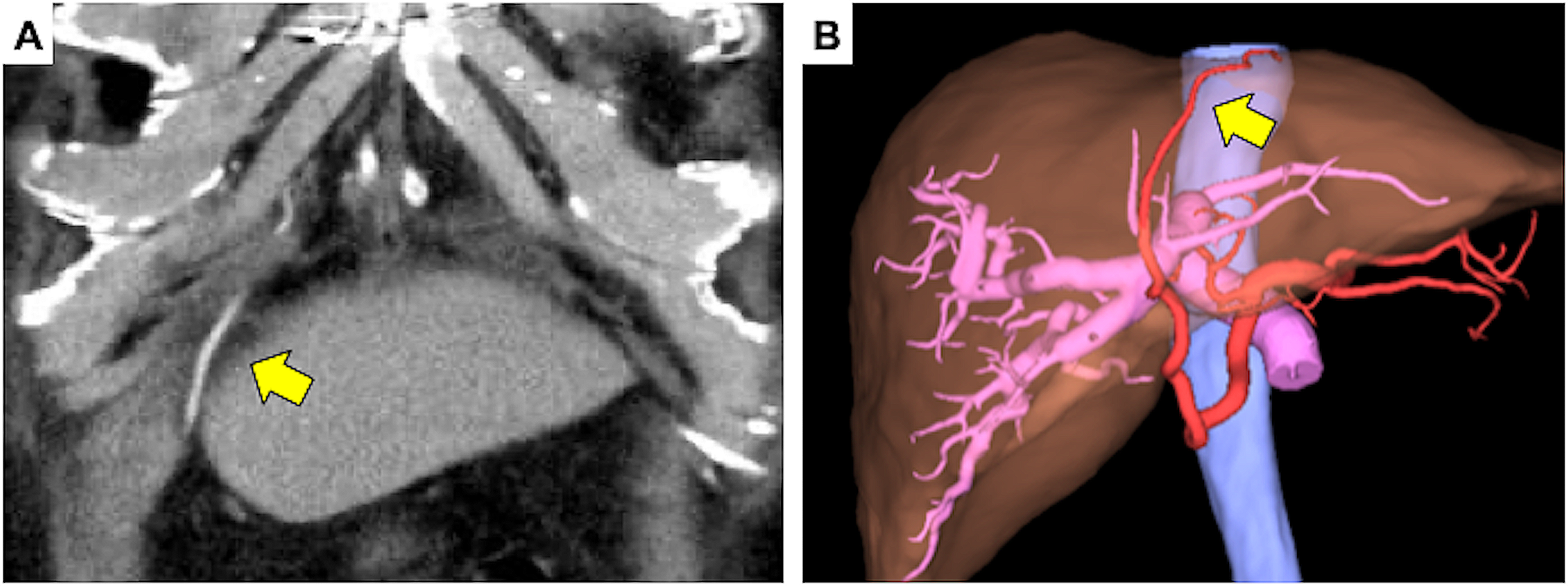
RGEA grafts are excellent conduits for coronary revascularization, similar to the internal thoracic artery. Long-term patency of RGEA grafts as conduits for CABG has also been reported [1, 2, 7]. The RGEA is currently used as a bypass graft for posterior coronary circulation. However, CABG using RGEA is not often performed. In the presented case, the right coronary artery exhibited significant stenosis (99% occlusion). Additionally, the ascending aorta’s condition was deemed suboptimal. To minimize manipulation of the ascending aorta and considering the patient’s atherosclerosis obliterans in the lower limbs and diabetes mellitus, conserving the saphenous vein was a prudent decision. The patient’s lower limb wounds might be challenging to heal, necessitating the retention of the saphenous vein in anticipation of potential future arterial bypass requirements due to the progression of arteriosclerosis obliterans. For these reasons, the RGEA graft was used. Graft injuries during abdominal surgery after CABG using the RGEA may cause coronary failure and fatal arrhythmia. To avoid graft injury, it is important to understand how to harvest and place the graft in CABGs. There are two possible routes for RGEA grafting: ante-gastric and retro-gastric. Most cardiac surgeons employ the ante-gastric route because it allows easier identification of bleeding from the RGEA pedicle. In this case, the graft traversed the ventral side of the stomach, proceeded to the left side of the hepatic falciform ligament via the liver’s ventral surface, and reached the heart through an opening in the diaphragm (Fig. 1).
During laparotomy, the RGEA frequently adheres to the abdominal wall, hepatic falciform ligament, and liver surface. In the present case, it adhered to the liver surface adjacent to the hepatic falciform ligament. Because of the adhesion of the graft to the hepatic dissection line, we were forced to remove the graft from the hepatic surface, but we were able to do so without damaging the graft. Fortunately, no electrocardiographic changes were observed during the dissection or taping. However, spasms and injuries induced by graft handling during surgery can cause critical coronary failure [3]. To avoid inadvertent graft injury, in addition to perioperative management with anticoagulation therapy, an understanding of the graft route and careful and conservative surgical manipulation are necessary.
Various reports on abdominal surgery after CABG with the RGEA have been published. The following is a summary of the points to be considered for each surgery. Sakamoto et al. reported that in laparoscopic cholecystectomy, during dissection of Calot’s triangle, it is necessary to ensure that the pedicle is not stretched, and it is important to use a lower pneumoperitoneal pressure (such as 5 mmHg). In laparoscopic colectomy, it has also been reported that care should be taken to avoid the possibility of unexpected excessive stress on the RGEA graft due to positional changes [8, 9]. Although gastrectomy is most frequently reported, the RGEA graft may be resected, and a replacement graft may be used from the viewpoint of the lymph node dissection. However, in cases such as early stage cancer, there is little metastasis to the lymph nodes, and RGEA resection should be performed with caution [3]. There are reports that pancreaticoduodenectomy allows grafts to be left in place [5], and there are also reports of preoperative reconstruction of a replacement graft [6, 10]. Hepatic resection is more variable depending on the site of resection; however, more caution is required for left lobectomy because the graft often runs over the anterior aspect of the left lobe [11]. The two-stage explantation method has been reported to be effective in preserving RGEA grafts during transplantation [12]. There have also been reports of a backup system for cardiovascular surgery and the placement of a sheath in the femoral artery for quick response [3]. Moreover, a recent report showed that real-time vessel navigation using indocyanine green fluorescence (ICG) and visualization of the RGEA graft is useful for easy identification [13].
In this case, the left hepatic coronary mesentery was not dissected, but the RGEA was in traction, as the left lobe of the liver fell into the space after right lobectomy. Therefore, the falciform ligament was anchored to the abdominal wall to prevent tension. Laparoscopic surgery has increased in recent years and can be performed in the left semi-supine position. In such situations, it is essential to verify the condition of the RGEA graft with the patient in a supine position. Furthermore, securing it to the abdominal wall is crucial for preventing complications associated with RGEA grafts. In the future, with the increasing number of patients with metabolic syndrome, particularly hyperlipidemia, the likelihood of performing abdominal surgery after CABG using RGEA grafts, as in our case, is expected to increase. Gaining a thorough understanding of the preoperative anatomy and being cognizant of the pitfalls and innovations in each surgical procedure are paramount.






留言 (0)