
記住我




It is a retrospective cohort study. Medical Information Mart for Intensive Care IV (MIMIC-IV) database is a single center data from Beth Israel Deaconess Medical Center which contains information relating to patients admitted to critical care units between 2008 and 2019. The latest version is released at 2023–01–06, with version number v2.2. We used ICD-9 codes (491, 492 or 496), and ICD-10 codes (J41–J44) to defined COPD. Moreover, any of the three COPD codes listed in the primary diagnosis field as AECOPD according to published study [15]. The exclusion criteria were as follows: repeated admission, ICU stay time less than 24 h and patients with missing data. One of the authors (QH) had been given permission to extract data from this database after completing the database usage examination (ID: 49872601). Due to the relatively large number of missing data for lactate and albumin, we divided screening process into two portions for more clearly as shown in Fig. 1. Data from MIMIC-IV are publicly available, thus this study was exempted by the ethics committee of the First People’s Hospital of Changzhou.
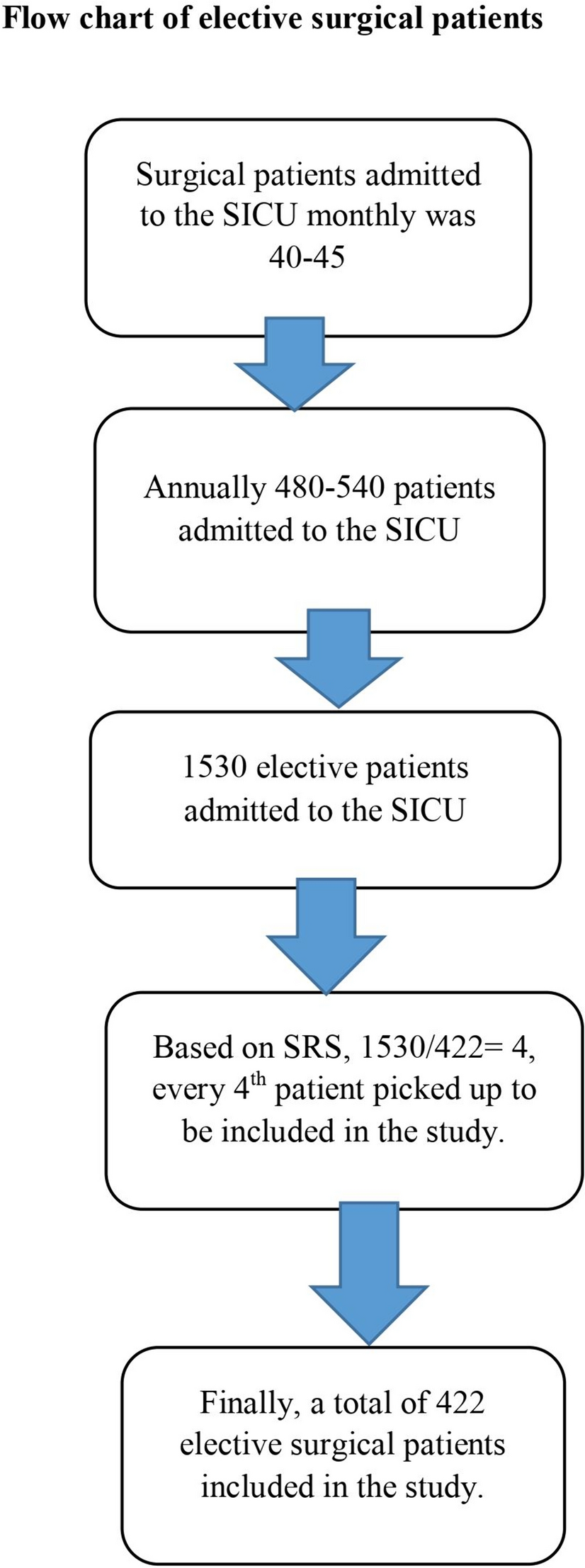
Fig. 1
The flowchart of the screening process. A Initial screening. B Final screening
Variable extractionInformation, including demographic (age, gender), first-day severity of illness [sequential organ failure assessment (SOFA), Oxford Acute Severity of Illness (OASIS), Glasgow coma scale (GCS)], comorbidities (myocardial infarct, congestive heart failure, diabetes, renal disease, malignant cancer, delirium, sepsis, tobacco status), first-day laboratory tests [arterial blood gases (pH, arterial carbon dioxide tension, arterial oxygen tension, base excess), white blood cell, platelet, red blood cell distribution width, hematocrit, hemoglobin, creatinine, glucose, potassium, sodium, lactate, and albumin], first-day vital signs (hear rate, respiratory rate, mean arterial blood pressure, SpO2), status of mechanical ventilation, survival time were obtained. If patients had multiple measurements for some variables at first day on ICU admission, only the first value was used. Distribution normality was evaluated using Shapiro–Wilk normality test. Continuous variables were described as means and standard or median (25th–75th percentile), and categorical variables as proportions. The main outcome was defined as 28-day mortality after ICU admission.
Statistical analysisDifferences between different groups in baseline data analysis were compared using t-test or Wilcoxon rank-sum test for continuous variables, and the chi-square test for categorical variables. The receiver operating characteristic (ROC) curves were used to predictive analysis and identify cut-off values, and the area under the ROC curve (AUC) was calculated. According to cutoff value of LAR, patients were divided into high LAR and low LAR. Significance of survival analysis was performed by K–M curve with log-rank test. Univariate and multivariate logistic regression models were performed to explore the relationship between LAR and 28-day mortality in AECOPD patients. Factors with a p-value of less than 0.05 in the univariate analysis were entered in the multivariate analysis. Stratified and interaction analyses were applied to investigate whether LAR had any effect in different comorbidities.
All data were extracted by Navicat Premium 16.1.3 software. Statistical analysis was performed using R language. P-value < 0.05 was considered as statistically significant.
留言 (0)