
記住我










An 8-year-old boy presented to the dermatology department with a 2-month history of progressive, patchy alopecia on the scalp. Initially, a small patch of hair loss had been noted, then the patches had started to extend. He was otherwise healthy and taking no medications. On examination, several patches of hair loss distributed over the scalp were noted, with a few visible greyish-white scales (Figure 1A). Wood’s lamp examination showed blue-green fluorescence (Figure 1B). Potassium hydroxide preparation microscopy showed spores and hyphae. We diagnosed tinea capitis based on these findings, which was confirmed by positive fungal culture 2 weeks later. The scales faded and the hair regrew after 6 weeks of empiric treatment with oral itraconazole and topical ketoconazole 2% wash.
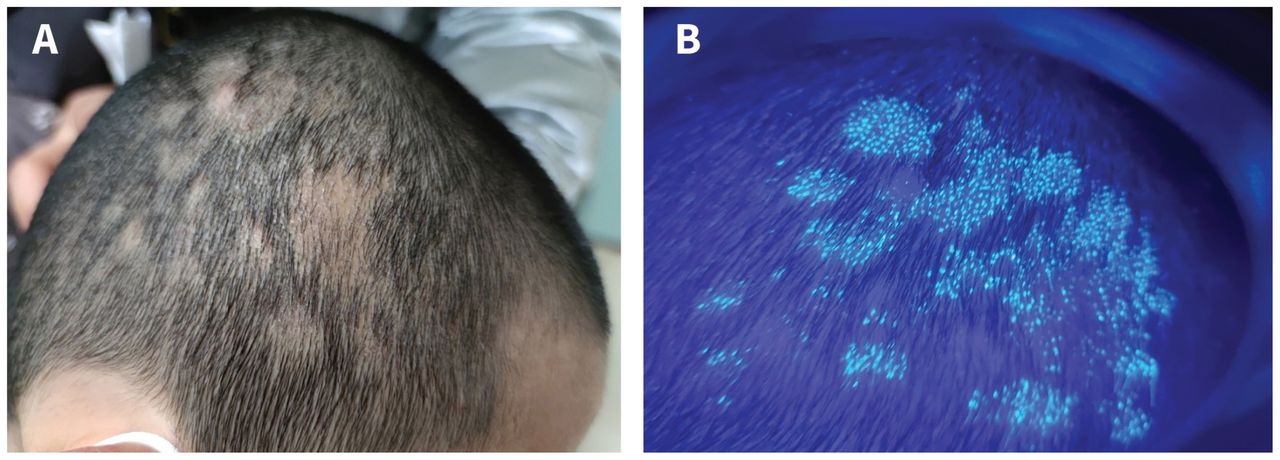 Figure 1:
Figure 1: (A) Patches of alopecia on the scalp of an 8-year-old boy without erythema or papulopustules, and some hair covered with greyish-white scales. (B) Blue-green fluorescence on the hair under Wood’s lamp ultraviolet light examination.
Tinea capitis, or “ringworm,” is a dermatophyte infection that occurs most commonly in children. It is characterized by itchy lesions progressing to alopecia with visible scales on the scalp, and affected children will usually have cervical and suboccipital lymphadenopathy.1 Other clinical manifestations of tinea capitis, such as black dot, kerion, or favus, depend on the type of dermatophyte involved and the degree of host immune response. In North America, noninflammatory tinea capitis is usually caused by Trichophyton tonsurans and Microsporum canis; however, organisms may vary in other parts of the world.2 Wood’s lamp fluorescence can be seen in infections caused by M. canis, but lesions caused by T. tonsurans do not fluoresce.1 Patients with a travel history, those who have recently immigrated, or patients not responding to treatment should have samples sent for fungal cultures to confirm the causative organism.
The differential diagnosis for patchy alopecia includes seborrheic dermatitis, alopecia areata, and trichotillomania.1 Systemic antifungals, such as terbinafine, itraconazole, and fluconazole, are needed to cure tinea capitis, since topical adjuvant therapy has limited penetration into the hair follicles.3 Family members and pets may be sources of infection, and may require simultaneous treatment to prevent recurrence.3
FootnotesCompeting interests: None declared.
This article has been peer reviewed.
The authors have obtained parental consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
留言 (0)