
記住我



Available online 20 April 2024, 117556
 Author links open overlay panel, , Highlights•
Author links open overlay panel, , Highlights•Absolute mass changes in remnant cholesterol, LDL cholesterol, and apo B can explain results of the PROMINENT trial.
•To reduce ASCVD lipid lowering drugs need to reduce total atherogenic cholesterol and total number of atherogenic particles.
•Understanding the potential for causing ASCVD, lipoproteins should be judged by their absolute mass of cholesterol content.
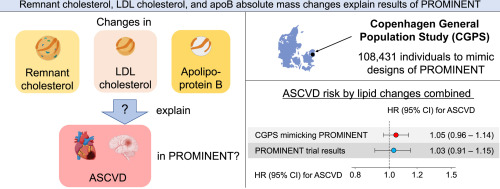
Abstract:Background and aimsThe PROMINENT trial, a cardiovascular outcome trial of the triglyceride- and remnant cholesterol-lowering agent pemafibrate, has shown neutral results despite reduction in plasma triglycerides and remnant cholesterol. We tested the hypothesis that absolute mass changes in remnant cholesterol, LDL cholesterol, and apolipoprotein B explain the results of the PROMINENT trial.
MethodsAmong 108,431 individuals from the Copenhagen General Population Study (CGPS), those who met the key inclusion criteria of the PROMINENT trial were analyzed to mimic the trial design. The endpoint atherosclerotic cardiovascular disease (ASCVD) was cardiovascular death, myocardial infarction, ischemic stroke, and coronary revascularization as defined in PROMINENT.
ResultsIn the PROMINENT trial, treatment with pemafibrate resulted in -7mg/dL (-0.18mmol/L;-18%) change in remnant cholesterol, +10mg/dL (+0.26mmol/L;+12%) LDL cholesterol, and +5mg/dL (+0.05g/L;+5%) apolipoprotein B. In the CGPS mimicking PROMINENT, the estimated hazard ratios for ASCVD were 0.97(95% confidence interval:0.94–0.99) for a -7mg/dL (-0.18mmol/L) change in remnant cholesterol, 1.04(1.01–1.07) for a +10mg/dL (+0.26mmol/L) change in LDL cholesterol, and 1.02(1.01–1.03) for a +5mg/dL (+0.05g/L) change in apolipoprotein B. When combining absolute changes in remnant cholesterol, LDL cholesterol, and apolipoprotein B, the estimated hazard ratio for ASCVD was 1.05(0.96–1.14) in the CGPS mimicking PROMINENT compared to 1.03(0.91–1.15) in the PROMINENT trial.
ConclusionsAbsolute mass changes in remnant cholesterol, LDL cholesterol, and apolipoprotein B can explain results of the PROMINENT trial. The 3mg/dL (0.08mmol/L) higher total atherogenic cholesterol together with 5mg/dL(0.05g/L) higher apolipoprotein B seem to explain the trend toward more ASCVD in the pemafibrate arm.
Section snippetsIntroduction:Randomized double-blind placebo-controlled trials have shown inconsistent results for the effect of fibrates as triglyceride- and remnant cholesterol-lowering agents on prevention of atherosclerotic cardiovascular disease (ASCVD) [1], [2], [3], [4], [5], [6]. Most recently in the PROMINENT (Pemafibrate to Reduce Cardiovascular OutcoMes by Reducing Triglycerides IN patiENts With diabeTes) trial including 10,497 individuals with diabetes, on statins, and at high ASCVD risk, administration of 0.4
Study populationThe Copenhagen General Population Study is a prospective cohort study recruited in 2003–2015, including individuals aged 20–100 years randomly selected from the Danish Civil Registration System (43% participation rate) [15]. Information on lifestyle and medication including statin therapy was obtained through a questionnaire. Furthermore, participants underwent a physical examination and had nonfasting blood samples drawn for lipid profile measurements [16]. We used 108,431 eligible individuals
ResultsIn 108,431 eligible individuals in the CGPS, 2,487 fulfilled the key inclusion criteria for the PROMINENT trial (the CGPS mimicking PROMINENT) (Table 1). In the CGPS, calculated remnant cholesterol was highly positively correlated with directly measured remnant cholesterol (Supplementary Fig. 1).
DiscussionIn individuals fulfilling the key inclusion criteria of the PROMINENT trial (the CGPS mimicking PROMINENT), changes in remnant cholesterol, LDL cholesterol, and apolipoprotein B combined can explain the results of the PROMINENT trial (Figure 5). In the PROMINENT trial, total atherogenic cholesterol increased by 3 mg/dL (+0.08 mmol/L) and total number of atherogenic lipoproteins (marked by apolipoprotein B) increased by 5 mg/dL (+0.05 g/L) in the pemafibrate versus placebo arm, intuitively
Data availabilityThe data underlying this article cannot be shared publicly because the Danish data protection agency does not allow open access. However, on reasonable request, additional analyses can be done after contacting the corresponding author.
Declaration of Competing InterestBGN reports consultancies or talks sponsored by AstraZeneca, Sanofi, Regeneron, Akcea, Amgen, Amarin, Kowa, Denka, Novartis, Novo Nordisk, Esperion, Silence Therapeutics, Abbott, Mankind, Lilly, and Arrowhead. TD reports a consultancy by Novo Nordisk. AL reports a talk sponsored by Amarin and a consultancy by Novartis.
Financial supportThis work was supported by the Capital Region of Denmark [research fund to TD (grant number A7165 and A7272)]; the Department of Clinical Biochemistry, Herlev and Gentofte Hospital, Copenhagen University Hospital, Denmark; and the Japan Society for the Promotion of Science [JSPS: Postdoctoral Fellowship for Research Abroad to TD (grant number 202360405)]. The funders had no direct role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report;
Declaration of Competing Interest☐ The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
☒ The author (Takahito Doi) is an Editorial Board Member for Cardiovascular Intervention and Therapeutics and was not involved in the editorial review or the decision to publish this article.
☒ The authors declare the following financial interests/personal relationships which may be considered as potential competing interests:
Acknowledgments:The authors thank participants and staff of the Copenhagen General Population Study for their invaluable contributions.
References (42)RubinsH.B. et al.Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study GroupN Engl J Med
(1999)
FrickM.H. et al.Helsinki Heart Study: primary-prevention trial with gemfibrozil in middle-aged men with dyslipidemia. Safety of treatment, changes in risk factors, and incidence of coronary heart diseaseN Engl J Med
(1987)
DoiT. et al.Lipoproteins, Cholesterol, and Atherosclerotic Cardiovascular Disease in East Asians and EuropeansJ Atheroscler Thromb
(2023)
NordestgaardB.G. Triglyceride-Rich Lipoproteins and Atherosclerotic Cardiovascular Disease: New Insights From Epidemiology, Genetics, and BiologyCirc Res
(2016)
FerenceB.A. et al.Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus PanelEur Heart J
(2017)
BorenJ. et al.Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European Atherosclerosis Society Consensus PanelEur Heart J
(2020)
GinsbergH.N. et al.Triglyceride-rich lipoproteins and their remnants: metabolic insights, role in atherosclerotic cardiovascular disease, and emerging therapeutic strategies-a consensus statement from the European Atherosclerosis SocietyEur Heart J
(2021)
DoiT. et al.A possible explanation for the contrasting results of REDUCE-IT vs. STRENGTH: cohort study mimicking trial designsEur Heart J
(2021)
DoiT. et al.Mass changes in remnant cholesterol and LDL cholesterol explain part of the results of gemfibrozil and non-gemfibrozil fibrate trialsJ Intern Med
(2024)
NordestgaardB.G. et al.Fasting is not routinely required for determination of a lipid profile: clinical and laboratory implications including flagging at desirable concentration cut-points–a joint consensus statement from the European Atherosclerosis Society and European Federation of Clinical Chemistry and Laboratory MedicineEur Heart J
(2016)
FriedewaldW.T. et al.Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifugeClin Chem
(1972)
View full text© 2024 Published by Elsevier B.V.
留言 (0)