
記住我

Infectious etiologies account for a substantial portion of uveitis in the United States and as much as one of three cases in tertiary referral centers.1 Polymerase chain reaction (PCR) is a sensitive and specific test that detects the presence of pathogenic DNA, and the use of this diagnostic modality has greatly improved clinicians' ability to identify and treat intraocular infections.2 In many cases, multiple PCR tests are performed on the same sample,2–7 which creates the potential for multiple positive results. Such occurrences have been reported, but the nature, extent, and effect of multiple simultaneously positive PCR samples in patients with panuveitis has not been extensively described in the literature. This study aimed to determine the rate of intraocular coinfections and characterize the clinical entity.
MethodsThe approval of the University of Miami Institutional Review Board was obtained before conducting this retrospective case study, which was performed in accordance with the Health Insurance Portability and Accountability Act of 1996 and adhered to the tenets of the Declaration of Helsinki. Testing logs of the Bascom Palmer Eye Institute Clinical Microbiology Laboratory were reviewed. Inclusion criteria was defined as patients undergoing diagnostic PCR testing of intraocular fluid between November 1, 2001 and December 31, 2021. All intraocular samples were obtained in various clinical settings at the Bascom Palmer Eye Institute, including the emergency room, outpatient clinic, and operating room as standard of care. Exclusion criteria included samples with a final PCR result for only a single pathogen, samples from external ocular tissues such as cornea, lid, or conjunctiva, and samples in which additional infections were proved by methods other than PCR. Coinfection was defined as a single intraocular sample from a specific date with more than one positive PCR result. Pathogen results were reported in a binary qualitative manner, indicating a pathogen was either present or absent in the sampled fluid. Patient charts were reviewed and included in the study if clinical history and presentation were consistent with the Standardization of Uveitis Nomenclature's criteria for panuveitis. All patients had inflammation present in the anterior chamber, vitreous, and signs of retinal or choroidal lesions either on physical examination or on multimodal imaging. The instances of coinfection were recorded, and the available patient charts were reviewed to determine patient characteristics, specimen source, and patient clinical course. Although not every sample was tested for every pathogen, pathogens for which PCR analysis were ordered included: cytomegalovirus (CMV), Epstein–Barr virus (EBV), varicella zoster virus (VZV), Toxoplasma gondii, herpes simplex virus 1 (HSV-1), herpes simplex virus 2 (HSV-2), and Toxocara. Statistical analyses were performed using GraphPad Prism software. Descriptive statistics were used for patient characteristics and outcomes. Population values were reported as the mean, SD, percentage, or range. Best-corrected visual acuity was converted to logarithm of the minimum angle of resolution (logMAR) for statistical analysis. Counting fingers (CF), hand motion (HM), light perception (LP), and no light perception (NLP) were given values of 1.9, 2.3, 2.7, and 3.0, respectively. Two-tailed Student t-test were used for statistical analysis to compare mean values of patients' visual acuities.
ResultsIn total, 1,588 intraocular samples met inclusion criteria. Of these, 28 samples (1.76%) had more than one positive PCR test result. Eighty-two percent (n = 23) of patients underwent sampling of the aqueous fluid for PCR analysis, and 18% (n = 5) underwent diagnostic vitrectomy in the operating room. No samples were positive for more than two pathogens.
Pathogens identified in coinfection included CMV (n = 16, 57.1%), EBV (n = 13, 46.4%), VZV (n = 8, 28.6%), T. gondii (n = 6, 21.4%), HSV-2 (n = 6, 21.4%), HSV-1 (n = 6, 21.4%), and Toxocara (n = 1, 3.6%). Of the combinations, 26 of 28 (92%) samples included CMV, EBV, or both (3 samples positive for both CMV and EBV). The remaining 2 of the 28 samples (7.1%) that were not positive for CMV or EBV were positive for the combinations of HSV-1/HSV-2 and HSV-1/T. gondii, respectively. All permutations of infectious pathogens and the number of individual occurrences are listed in Table 1.
Table 1. - Frequency of Pathogen Involvement in Coinfection Pathogen (n) HSV-1 HSV-2 CMV VZV EBV T. gondii Toxocara HSV-1 1 3 0 1 1 0 HSV-2 2 0 3 0 0 CMV 5 3 2 1 VZV 3 0 0 EBV 3 0 T. gondii 0 Toxocara Pathogen (n, % of cases) CMV 16 57.1 EBV 13 46.4 VZV 8 28.6 T. gondii 6 21.4 HSV-2 6 21.4 HSV-1 6 21.4 Toxocara 1 3.6The mean age at the time of PCR testing was 47 years (n = 28, SD 17.9, range of 8–85 years), and a majority of patients were male (n = 18, 64.3%). Of the 28 samples identified from 28 patients, charts from 26 patients were retrievable and clinical data were reviewed.
Most patients were immunocompromised (n = 17, 65.4%). The etiology of their immunocompromised state consisted of HIV infection (n = 12, 46.2%), pharmacologic immunosuppression from systemic steroid and/or immunomodulatory therapy (n = 3, 11.5%), and a history of lymphoma (n = 2, 7.7%). Of the patients on pharmacologic immunosuppression, one patient was on chronic prednisone for treatment of rheumatoid arthritis and two patients were on chronic tacrolimus and mycophenolate after undergoing kidney transplant.
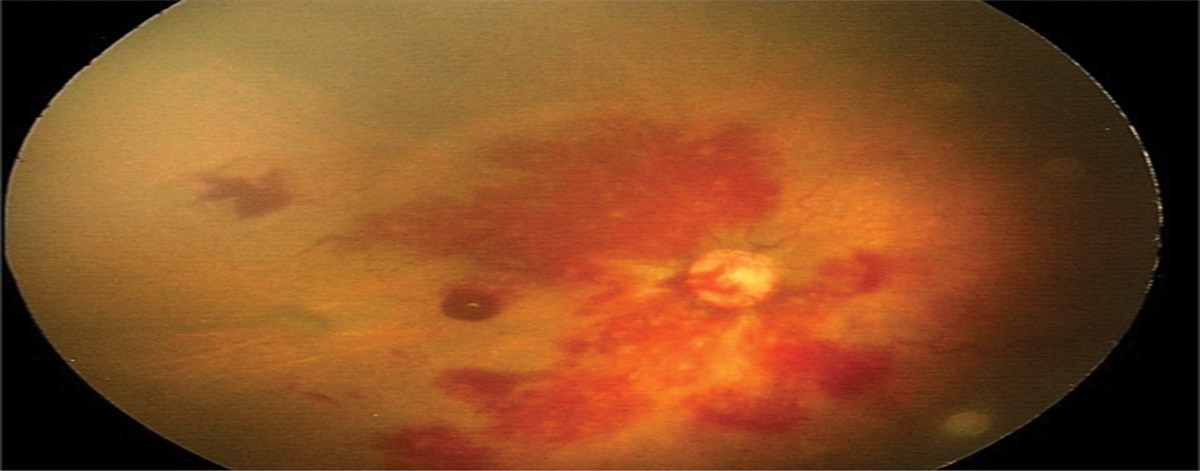
Panuveitis was present in 100% (n = 26) of patients based on Standardization of Uveitis Nomenclature's criteria. Intraocular inflammation (both anterior and vitreous) was the most common clinical feature and was present in 100% (n = 26) of examinations at the time of diagnosis. This was followed by visible retinal whitening consistent with retinitis at presentation (n = 22, 84.6%). Two patients (7.7%) without visible retinal whitening had chorioretinal lesions thought to be related to active inflammation. Two patients (7.7%) had no view of the fundus because of anterior chamber and vitreous inflammation. However, the first patient had a documented history of recent retinal vasculitis, meeting the Standardization of Uveitis Nomenclature's criteria for panuveitis. The second patient had a confirmed retinal detachment (RD) on B-scan ultrasonography. Although RD is not described in the Standardization of Uveitis Nomenclature's criteria, given the clinical history and confirmed PCR positivity of both EBV and HSV-2, best clinical judgement was used by the observer to assume that the RD was likely secondary to an underlying panuveitic process with a viral etiology. Intraretinal hemorrhage at presentation and RD during the clinical course were also prominent features present in 38.5% (n = 10) and 34.6% (n = 9) of patients, respectively (Table 2). Of the nine patients with a RD identified, 3 (33%) were present on the initial presentation and six were diagnosed at a subsequent follow-up visit with a mean time of 130 ± 93 days from the time of initial visit.
Table 2. - Patient Characteristics and Clinical Course for Coinfections Sex (n, %) Male 18 64.3 Female 10 35.7 Age (years) Mean 46.9 ± 17.9 Range 8–85 PCR sample fluid (n, %) Anterior chamber 23 82 Vitreous 5 18 Immune status (n, %) Immunocompromised 17 65.4 HIV 12 46.2 Pharmacologic suppression 3 11.5 Lymphoma 2 7.7 No known immune compromise 9 34.6 Initial visual acuity (n = 26) Mean (logMAR, Snellen) 1.3 ± 0.9 20/400 Worse than 20/40 84.6% 20/200 or worse 53.8% CF or worse 42.3% Initial examination (n, %) Intraocular inflammation* 26 100 Retinal whitening 22 84.6 Retinal hemorrhage 10 38.5 Retinal detachment 9 34.6 Final visual acuity (n = 26) Mean (logMAR, Snellen) 1.3 ± 1.1 20/400 Worse than 20/40 61.5% 20/200 or worse 53.8% CF or worse 46.2%*Indicated by presence of cell reaction in the aqueous and vitreous.
Three patients (11.5%) presented with bilateral panuveitis at the initial visit. All three patients had some form of immunocompromise. The first patient had a history of HIV with a last CD4 count of seven and was positive for both VZV and EBV with signs of optic nerve enhancement on MRI in the studied eye. The fellow eye's ocular fluid was sampled but was only positive for VZV. The second patient had a history of lymphoma, and the studied eye was positive for CMV and HSV-1. The fellow eye was not sampled for PCR testing during the clinical course. The third patient had a history of HIV with a last CD4 count of 46 and positive ocular fluid of the studied eye for CMV and T. gondii. The fellow eye was tested as well, but no pathogens were identified. Of note, after resolution of this patient's active retinitis, EBV-positive (confirmed by biopsy of brain mass) central nervous system (CNS) lymphoma was subsequently diagnosed and treated with high-dose methotrexate, rituximab, and cytarabine, leading to remission of the neoplasm. The ocular fluid was never tested for EBV for this patient.
The mean visual acuity (logMAR) in the affected eye of patients at presentation was 1.3 (n = 26, SD = 0.9, Snellen ∼20/400). Final recorded mean visual acuity was 1.3 (n = 26, SD = 1.1, Snellen ∼20/400). Severe visual impairment was common at the final follow-up because 53.8% had 20/200 or worse vision and 46.2% with counting fingers or worse vision. The mean follow-up time was 2.33 ± 3.75 years (Table 2).
The most common combination was CMV/VZV, which was present in samples from five patients. Cytomegalovirus/HSV-1, CMV/EBV, HSV-2/EBV, VZV/EBV, and toxoplasmosis/EBV were each found in ocular fluid from three patients. Comparing the final visual acuity in these most prevalent subgroups (all combinations with three or more occurrences), patients who were CMV-positive had better visual acuity outcomes (Table 3).
Table 3. - Final Visual Acuities for the Most Common Coinfections Pathogens Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 CMV/VZV NLP NLP 20/2000 20/30 20/30 CMV/HSV-1 20/400 20/200 20/40 CMV/EBV 20/80 20/25 20/20 HSV-2/EBV NLP NLP HM VZV/EBV HM CF 20/4,000 T. gondii/EBV LP 20/1,000 20/800Patients with coinfection with ocular fluid that was CMV-positive overall had better visual outcomes compared with patients with CMV-negative samples. CMV-positive patients had a mean initial visual acuity of 1.12 (n = 16, SD = 0.9, Snellen ∼20/265), whereas the CMV-negative patients had a mean initial visual acuity of 1.70 (n = 10, SD = 0.9, Snellen ∼20/1,000). CMV-positive patients had a mean final visual acuity of 0.94 (n = 16, SD = 1.1, Snellen ∼20/175), whereas the CMV-negative patients had a mean final visual acuity of 1.82 (n = 10, SD = 1.0, Snellen ∼20/1,320) (Table 4). The final visual acuity between the two groups were statistically significant (P < 0.05). A majority of the CMV-negative patients were EBV positive (n = 10, 83.3%). Of the two CMV-negative and EBV-negative patients, one was positive for HSV-1/HSV-2 with no clinically recorded visual acuity at the initial and the final visit. A second patient was positive for HSV-1/T. gondii and was treated with clindamycin and trimethoprim/sulfamethoxazole, with good visual recovery to 20/20 at the last clinic visit. Three patients who were positive for both CMV and EBV had a final visual acuity of 20/20, 20/25, and 20/80, respectively (Table 3). Of the CMV-positive patients, 81.3% received intravitreal foscarnet and ganciclovir during their clinical course, 93.8% received systemic (oral or intravenous) induction treatment with either valganciclovir or valacyclovir/acyclovir, and 100% received either local intravitreal injection or oral antivirals. In total, 68.8% of CMV-positive patients received both intravitreal and systemic antiviral induction therapy simultaneously. Of the CMV-negative patients, although 70% of patients (n = 7) received systemic induction treatment with antivirals, only one patient (10%) received intravitreal antiviral therapy in which the same one patient received both concurrent intravitreal and systemic antivirals (Table 4).
Table 4. - CMV-Positive Versus CMV-Negative Coinfection Patient Characteristics CMV-Positive (n = 16) CMV-Negative (n = 10) P Initial VA mean in logMAR (SD) 1.12 (0.9) 1.71 (0.9) >0.05 Final VA mean in logMAR (SD) 0.94 (1.1) 1.82 (1.0) <0.05 Intravitreal foscarnet/ganciclovir 81.30% 10% Induction with oral or intravenous antivirals 93.8% 70% Both oral/intravenous and intravitreal antivirals 68.8% 10% Immunocompromised 69% 50% Retinal detachment 31.30% 40%Five patients received only treatment thought to be effective for one of the two pathogens identified on PCR. Of these five patients, one patient was positive for CMV and T. gondii, received treatment for only CMV, and resulted in decline of vision from 20/25 to 20/30. Another patient was positive for CMV and Toxocara, was treated for only CMV, and had improvement of vision from counting fingers to 20/60. Two patients were positive for EBV and T. gondii and both were treated only for T. gondii. Both had an initial visual acuity of counting fingers, and one remained counting fingers, whereas the other declined to light perception at the final follow-up. One patient was positive for HSV-1 and T. gondii, was only treated for T. gondii, and had vision improve from 20/50 to 20/20 (Table 5).
Table 5. - Patients Receiving Treatment Targeted for Only One Pathogen in Coinfections Pathogen Combination Treatment VA Initial (logMAR) Initial VA (Snellen Equiv.) VA Final (logMAR) Final VA (Snellen Equiv.) CMV/Toxoplasma gondii Oral valgancyclovir + intravitreal foscarnet/ganciclovir 0.09 20/25 0.176 20/30 CMV/toxocara Oral valgancyclovir + intravitreal foscarnet/ganciclovir 1.9 CF 0.48 20/60 EBV/T. gondii Pyramethamine, sulfadiazine 1.9 CF 1.9 CF EBV/T. gondii Clindamycin, trimethoprim–sulfamethoxazole 1.9 CF 2.7 LP HSV-1/T. gondii Clindamycin, trimethoprim–sulfamethoxazole 0.4 20/50 0 20/20Polymerase chain reaction has become a crucial part of diagnosing infectious uveitis, and the precision enabled by this test has allowed clinicians to identify multiple, simultaneous pathogens. The current case series is unique in that it is the largest collection of intraocular coinfections reported in the literature. Coinfections occurred over a wide range of ages and involved 12 distinct combinations of pathogens. Although these events are rare and are not homogenous, there were several unifying characteristics. Intraocular inflammation along with retinal involvement was noted at presentation in most of the patients. Immunocompromise was very common, and of those who were “immunocompetent,” some had risk factors for relative immune system compromise such as age >80 years and end-stage renal disease. Finally, the risk of vision loss in these patients is extremely high with a significant portion of patients becoming legally blind as a result. Although some pathogen combinations were detected multiple times, not all combinations of pathogens occurred. Conversely, except for two, all samples included either CMV or EBV, suggesting that these pathogens are involved in coinfection not as a result of random chance. Rather the interaction between the two pathogens and the host likely makes certain combinations and pathogens more likely to be present in coinfection.
Coinfections have been extensively described in other areas of medicine. Synergistic, inhibitory, and null interactions have all been demonstrated. For example, in the liver, coinfection with hepatitis B virus and hepatitis D virus synergistically leads to a more virulent infection than either alone.8 Similarly, in patients with Pneumocystis pneumonia, either aspergillosis or CMV coinfection is associated with increased mortality.9 Conversely, coinfection by respiratory syncytial virus and influenza A virus in the respiratory tract seems to lead to an inhibitory effect where the clinical presentation is attenuated compared with either individual virus alone.10 In the current study, the effect of multiple intraocular pathogens on the clinical presentation and course may have an association with the specific pathogens involved. Patients with a combination of EBV and CMV had a relatively good visual prognosis (range: 20/20, 20/25–20/80). This is impressive considering other studies of CMV retinitis report poor final visual acuity (20/200 or worse) in approximately 15% to 40%.11,12 None of the patients with CMV/EBV coinfection experienced this level of ocular morbidity (Table 3).
Overall, the initial and the final visual acuity of CMV-positive patients were more favorable than the CMV-negative patients. One reason for this may be the predictability and availability of known effective antivirals for CMV-related retinitis,13,14 which typically consists of systemic antivirals along with supplemental intravitreal antivirals.15 In our cohort of CMV-positive patients, a majority received local injections of intravitreal foscarnet/ganciclovir, oral induction treatment with valganciclovir/valacyclovir/acyclovir, or both. A majority of the second pathogens in the CMV-positive patients were also viruses (e.g., HSV-1, HSV-2, and VZV) that have demonstrated consistent susceptibility to antivirals used to treat CMV. Therefore, the same antiviral therapy would theoretically cover both pathogens. Patients with second pathogens that were not viruses (e.g., Toxoplasma) were treated as clinically indicated with appropriate medical therapy if there was a clinical suspicion for the second pathogen based on examination and imaging. Five of our patients were only treated for one pathogen, with variable effects on final visual acuity.
In contrast, final visual acuities of the CMV-negative patients were worse compared with the CMV-positive patients. Of the 12 CMV-negative patients, 10 were positive for EBV and an additional pathogen, with the final mean visual acuity being CF. One hypothesis for the poor visual outcomes in this subset of patients may be the interaction between EBV and the second pathogen. For example, the combination T. gondii/EBV seemed to produce a more virulent infection than T. gondii alone. All three of the coinfection cases with T. gondii/EBV had vision worse than 20/200, whereas only approximately 17% to 35% of patients with ocular toxoplasmosis from previous studies experienced that level of vision loss.16–18
Epstein–Barr virus is a common virus and is seropositive in approximately 90% to 95% of the population by the age of 25 years.19 The pathogenicity of detected EBV, along with any other pathogen that was identified, is difficult to definitively discern given no functional studies were performed, and there is a possibility that there may be circulating lymphocytes introduced from systemic circulation in the setting of severe intraocular inflammation. Although a rarely reported condition, EBV-associated retinitis generally portends a poor visual outcome,20 likely because there is no data-driven, clinically approved medical treatment for EBV. Several articles have reported that EBV can be the sole pathogen causing necrotizing retinitis,2,21–26 and EBV has rarely been reported with simultaneous infection with a second pathogen.5 Attempted treatments in these studies included systemic and/or intravitreal antivirals, with two cases using intravitreal methotrexate,21,26 all with variable outcomes in visual acuity. In our series, EBV was not treated consistently with one antiviral. Rather, the choice of therapy was dependent on the second pathogen (e.g., CMV/EBV was treated with valganciclovir, HSV-1/EBV with acyclovir, or T gondii/EBV with trimethoprim/sulfamethoxazole).
Many cases of co-infection present initially with panuveitis and distinct retinitis on examination, but may take several days to weeks to obtain confirmation of pathogens present on ocular fluid sampling. In our institutional practice, patients with undifferentiated panuveitis with active retinitis undergo empirical treatment with valacyclovir at treatment dose for viral retinitis, along with serial intravitreal foscarnet/ganciclovir and oral trimethoprim–sulfamethoxazole (to cover for potential toxoplasmosis), until the results of the PCR have resulted. Given the high rate of poor final visual acuity in the study cohort, PCR-guided treatment is advised for both pathogens. If the pathogens include CMV, valganciclovir treatment may be substituted for valacyclovir given its greater efficacy toward CMV while still effective against other viruses such as HSV and VZV. If toxoplasmosis is present along with another virus, treatment for both pathogens is recommended. In the presence of EBV, systemic and local antivirals may be considered. However, there is no data-driven therapeutic that is effective against EBV.
The direction of the association with EBV in the intraocular setting remains unclear: does EBV create a milieu that promotes a second infectious agent or does an initial infection permit latent EBV to reactivate? EBV is known to produce a viral homolog of IL-10 that seems to alter the natural immune response, contributing to EBV's chronic infection.27 When present intraocularly, mechanisms that permit EBV's latency may make other infections more likely. Alternatively, some have speculated that local reactivation of the virus from B cells or retinal pigment epithelium cells may occur in cases of immunosuppression28 or exuberant inflammation.29
Cytomegalovirus and EBV may be two of many pathogens closely linked to coinfection, and such knowledge could lead to a more nuanced understanding of the pathogenesis of infectious uveitis that we currently attribute to one, unprovoked agent. Although the rarity of these events makes this compilation valuable, the small sample size limits the ability to draw definitive conclusions about particular combinations of pathogens and how to treat them. Additionally, the PCR was qualitative rather than quantitative, so the relative predominance of either pathogen could not be discerned. Newer diagnostic tools such as metagenomic next-generation sequencing have demonstrated high sensitivity in identifying the presence of multiple concurrent pathogens and may be a powerful approach in the clinical setting, especially as newer technologies such as nanopore sequencing can acquire real-time genomic results within hours of sample submission.30,31
Because of its retrospective nature, this study only describes the practice patterns as they currently stand. A prospective study would be particularly useful when considering treatment options for specific coinfections.
Although previously noted in the literature, this is the first large series of PCR-proven intraocular coinfections. These coinfections depend on the sensitivity and specificity of PCR for diagnosis, and a high index of suspicion is required to uncover these cases. Given the data presented here, the possibility of simultaneous infections must be considered in cases of immune system compromise, severe retinitis, or any time CMV or EBV are detected intraocularly.
References 1. Lin P. Infectious uveitis. Curr Ophthalmol Rep 2015;3:170–183. 2. Harper TW, Miller D, Schiffman JC, Davis JL. Polymerase chain reaction analysis of aqueous and vitreous specimens in the diagnosis of posterior segment infectious uveitis. Am J Ophthalmol 2009;147:140–147.e2. 3. Sugita S, Shimizu N, Watanabe K, et al. Use of multiplex PCR and real-time PCR to detect human herpes virus genome in ocular fluids of patients with uveitis. Br J Ophthalmol 2008;92:928–932. 4. de-la-Torre A, Valdés-Camacho J, de Mesa CL, et al. Coinfections and differential diagnosis in immunocompetent patients with uveitis of infectious origin. BMC Infect Dis 2019;19:91. 5. Sato T, Kitamura R, Kaburaki T, Takeuchi M. Retinitis associated with double infection of Epstein-Barr virus and varicella-zoster virus: a case report. Medicine (Baltimore) 2018;97:e11663. 6. Chen S, Malik KJ, Shen D, Chan C-C. Acute retinal necrosis with multiple viral infections: a case report. Int J Ophthalmic Pathol 2014;3:1000151. 7. Nakamura T, Daikoku T, Shiraki K, Hayashi A. Detection of cytomegalovirus in an immunocompetent adult presenting with acute retinal necrosis due to varicella-zoster virus: a case report. Clin Ophthalmol 2015;9:853–858. 8. Smedile A, Farci P, Verme G, et al. Influence of delta infection on severity of hepatitis B. Lancet 1982;2:945–947. 9. Boonsarngsuk V, Sirilak S, Kiatboonsri S. Acute respiratory failure due to Pneumocystis pneumonia: outcome and prognostic factors. Int J Infect Dis 2009;13:59–66. 10. Pinky L, Dobrovolny HM. Coinfections of the respiratory tract: viral competition for resources. PLoS One 2016;11:e0155589. 11. Kuo IC, Kempen JH, Dunn JP, et al. Clinical characteristics and outcomes of cytomegalovirus retinitis in persons without human immunodeficiency virus infection. Am J Ophthalmol 2004;138:338–346. 12. Jabs DA, Ahuja A, Van Natta ML, et al. Long-term outcomes of cytomegalovirus retinitis in the era of modern antiretroviral therapy: results from a United States cohort. Ophthalmology 2015;122:1452–1463. 13. Stewart MW. Optimal management of cytomegalovirus retinitis in patients with AIDS. Clin Ophthalmol 2010;4:285–299. 14. Port AD, Orlin A, Kiss S, et al. Cytomegalovirus retinitis: a review. J Ocul Pharmacol Ther 2017;33:224–234. 15. Foscarnet-Ganciclovir Cytomegalovirus Retinitis Trial. 4. Visual outcomes. Studies of Ocular Complications of AIDS Research Group in collaboration with the AIDS Clinical Trials Group. Ophthalmology 1994;101:1250–1261. 16. Bosch-Driessen LEH, Berendschot TTJM, Ongkosuwito JV, Rothova A. Ocular toxoplasmosis: clinical features and prognosis of 154 patients. Ophthalmology 2002;109:869–878. 17. Aleixo ALQdC, Curi ALL, Benchimol EI, Amendoeira MRR. Toxoplasmic Retinochoroiditis: clinical characteristics and visual outcome in a prospective study. PLoS Negl Trop Dis 2016;10:e0004685. 18. Arruda S, Vieira BR, Garcia DM, et al. Clinical manifestations and visual outcomes associated with ocular toxoplasmosis in a Brazilian population. Sci Rep 2021;11:3137. 19. Winter JR, Jackson C, Lewis JE, et al. Predictors of Epstein-Barr virus serostatus and implications for vaccine policy: a systematic review of the literature. J Glob Health 2020;10:010404. 20. Suzuki K, Namba K, Hase K, et al. A case of Epstein-Barr virus acute retinal necrosis successfully treated with foscarnet. Am J Ophthalmol Case Rep 2022;25:101363. 21. Cho J, Bhavsar AR, Cho DH, et al. Successful treatment of Epstein-Barr virus-induced necrotizing retinitis with intravitreous ganciclovir, foscarnet, and methotrexate. Case Rep Ophthalmol 2022;13:116–123. 22. Hamam RN, Mansour A, El Mollayess G. Positive Epstein-Barr virus polymerase chain reaction in a case of acute retinal necrosis. Can J Ophthalmol 2012;47:e61–e62. 23. Schaal S, Kagan A, Wang Y, et al. Acute retinal necrosis associated with Epstein-Barr virus: immunohistopathologic confirmation. JAMA Ophthalmol 2014;132:881–882. 24. Oe C, Hiraoka M, Tanaka S, Ohguro H. Acute retinal necrosis associated with Epstein-Barr virus in a patient undergoing immunosuppressive therapy. Case Rep Ophthalmol 2016;7:195–201. 25. Chan EW, Sun V, Eldeeb M, Kapusta MA. Epstein-Barr virus acute retinal necrosis in an immunocompetent host. Retin Cases Brief Rep 2021;15:412–416. 26. Mashima A, Usui Y, Umazume K, et al. Successful treatment of necrotizing retinitis with Epstein-Barr virus-positive ocular fluid by intravitreal methotrexate injection. Ocul Immunol Inflamm 2020;28:552–555. 27. Jog NR, Chakravarty EF, Guthridge JM, James JA. Epstein-Barr virus interleukin 10 suppresses anti-inflammatory phenotype in human monocytes. Front Immunol 2018;9:2198. 28. Ongkosuwito JV, Van der Lelij A, Bruinenberg M, et al. Increased presence of Epstein-Barr virus DNA in ocular fluid samples from HIV negative immunocompromised patients with uveitis. Br J Ophthalmol 1998;82:245–251. 29. Yamamoto S, Sugita S, Sugamoto Y, et al. Quantitative PCR for the detection of genomic DNA of Epstein-Barr virus in ocular fluids of patients with uveitis. Jpn J Ophthalmol 2008;52:463–467. 30. Lee AY, Akileswaran L, Tibbetts MD, et al. Identification of torque teno virus in culture-negative endophthalmitis by representational deep DNA sequencing. Ophthalmology 2015;122:524–530. 31. Li X, Li Z, Wang M, et al. The diagnostic utility of nanopore targeted sequencing in suspected endophthalmitis. Int Ophthalmol 2023;43:2653–2668.
留言 (0)