
記住我
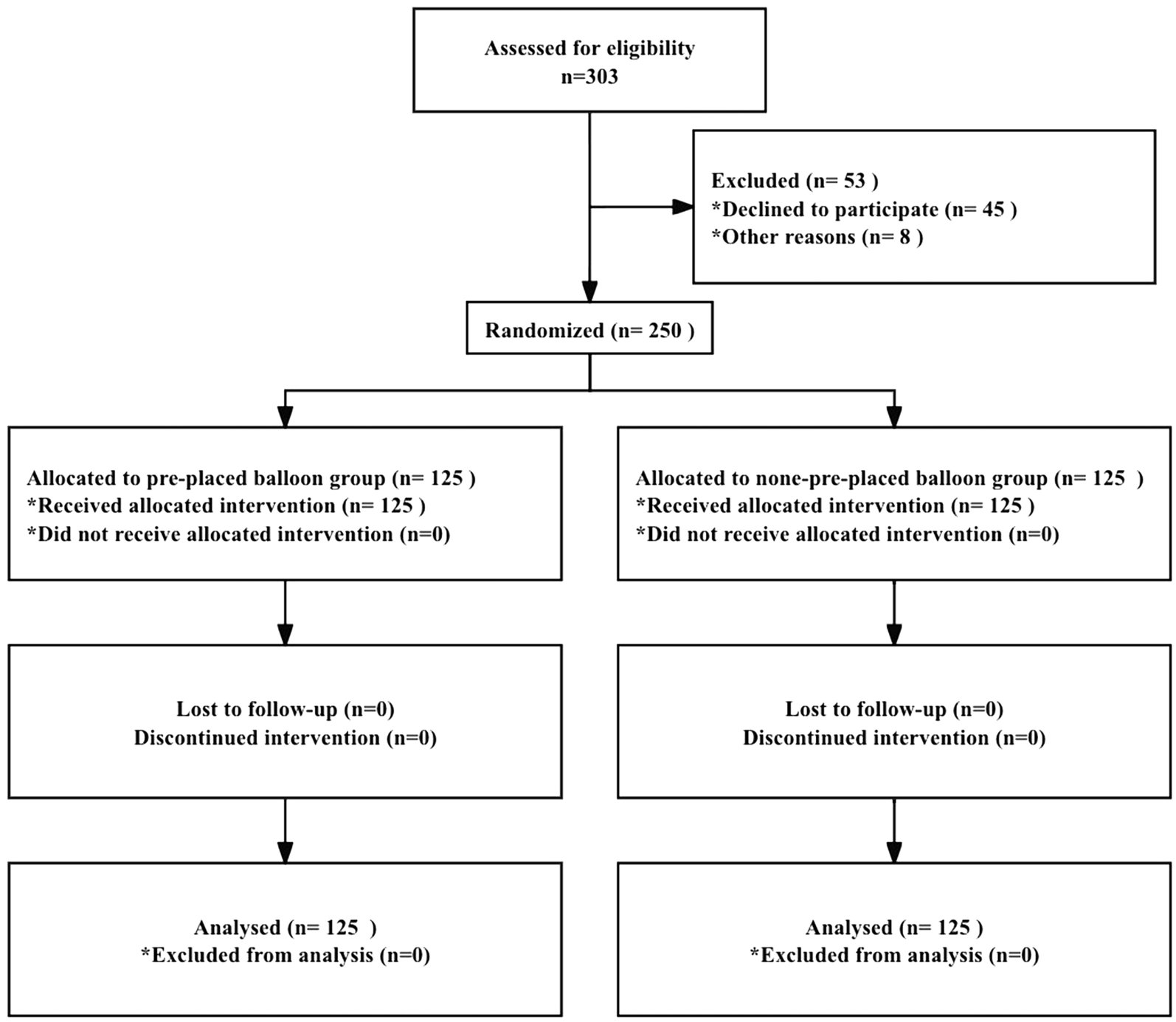
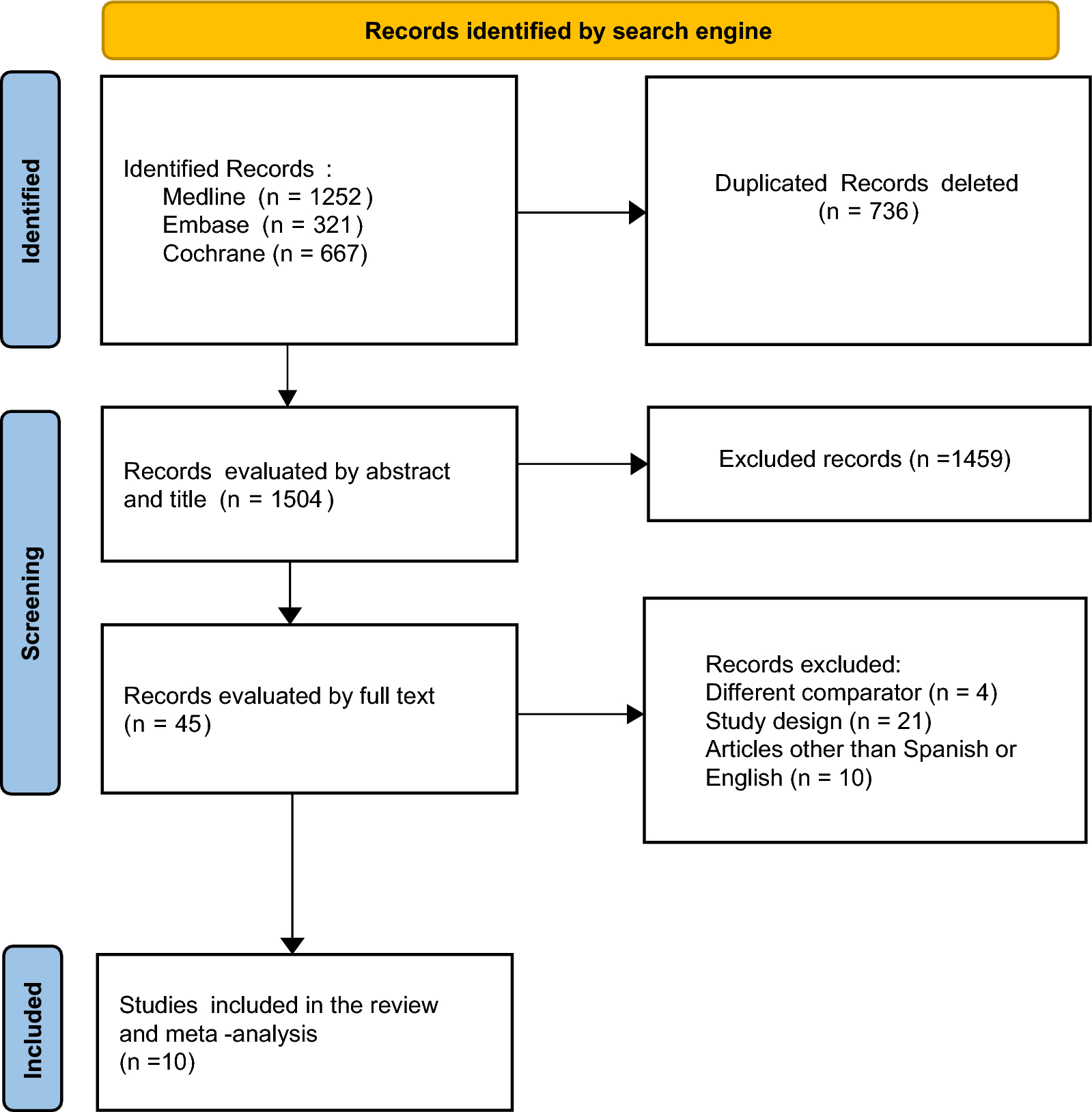
Four electronic databases searches yielded a total of 1933 records from inception to January 2023. After removing duplicates, 975 records were screened based on their titles and abstracts. The initial screening identified 338 potentially relevant studies evaluated against eligibility criteria. A total of 321 articles were deemed ineligible after thoroughly examining of their full text due to non-compliance with the established eligibility criteria. Ultimately, a total of 17 SRs with or without a meta-analysis on ECMO were included for systematic scoping review and evidence synthesis [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38]. Figure 1 displays all comprehensive review processes, exclusion numbers, and reasons for full-text exclusions.
Fig. 1
Flow diagram of the literature reviewing process and results
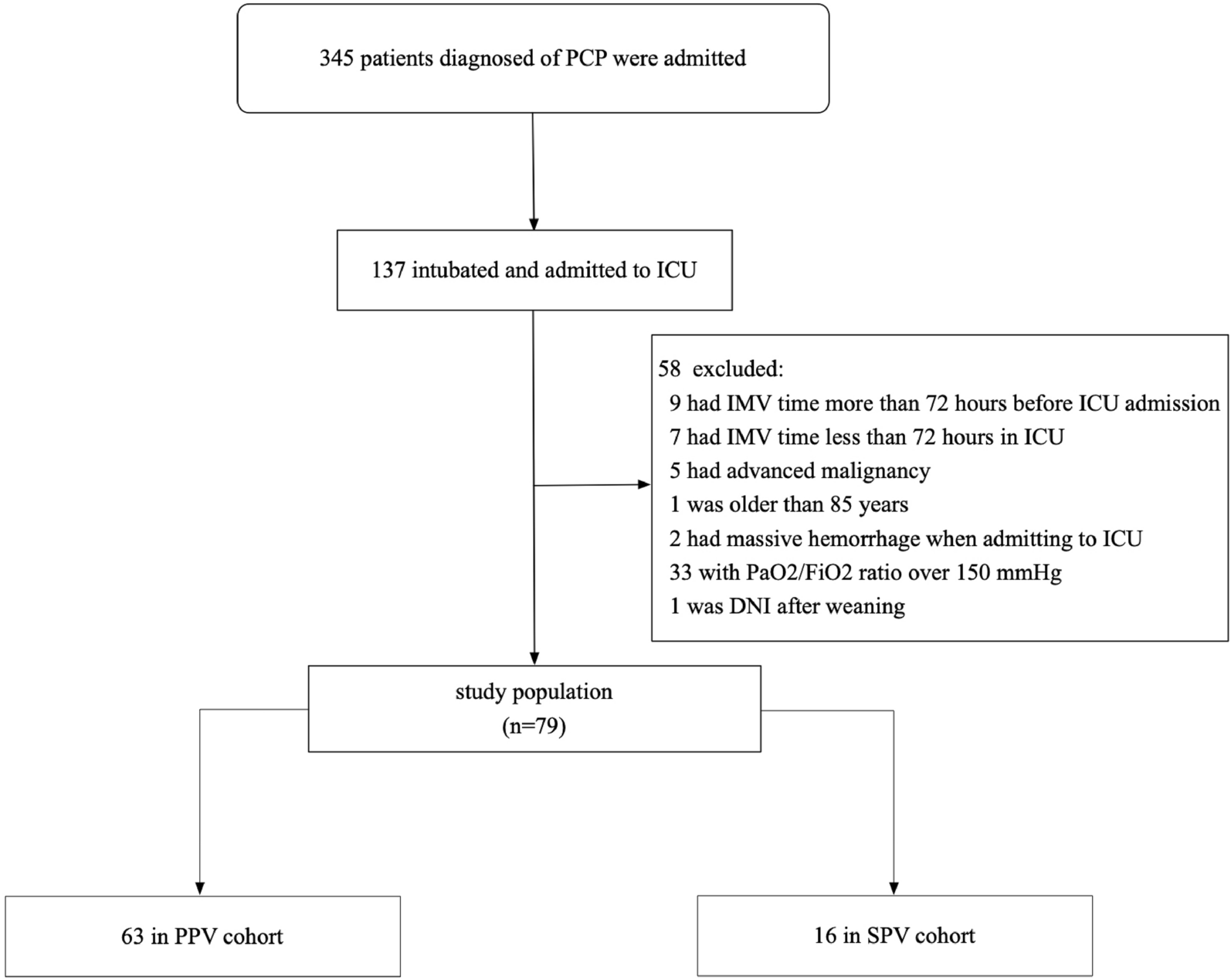
Characteristics of included SRsAnnual trends in publicationsThe correlation between the number of studies and the year of publication was plotted to visualize the trend of ECMO studies published over time. SRs on ECMO first appeared in 2010, although our search began with databases construction. Nonetheless, there has been a worldwide increase in ECMO literature, with a peak in 2020, that likely due to the COVID-19 pandemic. Figure 2 depicts the trend in publication of research studies.
Fig. 2
Annual trends in publications of SRs on ECMO
Geographical distributionSRs exhibited variation in their country of origin, with the greatest frequency being observed for Canada [24, 27, 28, 31, 34] (n = 5). Other nations represented were the United States [22, 33, 35, 38] (n = 4), Italy [23, 37] (n = 2), China [36] (n = 1), Brazil [30] (n = 1), France [32] (n = 1), Korea [25] (n = 1), Netherlands [26] (n = 1), and United Kingdom [29] (n = 1).
Primary studies and participantsThe number of studies included for ECMO ranged from 2 to 75, with an average of 14. Ten SRs contained fewer than 10 ECMO-related primary studies, five SRs included 10 to 25 primary studies, and two SRs contained more than 25 primary studies. Three SRs only included the type of randomized controlled trial (RCT), seven SRs included RCT and other study types, and seven SRs were limited to study categories other than RCT. The range of participants included in SRs was 429 to 38,160, averaging 5168. The majority of SRs (n = 12) included more than 1000 participants. There was a wide variety of clinical topics in the included SRs, including acute respiratory distress syndrome (ARDS) [31] (n = 1), dependent ARDS [38] (n = 1), severe ARDS [27, 30, 32, 36] (n = 4), acute respiratory failure (ARF) [24] (n = 1), ARF due to H1N1 influenza pandemic [22] (n = 1), acute lung injury (ALI) due to H1N1 influenza infection [23] (n = 1), acute liver failure (ALF) or acute on chronic liver failure (ACLF) [34] (n = 1), cardiac arrest [26, 28, 29, 33, 35, 37] (n = 6), and cardiac arrest of cardiac origin [25] (n = 1). The numbers of primary studies and participants are shown in Table 1. Eligibility criteria for SRs varied across studies showed in Table 2.
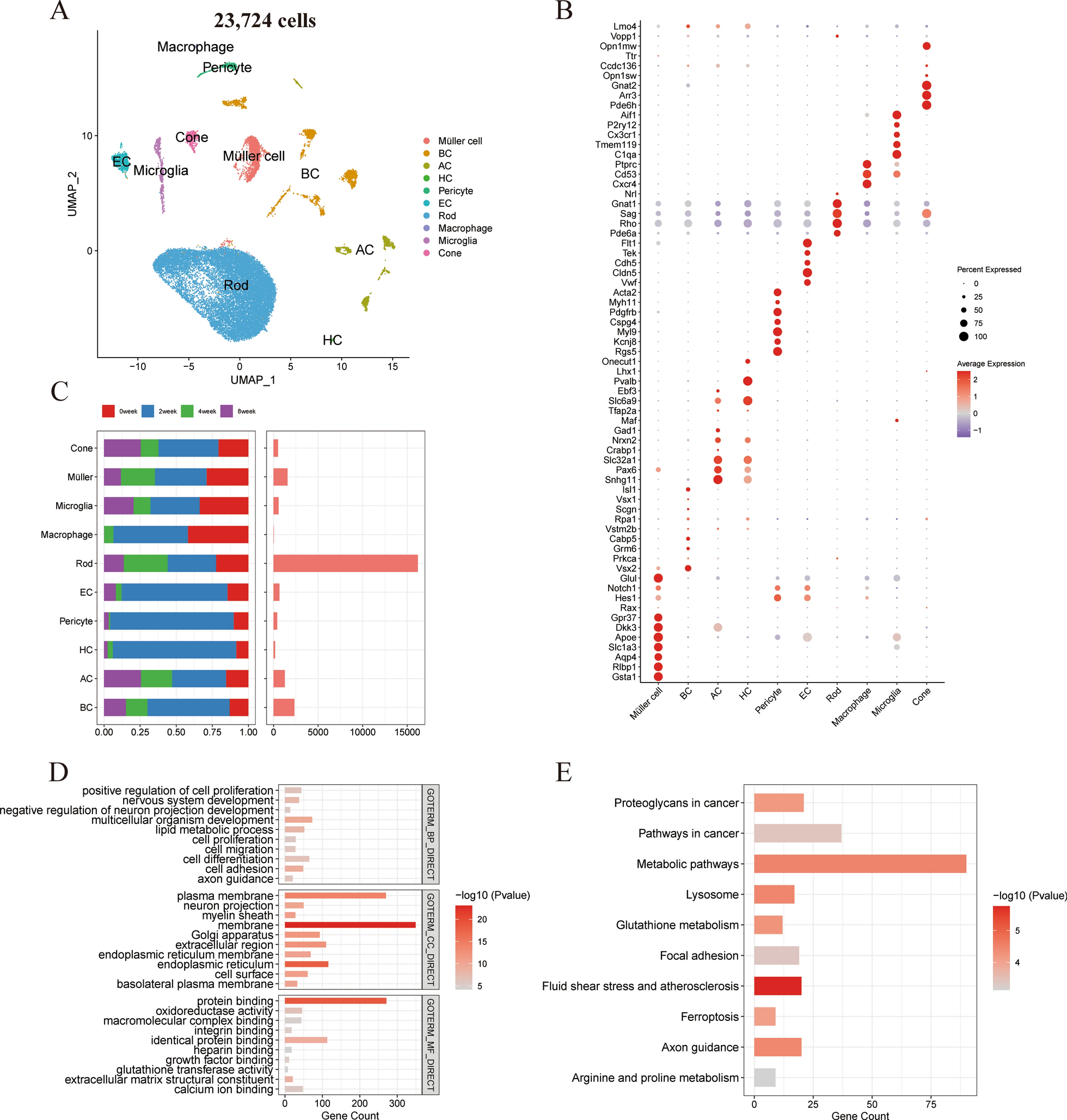
Table 1 Summary of the included SRs of ECMO treatmentTable 2 Eligibility criteria and method of quality appraisal or risk of bias of the included SRsMethodological quality of included SRsIn terms of methodological quality, the overall quality was rated as “Moderate” for six [23, 27, 28, 35,36,37], seven SRs scored “Low” [25, 26, 29, 31,32,33,34], four SRs scored “Critically Low” [22, 24, 30, 38], and “High” for none SRs according to AMSTAR-2 criteria. The most frequent flaws were as follows: lack of a reasonable explanation for the selection of study design type for inclusion, the absence of a report on sources of funding for included studies, a lack of a statement regarding potential sources of conflict of interest, and the absence of a protocol. Figure 3 depicts the methodological quality of the 17 SRs included in the analysis.
Fig. 3
Methodological quality of included SRs
Evidence quality of included SRsThe evidence quality of included one SR was considered high, 5 SRs were moderate and low quality respectively, while 6 SRs were assessed as having very low quality. The results of this evaluation can be found in Table 3.
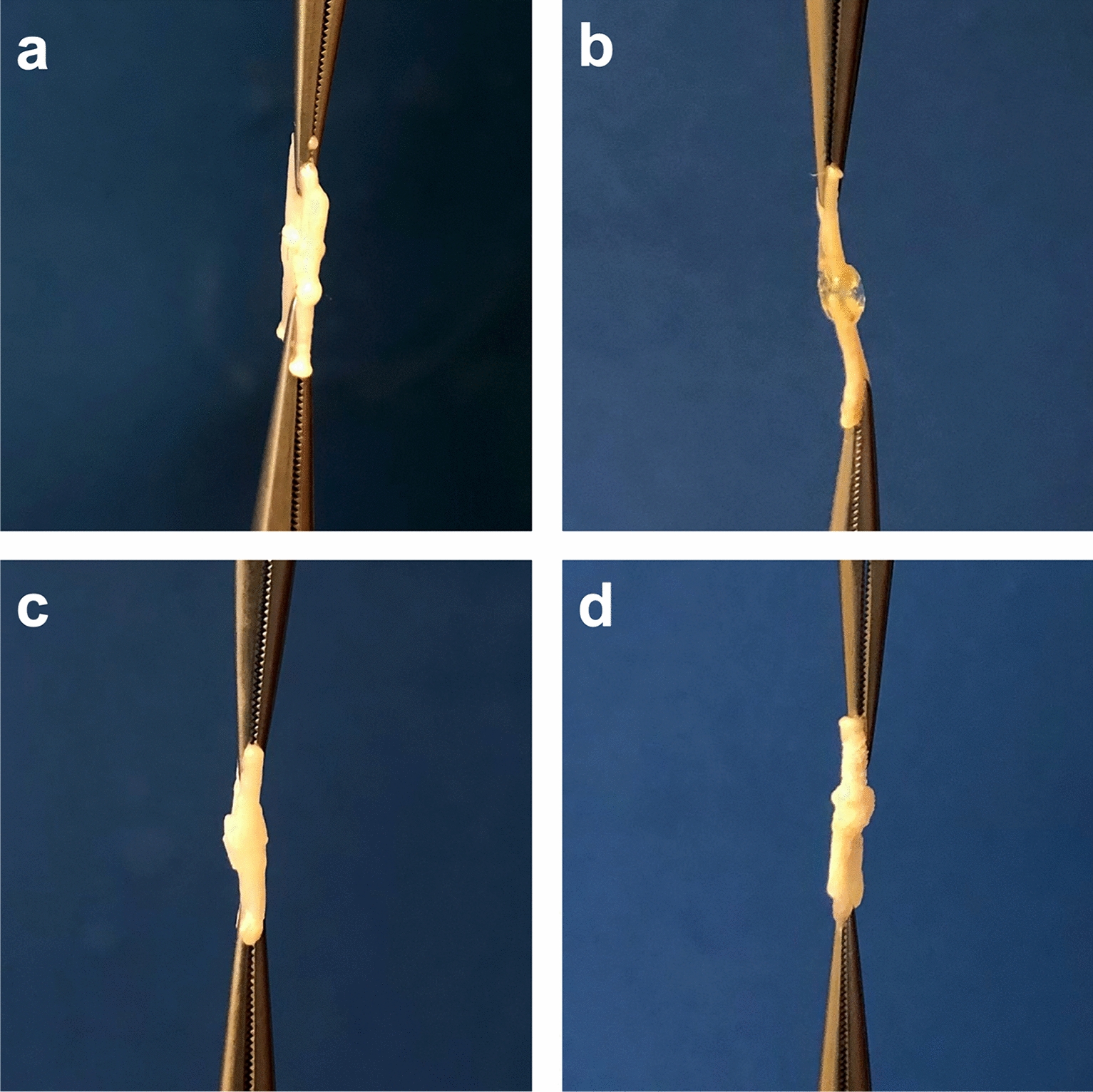
Table 3 Evidence quality of included SRsEvidence mappingFor diseases that overlap, the overall evidence quality was considered. Individual SRs reflected the conclusions, which were confirmed by an internal review. The evidence mapping on ECMO for adults is presented in Fig. 4.
Fig. 4
The evidence mapping on ECMO. X-axis, effect estimate on the certainty of the evidence statement; Y-axis, the number of primary research studies in the selected SR; bubble size, the number of SRs on this topic; bubble color, evidence quality of the findings by GRADE system assessment. ARDS adult respiratory distress syndrome, ALI acute lung injury, H1N1 influenza A, ALF acute liver failure, ACLF acute on chronic liver failure, ARF acute respiratory failure
Evidence of “beneficial” effectThe effects of ECMO, as indicated by statistically significant pooled treatment effects in SRs, were determined based on a substantial number of research studies that included findings on severe ARDS and ALI due to H1N1 influenza infection.
Four SRs [27, 30, 32, 36] evaluated the effects of ECMO on severe ARDS relative to conventional therapy. Among them, one SR [30] with moderate evidence quality was selected as “probably beneficial” on this mapping, suggestive of the probable efficacy of ECMO in severe ARDS; the efficacy of ECMO and severe ARDS in this study was likely linked to reducing mortality, treatment failure, and the need for renal replacement therapy, but longer ICU and hospital lengths of stay. Two SRs [32, 36], including 2 RCTs with moderate or high evidence quality, were selected as “beneficial” on this mapping, suggesting positive support for ECMO in severe ARDS based on 90-day and 30-day mortality outcomes; additionally, there was no difference in device-related adverse events compared to conventional therapy. The remaining SR [27], with low evidence quality, showed an “inconclusive” conclusion in survival to hospital discharge, indicative of weak confidence to support the effectiveness of ECMO. In general, 75% of SRs (comprising 6 RCTs) were classified under the categories of “beneficial” or “probably beneficial”. The overlapping severe ARDS of four SRs was eventually classified as a “beneficial” conclusion considering the overall evidence quality.
A single SR [23] consisting of eight observational studies, which were of low evidence quality, evaluated the impact of ECMO on ALI due to H1N1 influenza infection compared to conventional therapy. Results indicated that ECMO was feasible and effective in patients with ALI due to H1N1 infection; however, subjects with severe comorbidities or multiorgan failure remained at high risk of in-hospital death if prolonged support (more than one week) was required in the majority of cases, which ended in a “beneficial” conclusion.
Evidence of “probably beneficial” effectA considerable number of research studies on clinical topics such as ARDS, ALF or ACLF, and cardiac arrest were used to determine the promising effects of ECMO, as evidenced by statistically significant pooled effects in SRs.
One SR [31], with moderate evidence quality, compared the effects of ECMO on ARDS to conventional therapy, finding that venovenous ECMO in ARDS adults was associated with lower 60-day mortality (relative risk [RR] = 0.73, 95% confidence interval [CI] 0.58–0.92, P = 0.008, I2 = 0%), but also a moderate risk of bleeding.
One SR [34] with moderate evidence quality comparing extracorporeal life support (ECLS) to usual care found that ECLS might decrease mortality (RR = 0.84, [95% CI 0.74–0.96], moderate certainty) and improve hepatic encephalopathy (RR = 0.71, [95% CI 0.60–0.84], low certainty) in patients with ALF or ACLF. The impact of ECLS on hypotension (RR = 1.46, [95% CI 0.98–2.2], low certainty), bleeding (RR = 1.21, [95% CI 0.88–1.66], moderate certainty), thrombocytopenia (RR = 1.62, [95% CI 1.0–2.64], very low certainty) and line infection (RR = 1.92, [95% CI 0.11–33.44], low certainty) was uncertain.
Six SRs on cardiac arrest produced controversial results [26, 28, 29, 33, 35, 37]. Among them, two SRs [26, 37], both low evidence quality, were selected as “beneficial” on this mapping, suggestive of positive support for ECMO in cardiac arrest based on a 30-day survival rate ([95% CI 6–20%], P < 0.001), 30-day favorable neurological outcome ([95% CI 7–20%, P < 0.0001), survival with the favorable neurological outcome at the longest follow-up available (OR = 2.11, [95% CI 1.41–3.15], P < 0.001), survival at the longest follow-up available (OR = 1.40, [95% CI 1.05–1.87], P = 0.02). Three SRs [29, 33, 35] with low, moderate, or very low evidence quality showed a “probably beneficial” conclusion on this mapping, suggesting the probable efficacy of ECMO in cardiac arrest; the efficacy of ECMO and cardiac arrest in these studies was likely associated with improved survival, 30-day and long-term favorable neurological outcome, and long-term neurologically intact survival. The remaining SR [28] of 63 case series and 12 cohort studies concerning out-of-hospital cardiac arrest (OHCA), with very low evidence quality, demonstrated that although a trend toward improved survival with good neurologic outcome was reported in controlled, low-risk of bias cohort studies, a preponderance of low-quality evidence may ascribe an optimistic effect size of extracorporeal cardiopulmonary resuscitation (ECPR) on survival among OHCA patients, rated as “inconclusive” conclusion. On the whole, 83.3% of SRs were classified into “beneficial” or “probably beneficial” categories. For the overlapping cardiac arrest of six SRs, we ultimately rated it as “probably beneficial” conclusion after considering the overall quality of the evidence.
Evidence of “inconclusive” effectThis mapping contained several SRs that provided evidence of the potential inconclusive effect of ECMO in treating clinical topics, including dependent ARDS, ARF, ARF due to the H1N1 influenza pandemic, and cardiac arrest of cardiac origin.
According to one SR [38] with very low evidence quality, 30-day mortality (OR = 0.56, [95% CI 0.37–0.84]) and 90-day mortality (OR = 0.59, [95% CI 0.41–0.85]) were reduced in de
留言 (0)