The current landscape for diabetes treatment: Preventing diabetes-associated CV risk
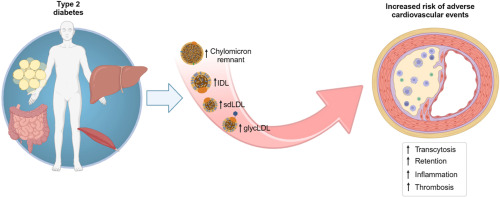
Atherosclerosis is a progressive, chronic inflammatory disease with an immune component characterized by accumulation of lipids, complex carbohydrates, blood products, fibrous elements, and calcium deposits in the intima/media of the arterial wall (1). Atherogenesis represents a continuum that initiates with the activation and dysfunction of the endothelium to progress toward the formation of stable and unstable plaques (1). Atherosclerotic cardiovascular disease (ASCVD) affects coronary arteries causing acute coronary syndrome, stable or unstable angina, and myocardial infarction; carotid arteries causing stroke, and peripheral arteries accounting for the majority of lower limb amputations. ASCVD accounts for two-thirds of cardiovascular (CV) disease and death worldwide (2). The process is even more common in people with type 2 diabetes (T2DM) in whom atherosclerosis typically develops earlier, with greater severity, and with more diffuse distribution as compared with individuals without diabetes. About one third of T2DM people have CV disease, and in 9 out of 10 of them the disease is of atherosclerotic nature (3) (Figure 1). Many factors concur to increase the risk of atherosclerosis in both diabetic and non-diabetic individuals (4) and multifactorial intervention remains the basis for effective prevention or mitigation of ASCVD. In people with T2DM, hyperglycemia has represented the initial therapeutic target to reduce CV risk, an approach initially addressed in the United Kingdom Prospective Diabetes Study (UKPDS) (5). In that seminal trial, “intensive” treatment attaining an average HbA1c of 7.0% in newly diagnosed T2DM people with no history of prior CV events was associated with a 16% risk reduction of myocardial infarction, though it did not reach statistical significance (p=0.052). This uncertain result triggered, amid much ignited discussions, new intervention trials (6) aiming at achieving an even stricter glycemic control (Figure 2). Yet, despite much effort and the attainment of average HbA1c levels well below 7% no CV benefit became apparent. Many reasons account for these frustrating results (6), but the most obvious one is that tackling chronic hyperglycemia in the context of multiple factors contributing to atherogenesis is unlikely to provide significant protection. This view is well supported by the results of the Steno 2 trial (7). In a small but carefully selected group of T2DM subjects, multifactorial treatment aiming to improve glucose level, blood pressure, lipid profile with concomitant use of an antiaggregant therapy yielded, over a mean follow-up of 7.8 years, a 53% relative risk reduction of cardiovascular disease. Subsequent analyses showed that the contribution of glycemic control was minimal as compared to the protective effect of controlling blood pressure and reducing LDL-cholesterol levels (8).
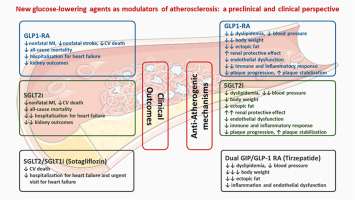
The early intervention trials were largely based on an old pharmacologic armamentarium mainly consisting of metformin, sulfonylureas, glitazones, and insulin 5, 6. The CV protective effect of metformin is still a matter of debate and many doubts about the CV safety of sulfonylureas (9) and insulin (10) have been raised over the years. Thiazolidinediones did generate some expectation due to their potent anti-inflammatory effect (11). In the PROactive trial, although the primary endpoint was not met, the main secondary endpoint (composite of all-cause mortality, non-fatal myocardial infarction, and stroke) was reached (HR 0.84, 95% CI 0.72-0.98; p=0.027) (12). In the meantime, new pharmacologic agents were introduced in the diabetes pharmacopeia. All these new agents, namely dipeptidyl peptidase 4 inhibitors (DPP4i), glucagon-like peptide-1 receptor agonists (GLP1-RA) and sodium-glucose cotransporter 2 inhibitors (SGLT2i), had to be tested in post-marketing CV outcome studies (CVOTs) (Figure 3) that have revolutionized current treatment of T2DM and offered an unprecedented opportunity to reduce atherosclerotic risk in these individuals.



留言 (0)