General considerations
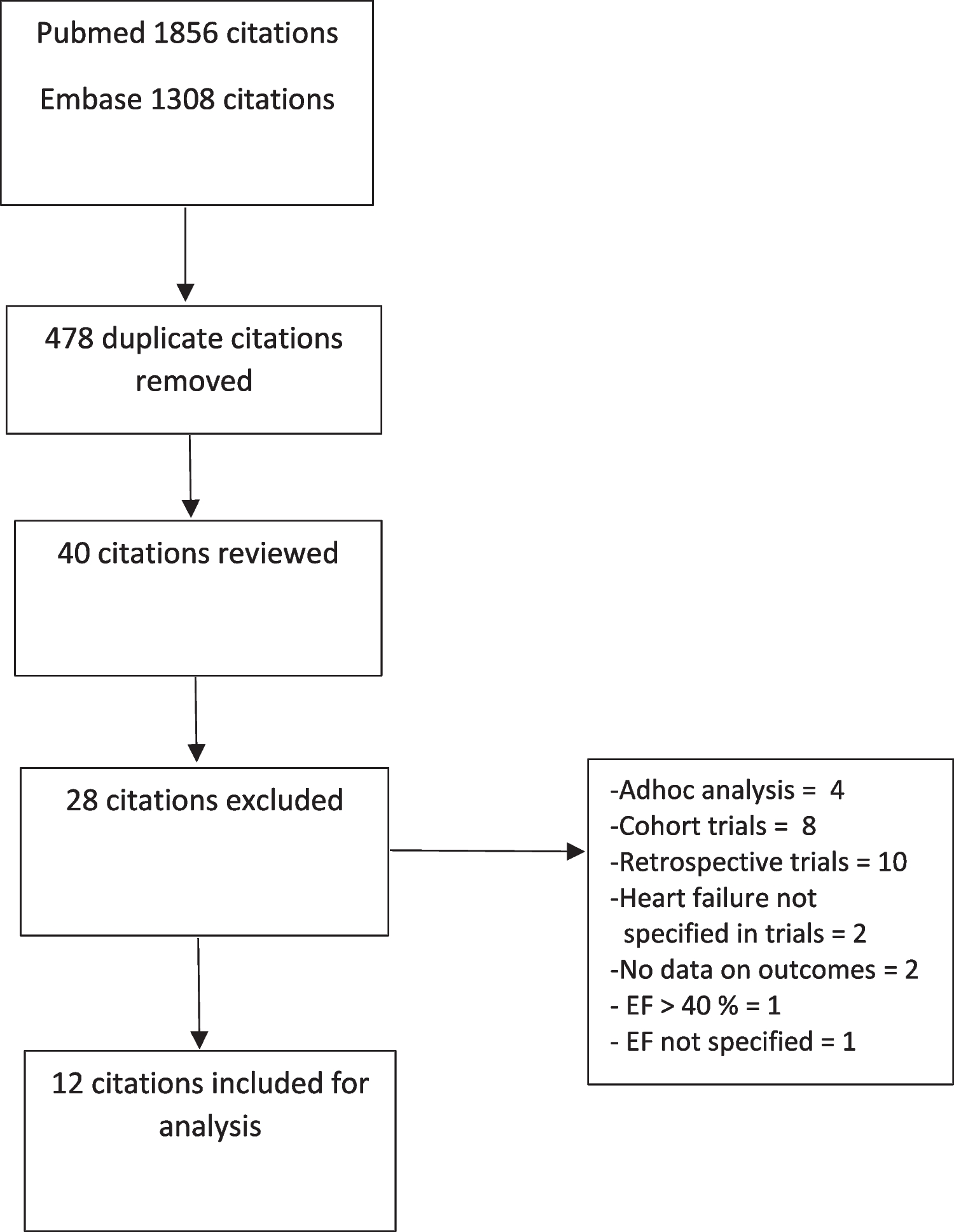
In our study, we enrolled 100 patients electively admitted to hospital. We investigated the application of a switching algorithm designed according to current requirements. This algorithm was divided into six successive steps. To apply the switching algorithm in routine care to an outpatient medication, we, first, collected all relevant information on outpatient medications via a medication reconciliation. The patient interview by the pharmacist proved to be the richest source for compiling the required information. The algorithm, however, could not be used for around a quarter of the identified medications due to missing patient-related information on the respective outpatient medications.
Before applying the switching algorithm, second, a medication review conducted by a pharmacist identified and resolved several drug-related problems. We focused on drug-drug interactions and potentially inappropriate medications while assessing drug-related problems. Of the 10 most frequently prescribed outpatient medications, only 2 were not listed in the hospital formulary. For those products which were not listed in the hospital formulary, most switches could be performed by using the standardized algorithm, with generic switching being the most common. Only rarely, an individual decision had to be made if no standardized switching to the hospital formulary was possible after the previous steps of the algorithm.
Since recommendations were issued to the wards as an order template, switching recommendations within this project were actually implemented in routine practice.
Medication reconciliation including a patient interview
For around a quarter, the information regarding product name and strength was not complete in our study. Therefore, switching could not be performed on the basis of the algorithm. In this case, time-consuming research would have been necessary to complete the patient- and medication-related information, or the concerning medication would have had to be discontinued during hospital stay without therapeutic justification. This shows that a consideration of the switching algorithm alone is not sufficient. The completeness of the required patient- and medication-related information should also be the subject of investigations. In this context, the patient interview by pharmacists contributed significantly to information completion according to our data.
We enrolled patients who were mainly admitted to the Urology Department. This indicates, at first glance, a fairly specific patient collective. At second glance, as the average age shows, we enrolled patients at an advanced age. It was, therefore, likely that our patients were additionally affected by several diseases of internal medicine. The top list of medications supports this assumption and nevertheless makes the results generalizable to other patients of elective hospital admission.
The pharmacist-led patient interview proved to be helpful in recognizing the requested information needs. In 64% of the patients, the drug information required for switching was compiled mainly by the patient interview.
Our results regarding the positive evaluation of the pharmaceutical patient interview are confirmed in the literature: For example, as reported in [22], the recording of medication use by means of patient interviews appears to be essential in identifying drug-related problems. By this, also self-medications can be considered for switching in principle. As a principle rule, however, we did not transfer self-medication to the hospital formulary or ordered those medications. In this context, we defined self-medication in the sense that a medication was taken by patients themselves without a physician’s prescription. Patients were instructed not to self-medicate during their hospital stay. Non-prescription medications, in contrast, which were prescribed by a physician, were switched.
Medication review
The evidence for medication reviews in the literature is very clear, as a recent Cochrane review [23] underlines. In adult hospitalized patients, medication reviews probably decrease the number of hospital readmissions and emergency department visits. Little to no effect was shown, however, on mortality [23]. The effect on health-related quality of life is described as very uncertain [23]. This is confirmed by another review [24] reporting that an isolated medication review during a short intervention period had effects on most medication-related outcomes. In contrast, minimal effects on clinical outcomes and no effects on quality of life were described by the same authors [24].
In our study, performing a medication review before applying the switching algorithm could be an essential step in optimizing drug safety. In our study, we have shown that drug-drug interactions occurred in 39% of those 79 patients who had more than one continuous medication. Potentially inappropriate medications (PIMs) were found in 16% of those 73 patients who were 65 years or older. However, in this study, we found that only one recommendation actually brought about a change—i.e., avoidance of drug-drug interactions concerning omeprazole by switching to pantoprazole.
Although various professional groups as well as nursing services have been involved in medication reviews [25], the involvement of a pharmacist in medication reviews in particular is frequently mentioned in the literature [26]. However, the focus here is more on discharge [27] and measures to reduce (re-)admission to hospital [28]. With regard to interfaces, medication reviews in outpatient care [29] and offered by community pharmacies [30] have also been examined. However, reviews on admission as reported by us in this work are comparatively rare, especially when they are associated with a consecutive medication switching. Although it can certainly be assumed that this is a routine measure in many hospitals, the number of published scientific studies as ours is comparatively low.
Algorithm-based outpatient medication switching
So far, the literature has mainly reported on therapeutically induced medication switching [31]. In recent years, however, quality assurance measures such as standardized switching by pharmacists and electronic prescribing aids have been implemented for switching induced through legal and economic reasons. Those strategies, however, were mainly implemented in university hospital settings. Therefore, we performed our study in a non-university setting addressing a standardized quality-assured switching. By this, we aimed to decrease follow-up costs due to a reduced number of expensive individual prescriptions.
An algorithm similar to that used in our study was applied to the medication schedules of 120 patients [9]. In this study, 774 medications prescribed at the time of their admission to a surgical department were assessed. However, in contrast to our study, which was conducted prospectively, the study in [9] was conducted retrospectively. We also included a wider range of electively admitted patients with a focus on urology. Furthermore, our study did not take place in a university hospital, which is often subject to special conditions in the context of maximum care that are not always transferable to other hospitals. In [9], 52.8% of the prescribed medications were included in the hospital formulary so that switching was not necessary. In contrast, only 18.5% were included in our hospital formulary. This shows the considerable difference of our data to a university hospital with a much more comprehensive hospital formulary.
In [9], 84.7% of the remaining medications were successfully switched to a corresponding generic medication and 10.2% to a therapeutic equivalent. In our study, 42.0% were a generic switching, while switching to a therapeutic alternative was recommended in 1.7% only. Even if the design of the algorithm cannot be compared one-to-one, the relative orders are largely consistent indicating that generic switching is usually possible and switching to a therapeutically equivalent is in comparison only rarely required.
The authors in [9] reported that for only 2.3% of the active substances no specific switching procedures were found according to the algorithm. In those cases, the medications were either discontinued or specific medication classes, current illnesses, or co-medication required manual switching as reported by the authors in [9]. What is more, only some medications were continued unswitched and ordered with a wholesaler. In our study, only for 0.4% a patient-individual switching had to be recommended by the pharmacist. Finally, 8.2% of outpatient medications still had to be ordered with wholesalers in our study.
It is also interesting to note that we succeeded in switching a total of 23 combination products in our study. Such products are very common in the outpatient sector and are intended to optimize adherence due to the small number of medications. Among the ten most frequently prescribed outpatient medicines, there were only two that were not included in the corresponding form listed in the hospital formulary. This shows that the significance of switching in the context of combination products is currently limited and that a simple switching to the hospital formulary is usually not a problem.
Limitations
The algorithm was designed to structure and standardize the frequently rather subjective switching on the ward. In this way, the bias in this area decreased by the study concept in principle. A bias in this study may nevertheless lie in the fact that this study focused on electively admitted patients. In particular, the data basis from the study was comparatively better than for non-elective admissions, for example, admitted to the central emergency department. The following additional limitations have to be considered while drawing conclusions for an international setting from our results: In many patients, the patient- and medication-related information for a systematic switching according to the algorithm was not available in spite of a sophisticated medication reconciliation. Our non-university inhouse setting was a very specific hospital with apparently a very short list of available medicines in the hospital formulary. Last but not least, the general setting in Germany is a specific healthcare system driven by rebate contracts and strictly separate outpatient and inpatient sectors.






留言 (0)